
Abstract
We evaluated the prevalence of serum 25-hydroxyvitamin D [25(OH)D] deficiency and the risk factors for vitamin D deficiency in HIV-infected patients in the South-Central United States. The study consisted of a cross-sectional assessment of vitamin D levels in HIV-infected patients receiving routine clinical care from a private practice in Houston, Texas (latitude 29°N). Vitamin D deficiency was defined as 25(OH)D less than 20 ng/ml (<50 nmol/liter). Two-hundred enrolled patients were surveyed with a vitamin D questionnaire to determine daily supplemental vitamin D intake, dietary vitamin D intake, and average sunlight exposure (minutes/day). Multivariate logistic regression analysis was used to determine significant risk factors for vitamin D deficiency. Median 25(OH)D was 15.5 ng/ml (interquartile range 10.9–24.6) for the total population (n=200). Approximately, two-thirds (64%) of patients had vitamin D deficiency and 20.5% had severe vitamin D deficiency [25(OH)D <10 ng/ml or <25 nmol/liter]. In univariate analysis, African-American race, current tobacco use, increased body mass index (BMI), lower serum calcium level, no supplemental vitamin D use, and low daily supplemental and total daily vitamin D intake were significantly associated with vitamin D deficiency. In multivariate analysis, African-American race [adjusted odds ratio (AOR) 3.53 (95% confidence interval (CI) 1.83–6.82)], higher BMI [AOR 1.07 (95% CI 1.002–1.139)], and low daily vitamin D supplemental intake [AOR 0.997 (95% CI 0.996–0.999)] were significantly associated with vitamin D deficiency. No HIV factors including antiretroviral class use were significantly associated with either vitamin D deficiency or severe vitamin D deficiency. Vitamin D deficiency and severe vitamin D deficiency were highly prevalent in this HIV population. In the HIV population, African-Americans or patients with a high BMI may benefit from vitamin D supplementation.
Introduction
O
Recent studies have also reported high rates (14–74%) of vitamin D deficiency in HIV-infected patients. 15 –26 Some of these studies shared significant independent risk factors for vitamin D deficiency, including darker skin pigmentation or African-American race, current efavirenz use, and nadir CD4 counts less than 200 cells/mm3. 17,19 However, very few of these studies controlled for major confounding factors such as daily dietary vitamin D intake, supplemental vitamin D intake, and sunlight exposure, which could influence vitamin D status in HIV-infected patients.
Therefore, taking these major confounding factors into consideration, the goal of this study was to determine the prevalence and risk factors for vitamin D deficiency in our HIV-infected population in the South-Central United States. Our clinic is located at 29°N, unlike other studies conducted in latitudes greater than 40°N. 15 –26 Finally, we determined whether there were any associations between vitamin D deficiency and antiretroviral class use of nonnucleoside reverse transcriptase inhibitors (NNRTIs) or protease inhibitors (PIs).
Materials and Methods
This cross-sectional cohort study included 200 HIV-infected patients from Therapeutic Concepts, a private practice in Houston, Texas. Patients were eligible for participation if they were at least 18 years of age, had a positive diagnosis of HIV infection, and had a serum 25(OH)D level drawn during a recent clinic visit between October 2008 and March 2009. At this clinic, serum 25(OH)D levels are a routine clinical test. Patients were excluded if they were pregnant or had overt cognitive impairment, chronic renal failure (defined as serum creatinine >1.5 mg/dl), or hepatic dysfunction [defined as AST or ALT ≥5×upper limit of normal (ULN)]. The protocol was approved by the institutional review board at the University of Houston and written consent was obtained from all patients.
Enrolled patients were surveyed with a face-to-face unvalidated vitamin D questionnaire at the same time their vitamin D level was drawn during their clinic visit. The vitamin D questionnaire was composed of three sections: daily supplemental vitamin D intake, daily dietary vitamin D intake (criteria defined by office of dietary supplements 27 ), and daily sunlight exposure (minutes/day). With regards to sunlight exposure, patients were asked “How many minutes (or hours) of direct sunlight are you exposed to on a daily basis (this does NOT include being behind a window, under a canopy, in the shade, etc.)?” Total daily vitamin D intake was defined as the sum of daily dietary and daily supplementary vitamin D intake.
The following relevant information was also collected from patient charts for each patient at the same time the vitamin D level was drawn: patient demographics [age, gender, and body mass index (BMI)], current tobacco use, previous diagnosis of AIDS, and pertinent laboratory markers (CD4 cell count, CD4 percentage, CD8 cell count, HIV viral load, serum calcium, phosphorous, albumin, alkaline phosphatase, AST, ALT, and creatinine clearance calculated by the MDRD method). Corrected calcium was calculated as follows: {serum calcium – [0.025×(albumin)] +1}. In addition, information regarding current antiretroviral and other medication use was collected from each patient. Adherence to current antiretrovirals was assessed by patients' recall of any missed doses in the previous 30 days prior to when their serum 25(OH)D was drawn.
Serum 25(OH)D levels were analyzed by a clinical laboratory (LabCorp) using Diasorin (Stillwater, MN) radioactive immunoassay (RIA) methods. Severe vitamin D deficiency was defined as serum 25(OH)D <10 ng/ml (<25 nmol/liter) vitamin D deficiency as serum 25(OH)D <20 ng/ml (<50nmol/liter) or optimal levels as serum 25(OH)D >30 ng/ml (>75 nmol/liter). 1,17,24 Since vitamin D levels were measured over a 6-month period, seasonality was stratified according to the Fall (from October to December) and Winter (from January to March) months.
SAS software version 9.2 (SAS Institute, Cary, NC) was used for all analyses. We used t-tests for continuous variables and chi-square tests for categorical variables. A p-value less than 0.05 was considered significant for all analyses adjusting for multiple comparisons where appropriate. All p-values were reported as two-sided. Risk factors for vitamin D deficiency were determined by univariate analyses and multivariate logistic regression analysis. Identified variables in the univariate analyses with a p-value less than 0.2 were included in the multivariate analysis regression models after assessing colinearity and backward selection was used to arrive at the final model.
Results
Patients
Among the 200 patients enrolled, 49% were African-American, 40% white, 9% Hispanic, and 76% male. The median values for the total population were as follows: age 46 [interquartile range (IQR) 37.7–52.2], BMI 26.2 [IQR 23.3–29.7], CD4 cell count 388 [IQR 217–610] cells/mm3, and CD 4% 22.2 [IQR 14.7–30.4]. For those on antiretrovirals (ARVs) [n=174], 68% were using PIs and 20% NNRTIs. Among those on ARVs, 82% had a viral load of less than 400 copies/ml. In the overall population, 36% had current tobacco use (n=72) and 23% (n=46) had CD4 cell counts of less than 200 cells/mm3.
Vitamin D status and risk factors for vitamin D deficiency
In our total population, 64% (n=128) had vitamin D deficiency, 20.5% (n=41) had severe vitamin D deficiency, and 14% (n=28) had optimal vitamin D levels. Median serum 25(OH)D was 15.5 ng/ml [IQR 10.9–24.6] for the total population. Univariate analysis showed that African-American race, current tobacco use, increased BMI, lower serum calcium level, no supplemental vitamin D use, and low daily supplemental and total daily vitamin D intake were significantly associated with vitamin D deficiency (Table 1). In multivariate analysis, African-American race, increased BMI, and low daily vitamin D supplemental intake were significant independent predictors of vitamin D deficiency (Table 2). Factors such as season, previous diagnosis of AIDS, CD4 cell count, CD8 cell count, HIV viral load, duration of current antiretroviral medication use, class of antiretroviral use (NNRTI or PI), albumin, daily dietary vitamin D intake, and sunlight exposure were also assessed in the univariate analysis, but were not significantly associated with vitamin D deficiency (data not shown). Furthermore, the multivariate analysis model was also performed with season as an additional variable and it was not significant.
OR, odds ratio; 95% CI, 95% confidence interval; BMI, body mass index (kg/m2).
Variables included in multivariate analysis were age, African-American, female, BMI, current tobacco use, CD4%, corrected calcium, phosphorus, supplement vitamin D use, daily supplemental vitamin D intake, dietary vitamin D intake, and total vitamin D intake (defined as both dietary and supplement intake). The model was also performed with season as an additional variable and it was not significant.
OR, odds ratio; 95% CI, 95% confidence interval; AOR, adjusted odds ratio; BMI, body mass index (kg/m2).
When restricting univariate analysis to those only on antiretroviral therapy (n=156) with at least 75% adherence to ARVs within the past month or an undetectable viral load (viral load <48 copies/ml) in those patients whose adherence to ARVs was unknown, NNRTI or PI use was not significantly associated with vitamin D deficiency. However, NNRTI use trended slightly toward significance in patients with severe vitamin D deficiency (OR 1.996, 95% CI 0.833–4.783, p=0.1211).
Relationship between antiretroviral (ARV) use, race, and vitamin D levels
African-Americans had considerably lower median vitamin D levels than whites for those on ARV therapy (Fig. 1). For those not on ARVs, however, African-Americans had slightly higher median vitamin D levels than whites. This latter trend may be explained by the higher total daily vitamin D intake among the African-American group versus the white group. With regards to ARV use, those patients on NNRTIs had slightly lower median vitamin D levels than those on PIs regardless of race. The proportion of those using either NNRTIs or PIs was similar among African-Americans and whites. The Hispanic population could not be evaluated within this study with regards to the relationship between ARV use, race, and vitamin D levels due to limited numbers.
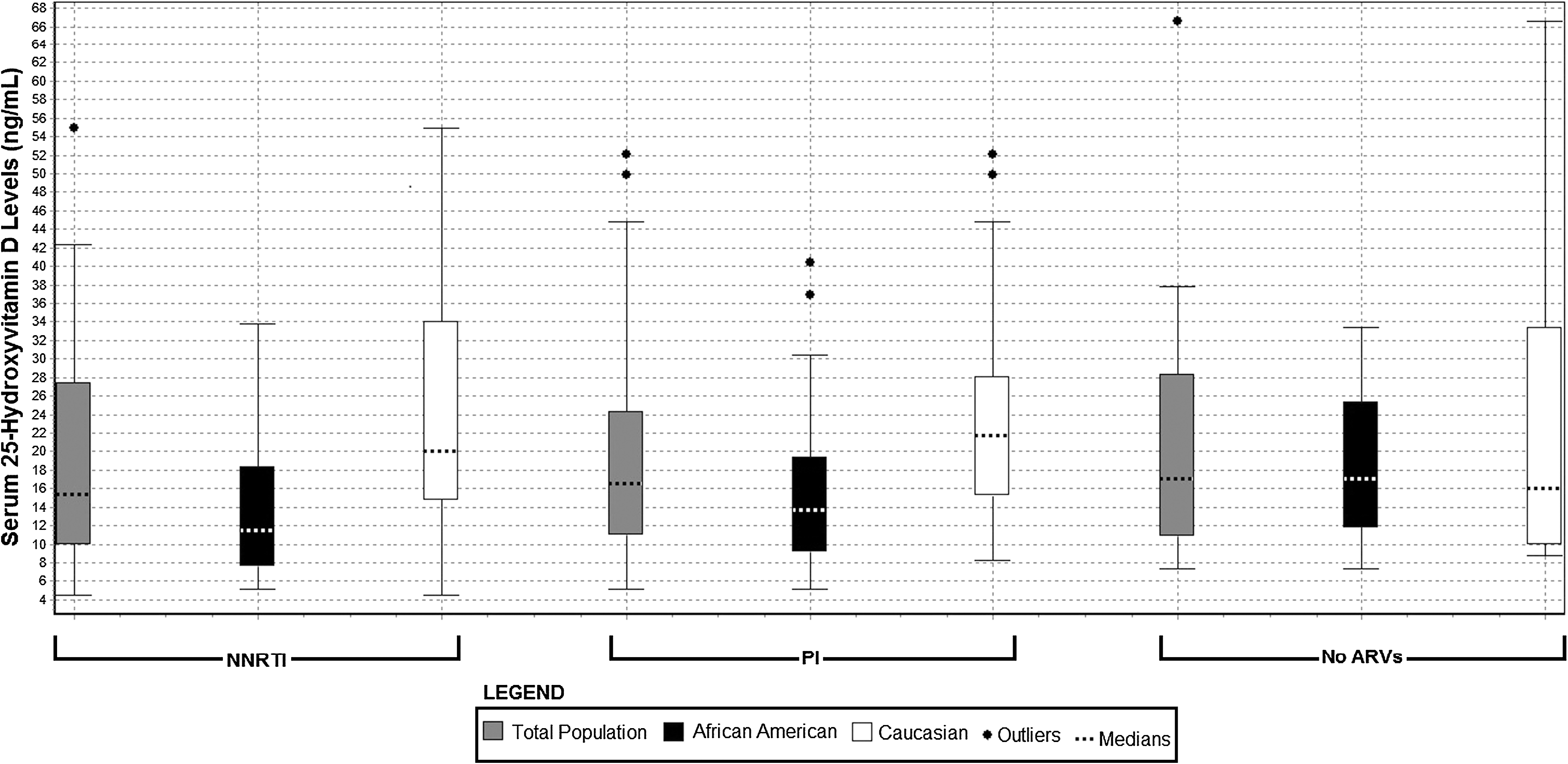
Relationship between antiretroviral use, race, and serum 25-hydroxyvitamin D levels.
Vitamin D questionnaire
All patients in the study were surveyed with a vitamin D questionnaire. Those who were vitamin D deficient had a significantly lower mean daily vitamin D supplemental intake than those who had vitamin D levels >20 ng/ml (115 vs. 342 IU, p<0.0001). Among those who had vitamin D deficiency 30% were using daily vitamin D supplementation compared to 54% in those who had vitamin D levels >20 ng/ml (p=0.0006). For those who used vitamin D supplementation within both groups, this was comprised mostly of nonprescribed vitamin D supplements such as multivitamins. Among the total population, 3% (n=6) used a daily supplemental vitamin D intake of less than 400 IU/day, 32% (n=64) used between 400 and 800 IU/day, and 3.5% (n=7) used more than 800 IU/day. Mean daily dietary vitamin D intake did not differ significantly between those who were vitamin D deficient and those who had vitamin D levels >20 ng/ml (273 vs. 344 IU, p=0.3873). However, mean total daily vitamin D intake was significantly lower in those in the vitamin D-deficient group compared to those who had vitamin D levels>20 ng/ml (388 vs. 686IU, p<0.0001). For mean daily sunlight exposure there was a trend toward significance between both groups with the vitamin D-deficient group having less exposure compared to those who had vitamin D levels >20 ng/ml (70 vs. 87 min, p=0.0659).
Discussion
Almost two-thirds of our HIV-infected population had vitamin D deficiency and at least 20% had severe vitamin D deficiency. These findings were surprising given that our clinic is located at latitude 29 degrees North and skin synthesis of vitamin D is possible annually at the latitude of 32 degree North or closer to the equator. 28 Furthermore, seasonality (Fall/Winter months) did not have an effect on those who had vitamin D deficiency. Understandably, other studies have found a significant association between seasonality (Winter/Spring months) and vitamin D deficiency, 17,18 since these were conducted at considerably more northerly latitudes than our study. One major explanation for the high prevalence of vitamin deficiency in our population could be the greater proportion of those who were African-American (49%). The significant association between African-American race and vitamin D deficiency has been well established in several studies. 15,17,19,21,22,26 Those who have darker skin pigmentation are less likely to adequately synthesize vitamin D from sunlight exposure than those who have lighter skin pigmentation such as whites. Darker skin pigmentation reduces cutaneous vitamin D absorption by as much as 99%, 29 and much greater exposure to UVB is needed to generate the same amount of serum 25(OH)D as fair-skinned individuals. 30 In our study, those who had vitamin D deficiency also tended to have shorter periods of daily sunlight exposure.
Risk factors for vitamin D deficiency in our population also included increased BMI and low daily supplemental vitamin D intake. In our study, for each one-point increase in BMI, there was a 6.9% increased risk of vitamin D deficiency. Other studies have also found a significant association between high BMI and vitamin D deficiency in both the general and HIV-infected populations. 2,19,21,31 –33 Wortsman et al. found that obese patients had lower basal serum 25(OH)D levels than nonobese patients, with BMI inversely associated with peak blood concentrations of vitamin D. 31 They proposed that differences in vitamin D levels were not attributed to the capacity of the skin to produce vitamin D after UVB exposure, but to a slower release of vitamin D from the skin into the circulation due to sequestration of vitamin D in adipose tissue in obese patients. Obesity defined as BMI >30 kg/m2 is a prevalent problem worldwide and is increasingly observed in African-Americans in the United States. 32 Those with low vitamin D levels may also be at an increased risk for insulin resistance and metabolic syndrome. 33 –36 Yanoff et al. found that the relative risk of hypovitaminosis D (defined as <15 ng/ml) continued to increase with greater BMI. 32 Authors of this study suggested that obese African-American adults, especially, those with a BMI >35, should be either routinely supplemented with vitamin D or routinely screened for vitamin D deficiency. The clinical relevance of vitamin D supplementation remains to be tested in HIV-infected patients, especially in obese African-Americans.
In our study, the significant association between low daily supplemental vitamin D intake and vitamin D deficiency is consistent with other studies. 16,37 Our study showed that patients who had a mean total daily vitamin D intake of at least ∼700 IU were less likely to have vitamin D deficiency. In the United States, current total vitamin D recommended daily intake varies between 400 and 800 IU per day (depending on age), 38 which is somewhat more than the mean total daily vitamin D intake observed in our overall population. One study found that vitamin D supplementation of 600-800 IU/day in HIV-infected postmenopausal African-American and Hispanic women was not sufficient enough to produce optimal vitamin D levels (>30 ng/ml) for a majority of the study population. 37 Taken together, a much higher total recommended daily vitamin D intake of at least 1000–2000 IU/day may be necessary to overcome vitamin D deficiency, especially, for African-American and Hispanic populations.
It is postulated that NNRTIs such as efavirenz may affect vitamin D metabolism through CYP3A4 and CYP24 induction. 17 CYP3A4 is responsible for conversion of vitamin D substrate to 25(OH)D and CYP24 for conversion of serum 25(OH)D and 1,25(OH)2D to inactive metabolites. Induction of these two enzymes may reduce both the amount of vitamin D substrate available and serum 25(OH)D. Efavirenz may also decrease 25(OH)D production by reducing transcription of CYP2R1 [another 25(OH)D hydroxylase]. 17 Other medications such as phenobarbital and rifabutin have been shown to cause osteomalacia through CYP3A4 induction leading to low vitamin D levels. 39 –42 In our study, patients who used NNRTIs had slightly lower median vitamin D levels than those on PIs regardless of race. However, we did not find a significant association between NNRTI use and vitamin D deficiency or severe vitamin D deficiency as in other studies. 17 –19,26 Three of these latter studies involved a greater number of patients (N>200) in addition to a higher proportion of patients who used NNRTIs such as efavirenz compared to our study.17-19 It is not known, however, if NNRTIs are the cause of vitamin D deficiency, since the collection of baseline vitamin D levels is uncertain in some studies. 17,19 The Swiss Cohort Study retrospectively analyzed changes in vitamin D levels in treatment-naive HIV-infected patients at baseline and at 12 and 18 months and found that those who were treated with NNRTIs had significantly lower median vitamin D levels after 18 months [46–39 nmol/liter (18.4–15.6 ng/ml)], but no significant changes with PIs [42–43 nmol/liter (16.8–17.2 ng/ml)]. 18
These findings are also consistent with a very recent study that showed that patients on an NNRTI-based regimen had significantly lower vitamin D levels after 12 months, but no changes for those on PIs. 26 Another study showed that patients who had efavirenz exposure for 30–90 days had significantly lower median vitamin D levels (8.6 IQR 5.3–9.6 ng/ml) versus those exposed for less than 30 days (13.9 IQR 9–21.1 ng/ml). 17 Some of these studies, however, were retrospective in nature and did not account for major confounding factors such as daily supplemental vitamin D intake, dietary vitamin D intake, or sunlight exposure. 18,26 To our knowledge, previous studies have not prospectively obtained repeated measures of vitamin D levels, especially baseline levels, prior to and after initiation of antiretroviral therapy to determine whether antiretroviral classes such as NNRTIs and PIs cause changes in vitamin D levels over time. Prospective studies are needed to determine the clinical significance of the effects of NNRTIs and PIs on vitamin D metabolism.
Our study had some limitations. First, we had a relatively small sample size that used NNRTIs (20%); this may have caused our study to have an inadequate power to determine a relationship between NNRTI use and vitamin D deficiency or severe vitamin D deficiency. This was a cross-sectional survey study design that does not allow for establishing causality between specific risk factors and vitamin D deficiency. We used an unvalidated questionnaire to assess total daily vitamin D intake; subjective recall of use of vitamin D supplementation may not be accurate. However, measures of daily dietary vitamin D intake of the most common foods with a high vitamin D content were evaluated for each subject utilizing the criteria defined by the office of dietary supplements. 27 Collected data on daily sunlight exposure from patients were subjective and may not be sufficient, since other variables such as sunscreen use, time of day, and hats/clothing could affect daily sunlight exposure. Furthermore, correlations between sunlight exposure and vitamin D levels have not been particularly high when using questionnaires, since there are so many other factors that can affect cutaneous synthesis of vitamin D. 43 Our study did have a major strength in that it recorded both daily dietary and supplemental vitamin D intake for each patient.
In conclusion, we observed a high prevalence of vitamin D deficiency in our diverse HIV-infected population in the South-Central United States. In the HIV population, African-Americans or patients with high BMI may benefit from vitamin D supplementation. Furthermore, larger, prospective, randomized controlled clinical trials are needed to test the clinical relevance of vitamin D supplementation for treatment of poor health outcomes such as metabolic syndrome. Finally, prospective studies are also needed to determine the effects of NNRTIs and PIs on vitamin D metabolism.
Footnotes
Acknowledgments
The contribution of the Therapeutic Concepts clinic staff is greatly appreciated. J.G. and C.M. contributed to the study design, ordering of laboratory markers, and manuscript review. A.T. contributed to data collection and analysis. S.A. contributed to the statistical analysis of the study. K.W.G. contributed to the statistical analysis and manuscript review. Data were presented previously at the 18th International AIDS Conference as an oral poster presentation.
Author Disclosure Statement
No competing financial interests exist.