
Abstract
A total of 242 HIV-1-infected children were followed up at the Complexe Pédiatrique of Bangui, Central African Republic, including 165 receiving antiretroviral treatment in first- (n=150) or second-/third-line (n=15) regimens. They were prospectively included in a study, in 2009, to assess their virological status and prevalence of antiretroviral drug-resistance mutations in cases of virological failure, according to revised 2010 WHO criteria (e.g., HIV-1 RNA >3.7 log10 copies/ml). Detectable plasma HIV-1 RNA was observed in 53% of children under first-line treatment, and virological failure was diagnosed in 40%, which was associated in 85% of cases with viruses harboring at least one drug-resistance mutation to nucleoside reverse transcriptase inhibitors (NRTI) or nonnucleoside reverse transcriptase inhibitors (NNRTI), and in 36% of cases with at least one major drug-resistance mutation to NRTI or NNRTI when excluding the M184V mutation. Overall, the proportion of children receiving a first-line regimen for a median of 18 months with virological failure associated with drug-resistance mutations, and thus eligible for a second-line treatment, was estimated at 34% of the whole cohort. In children under second-/third-line therapy, virological failure occurred in 47%, plus at least one major drug-resistance mutation to NRTI or NNRTI, though less commonly to protease inhibitors. Taken together, these findings argue in favor of the urgent need to improve distribution of pediatric antiretroviral drugs in the Central African Republic, to increase adherence by treated children, and to offer adequate HIV biological monitoring.
Introduction
T
However, previous studies in ARV-treated African children have reported a high prevalence of virological failure, variable according to the series, ranging from 13%, 8 44%, 7 to 75% 11 after 6 months of treatment, from 34% 12 to 46% 13 after 12 months, and 31% 14 after 24 months, and generally associated with the selection of ARV-resistance mutations. 7,11,12,15 –17 In that context, the interest of laboratory monitoring, using immunological as well as virological markers, to prevent therapeutic failure in ARV-treated children, especially children less than 2 years old, 18 has still not been demonstrated by randomized clinical trial. In ARV-treated adults living in resource-limited settings, it is, however, currently well demonstrated that the lack of virological monitoring increases the risk of virological failure and the selection of ARV-resistant viruses. 19 –21
In a previous report on 52 HIV-infected children followed up in the Complexe Pédiatrique of Bangui, the capital city of the Central African Republic, plasma HIV-1 RNA levels remained detectable in 75% of children after 6 months of ARV treatment, and 77% of children showed virological failure and resistant viruses. 11 These findings prompted us to assess the effectiveness of first- and second-/third-line ARV treatments in a larger series of HIV-infected children attending the Complexe Pédiatrique of Bangui, who were treated for a median of 18 months. In addition to assessing CD4 T cell counts, plasma HIV-1 RNA load was also used as a virological marker for treatment failure, as proposed by the World Health Organization (WHO) recommendations for HIV monitoring in resource-limited settings. 2,22
Materials and Methods
Children studied
All HIV-1-infected children attending the Complexe Pédiatrique of Bangui were prospectively included from April to June 2009.
The Complexe Pédiatrique of Bangui is the main healthcare clinic for HIV-infected children in the Central African Republic. The Complexe Pédiatrique belongs to the North–South so-called “ESTHER” (for “Ensemble pour une Solidarité Thérapeutique en Réseau”) network of partnerships between healthcare structures from France and the Central African Republic. Its operational research purpose is to promote the use of biological markers to monitor HIV-infected children treated by ARV drugs. “ESTHER” provides laboratory facilities for the Complexe Pédiatrique, including implementation of a class II laboratory equipped with a CD4 T cell analyzer, a hematology counter, and a spectrophotometer, and measurement of HIV-1 RNA load to the Pasteur Institute, Bangui. In addition, genotypic resistance tests can be carried out at the virology unit of the Européen Georges Pompidou Hospital, Paris.
Feedback is given to the children's parents and their pediatricians on all tested parameters carried out during the study period, plus information on any changes made to ARV treatment, if needed, and improvements in medical care. In particular, adherence to treatment is assessed at each visit by an empirical questionnaire addressed to the parent or the child, as previously described. 11 A switch of drug therapy remains challenging because there is a lack of second-line ARV drugs in the Central African Republic.
Children attending the Complexe Pédiatrique were principally born from HIV-infected mothers and have, in principle, received HIV preventive therapy from mother to child following national guidelines. Newborn children infected with HIV, despite prevention therapies, are followed up according to WHO recommendations for developing countries. 2,22 In addition, a minority of HIV-infected children also suffers from sickle-cell disease. In 2009, 1800 HIV-infected children were recorded, among which 450 were receiving ARV treatment.
HIV-1 viral load and CD4 cell count measurements
HIV-1 RNA viral load was performed using a generic HIV-1 RNA quantification assay (Biocentic, Bandol, France) on an Applied Biosystems 7500 real-time PCR system, as previously described. 23 The threshold of detection for this assay was 300 copies/ml. 23 The CD4 T cell count was measured by flow cytometry using FACSCalibur (Becton Dickinson, San Jose, CA), and expressed as an absolute count and percentage.
Genotypic resistance testing
HIV-1 protease and reverse transcriptase (RT) genes were sequenced by a ViroSeq HIV-1 genotyping system (Celera Diagnostics, Alameda, CA) using 1 ml of plasma sample. Resistance mutations were reported and interpreted as listed by the Agence Nationale de Recherches sur le SIDA et les hépatites virales (ANRS) algorithm (updated in July 2010;
The HIV-1 subtype was obtained by phylogenic analyses of RT gene sequences using reference sequences for the HIV-1 genetic subtypes and circulating recombinant forms obtained from the Los Alamos Database (available at
Results
Virological and immunological characteristics of the studied children
A total of 242 HIV-infected children were included over a period of 3 months; among these 127 (53%) were girls. Their median age was 8 years [range: 4 months–18 years; 77 children (32%) were aged 4 months–5 years]. Note that children in the present series were different from those included in the previous study conducted in the Central African Republic in 2006. 11
Most children were infected with HIV-1 recombinant CRF11_cpx (37%) or subtype A (36%). In addition, a large variety of HIV-1 subtypes was found: CRF02_AG (4%), H (2%), D (2%), F (2%), C (2%), CRF13_cpx (2%), and CRF21_A2D (1%). HIV-1 subtype was undetermined in 10% of cases due to numerous recombination events.
Among the 242 HIV-1-infected children, 165 (68%) were receiving an ARV-based therapy (Table 1). Most children (150/165, 91%) were receiving a first-line regimen, 13 (8%) a second-line regimen, and 2 (1%) a third-line regimen. All children were ARV-naive when they began their first-line ARV regimen and all children received a second-line treatment after a first-line regimen. In further analyses, children receiving a second- or third-line regimen were pooled into a group of 15 children. Among ARV-treated children, the adherence was estimated as very good in 24%, good in 5%, middle in 9%, and bad in 62%.
Median; interquartile range in parentheses.
NA, not applicable.
The threshold of virological failure according to the revised 2010 WHO recommendations was plasma HIV-1 viral load >3.7 log10 copies/ml.
The rate of resistant viruses is calculated among successful results for genotypic resistance tests carried out in plasma samples with detectable HIV-1 viral load (e.g., >300 copies/ml).
The rates of virological failure and of resistant viruses between children receiving first-line regimen and children receiving second-/third-line regimen were not statistically different (Mann–Whitney U test).
Median HIV-1 RNA viral load and absolute CD4 T cell counts in the 77 untreated children were 4.9 log10 copies/ml [interquartile range (IQR): 1.69–6.45] and 652 cells/mm3 (IQR: 378–1091), respectively (Fig. 1). Most ARV drugs in the first-line regimen were prescribed as a generic tablet containing a combined formulation of d4T/3TC/NVP, received by 76% of children. Nine children (5%) were prescribed a regimen containing lopinavir (LPV) as a first-line treatment. All children treated by LPV had undergone a 6-week adaptation period to assess drug tolerance. Median HIV-1 viral loads and CD4 T cell counts were assessed 18 months after initiation of the first-line regimen.
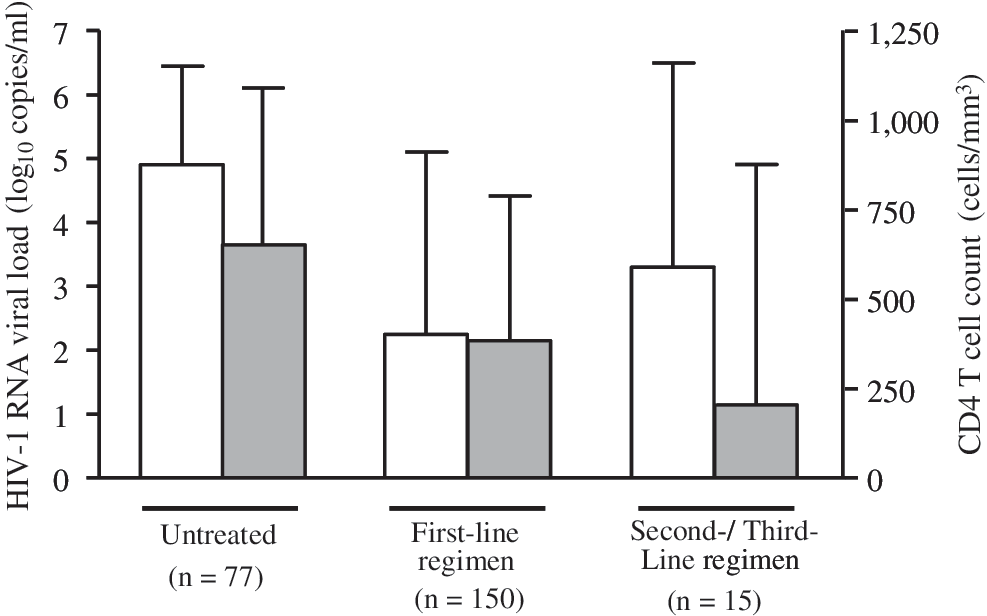
Median HIV-1 RNA plasma loads (white box) and absolute CD4 T cell counts (gray box) in 242 HIV-1-infected children followed-up in the Complexe Pédiatrique of Bangui, including 77 untreated children, 150 children who were receiving a first-line antiretroviral-based treatment, and 15 children receiving a second- or third-line antiretroviral-based treatment. Median HIV-1 RNA load and CD4 T cell counts were assessed at 18 months after initiation of the first-line regimen and 30 months after the initiation of a second- or third-line regimen. The error bars represent the interquartile ranges of the distribution.
Among the 150 children receiving a first-line regimen, 71 (47%) displayed an HIV-1 viral load of <400 copies/ml with a median CD4 T cell count of 702 cells/mm3 (IQR: 168–1139). Thus, 53% of HIV-infected children displayed detectable HIV-1 viremia under a first-line ARV-based treatment, with a median viral load of 5.0 log10 copies/ml (IQR: 3.7–5.6) and a median CD4 T cell count of 258 cells/mm3 (IQR: 85–525) (Fig. 1). In addition, 60 (40%) children under a first-line ARV-based treatment had an HIV-1 viral load >3.7 log10 copies/ml, e.g., the threshold of virological failure according to the revised 2010 WHO recommendations. 2
In the 15 children receiving a second-/third-line regimen, an LPV-containing regimen was prescribed for seven (47%) and an indinavir-containing regimen for three children (20%). The five remaining children received a nonnucleoside reverse transcriptase inhibitor (NNRTI)-based regimen. The median HIV-1 viral loads and absolute CD4 T cell counts were assessed 30 months following initiation of a second- or third-line regimen (IQR: 8–60 months). Among the 15 children, only four (27%) had an HIV-1 viral load <400 copies/ml, with a median absolute CD4 T cell count of 415 cells/mm3. Thus, a high proportion (73%) of HIV-infected children displayed detectable HIV-1 RNA plasma viremia under second- and third-line ARV-based treatments, with a median viral load of 5.4 log10 copies/ml (IQR: 3.0–6.6) and a median CD4 T cell count of 130 cells/mm3 (IQR: 56–1264) (Fig. 1). Seven (47%) children under a second-/third-line ARV-based treatment had an HIV-1 viral load of >3.7 log10 copies/ml.
In the present series of HIV-1-infected children, whose ages were mostly >5 years (68%), the distribution of CD4 T cell counts, expressed as a percentage, was similar to CD4 T cell counts in untreated and treated children (data not shown).
Test results for genotypic resistance
Successful results for genotypic resistance tests were obtained in 59 samples taken from children receiving a first-line regimen and in 10 samples taken from children receiving a second-/third-line regimen. Overall, 86% (59/69) of children harbored a virus and had at least one drug-resistance mutation. There was no relationship between resistance mutations patterns and HIV-1 subtypes.
Children receiving a first-line regimen
Regarding nucleoside reverse transcriptase inhibitors (NRTI), 49 of 59 children (83%) displayed viruses that harbored at least one mutation associated with NRTI resistance. On average, the virus exhibited one mutation associated with resistance to NRTI (range: 0–6). The most prevalent resistance mutations included M184V (n=43, 73%), followed by T69D/N/S (n=10; 17%), L74I/V (n=5; 8%), K65R (n=5; 8%), and Q151M (n=1; 2%) (Fig. 2A). Thymidine-associated mutations (TAMs) were present in seven (12%) viruses, and one virus (2%) showed an extensive resistance profile (e.g., at least three TAMs).
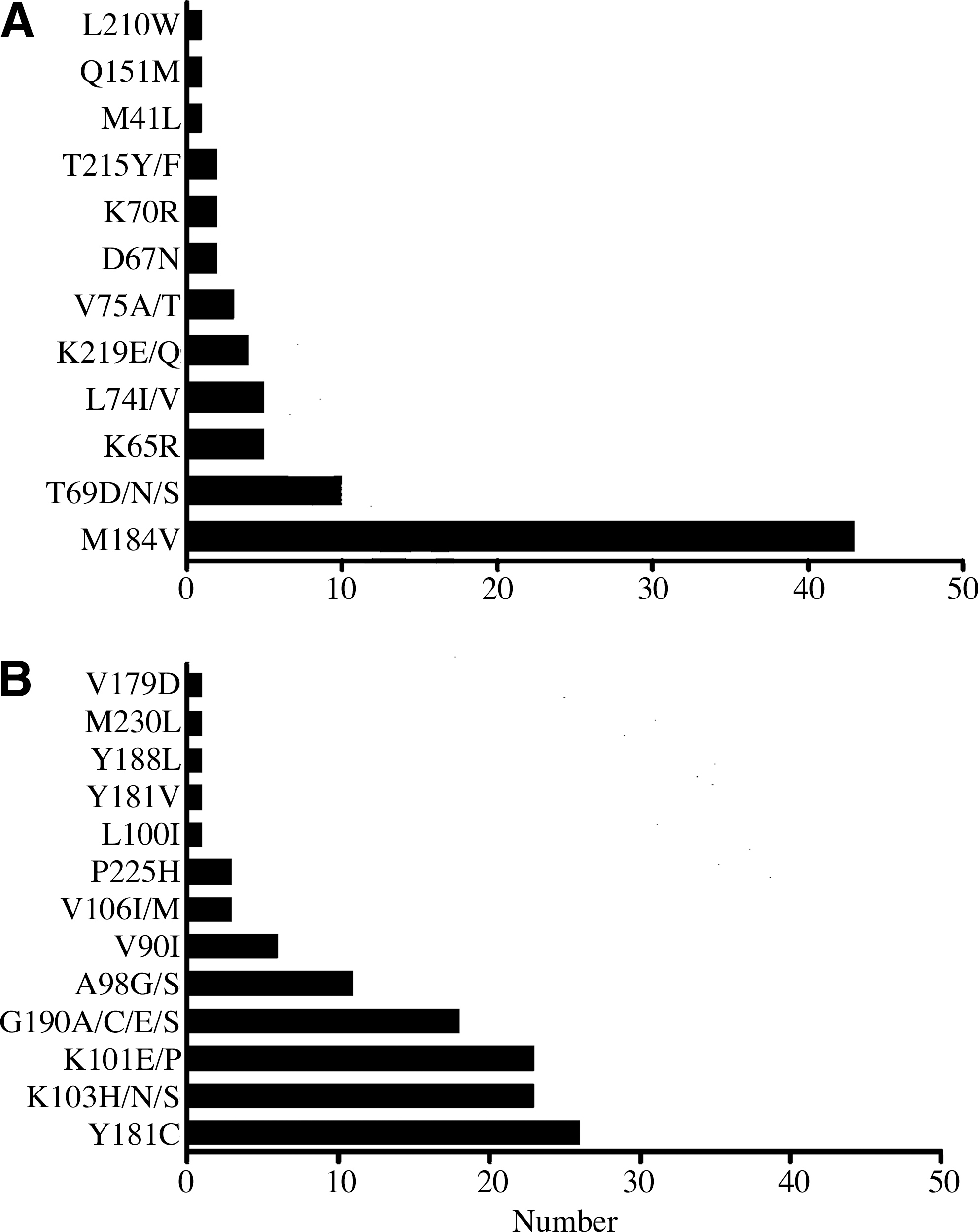
Number of resistance-associated mutations to nucleoside reverse transcriptase inhibitors
Assessing the prevalence of resistance to NNRTIs, 50 of 59 children (85%) displayed viruses that harbored at least one NNRTI-resistance mutation. On average, the viruses exhibited two mutations associated with resistance to NNRTI (range: 0–3). The most prevalent resistance mutations included Y181C (n=26; 44%), followed by K103H/N/S (n=23; 39%), K101E/P (n=23; 39%), G190A (n=18; 30%), and A98G/S (n=11; 19%) (Fig. 2B).
Fifty children (85%) who received a first-line regimen displayed viruses that harbored at least one drug-resistance mutation to NRTI or to NNRTI. If the M184V mutation was excluded, 21 children (36%) who received a first-line regimen had viruses that harbored at least one drug-resistance mutation to NRTI or NNRTI.
Among the 59 genotypic resistance tests performed in plasma samples from children receiving a first-line regimen, no major resistance mutations to PI drugs were detected.
Children receiving second-/third-line regimens
Among the 10 children receiving a second-/third-line regimen and who had a genotypic resistance test, nine (90%) displayed viruses that harbored at least one drug-resistance mutation to NRTI or NNRTI, and five (50%) had mutations after excluding the M184V mutation.
Regarding the NRTI drug class, 80% (8/10) of children displayed viruses with at least one NRTI-resistance mutation. On average, the viruses exhibited two mutations associated with resistance to NRTI (range: 0–5). The most prevalent resistance mutations included M184V (n=6; 60%), followed by 215Y/F (n=4; 40%), L210W (n=2; 20%), and K70R (n=2; 20%) (Fig. 3A). TAMs were present in five (50%) viruses, among which four (40%) showed extensive resistance profiles.
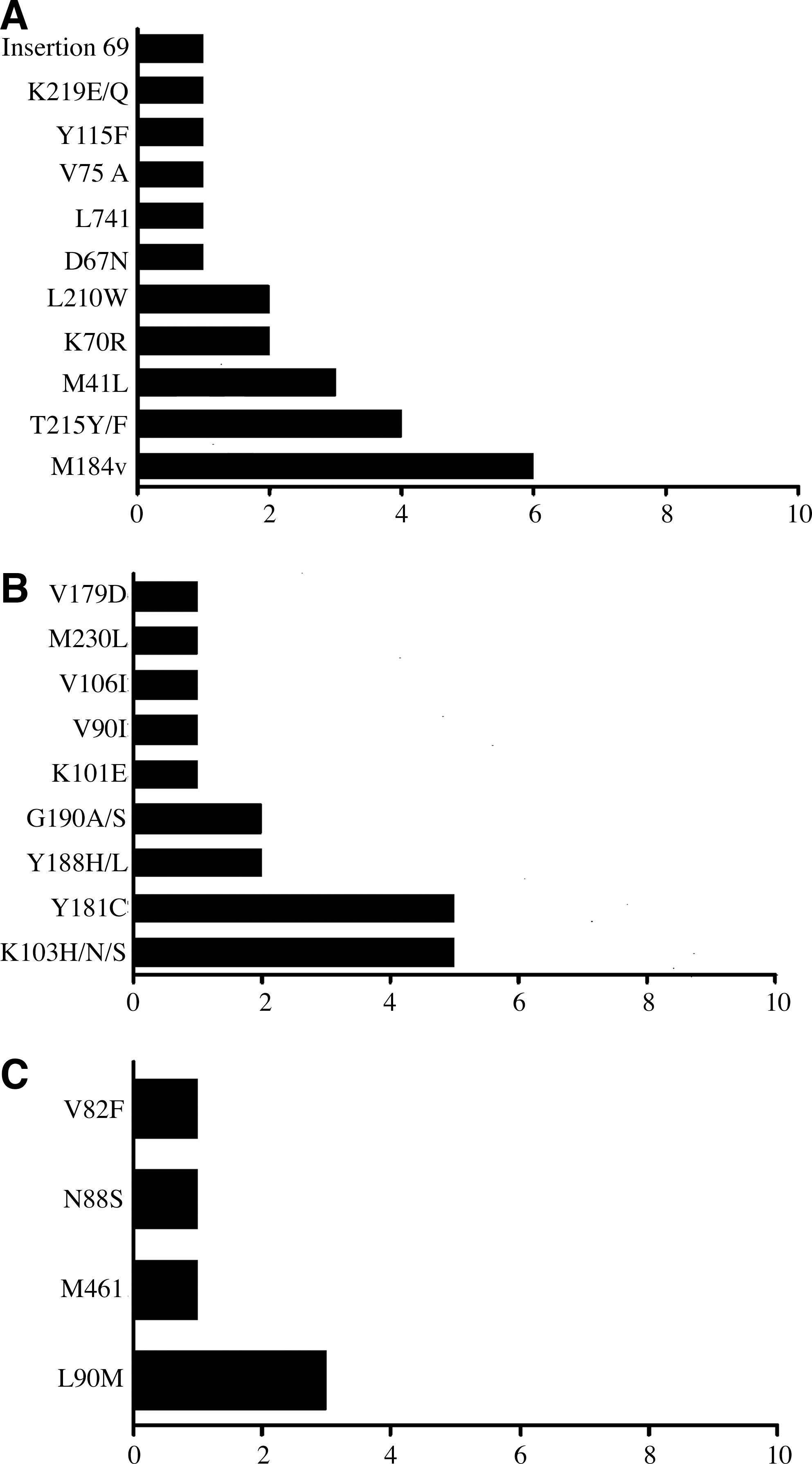
Number of resistance-associated mutations to nucleoside reverse transcriptase inhibitors
Assessing the prevalence of resistance to NNRTI, 80% of children displayed viruses that harbored at least one NNRTI-resistance mutation. On average, the virus exhibited two mutations associated with resistance to NNRTI (range: 0–3). The most prevalent resistance mutations included Y181C (n=5; 50%) and K103N (n=5; 50%), followed by Y188L (n=2; 20%) and G190A/S (n=2; 20%) (Fig. 3B).
Only four children displayed viruses exhibiting major PI-resistance mutations. The resistance mutation L90M was detected in three viruses, and was associated with the V82F mutation in one virus; the remaining virus harbored the resistance mutations M46I and N88S (Fig. 3C).
Interpretation of genotypic resistance tests and possible future therapeutic options
Genotypic resistance profiles were interpreted according to the ANRS algorithm for all drugs proposed for second-line regimens, according to the revised 2010 WHO recommendations. 2
Among the 59 sequenced viruses found in children receiving a first-line regimen, 49 (83%), 50 (85%), and 52 (88%) remained susceptible to abacavir, didanosine, and tenofovir, respectively. These data show that the NRTI drugs recommended for second-line regimens in Africa are expected to be active in more than 80% of cases. Conversely, the use of first-generation NNRTI appeared largely compromised, as 83% of children with virological failure, in a first-line regimen, were resistant to efavirenz and NVP. Moreover, resistance to etravirine was observed in nine viruses (15%), including an intermediate level of resistance in seven and a high level of resistance in two viruses. The PI drug class remained fully active in all children after first-line therapeutic failure.
Viruses taken from the 10 children displaying virological failure after a second- or third-line regimen showed 70%, 70%, and 80% remained susceptible to abacavir, didanosine, and tenofovir, respectively. Regarding the NNRTI drug class, 80% of viruses were resistant to efavirenz and NVP, and an intermediate level of resistance to etravirine was observed in two viruses (20%). Interestingly, all 10 viruses remained susceptible to LPV, but only six to atazanavir. Finally, the four viruses with PI-resistance mutations remained sensitive to only three molecules within the PI drug class: darunavir, fosamprenavir, and LPV. None of the PI-resistant viruses was susceptible to atazanavir.
Discussion
This study has reported on a large series of 242 HIV-1-infected children followed up at the Complexe Pédiatrique of Bangui, including 165 who received ARV-containing regimens in first- (n=150) or second-/third-line (n=15) treatments. Detectable plasma HIV-1 RNA was observed in 53% of children under a first-line ARV-based treatment, and virological failure was diagnosed in 40% according to the revised 2010 WHO criteria. 2 In children receiving a first-line regimen and who had virological failure, 85% displayed viruses harboring at least one drug-resistance mutation to NRTI or NNRTI, and 36% showed at least one major drug-resistance mutation to NRTI or NNRTI after excluding the M184V mutation. These observations demonstrate the high rate of virological failure after 18 months of first-line treatment, which is generally associated with drug-resistance mutations, but, in a minority of cases (15%), with viruses that are still susceptible to ARV drugs. Overall, 34% of the whole cohort of children receiving first-line ARV treatment for a median of 18 months had virological failure and displayed ARV-resistant viruses, and thus a second-line treatment was needed. In children under a second-/third-line therapy, virological failure appeared to be slightly more prevalent; in addition, there was at least one major drug-resistance mutation to NRTI or NNRTI, though less commonly to PI. Taken together, these findings show the necessity for systematic monitoring of plasma HIV-1 RNA load in ARV-treated children to diagnose, as early as possible, any therapeutic failure and to then switch to a new therapeutic line.
In a previous series of 52 children receiving first-line ARV-based treatment for 6 months, conducted at the Complexe Pédiatrique in 2007, 11 detectable plasma HIV-1 RNA (e.g., >400 copies/ml) was observed in 27 (52%) children, and virological failure was diagnosed in 12 (23%) (unpublished personal data), according to the revised 2010 WHO criteria. 2 In children under a first-line ARV-based treatment for 18 months, the proportion of therapeutic failures, in 2009, was twice as high (40%), whereas treatment duration had increased 3-fold. In addition, the median HIV-1 RNA load in children who still had replicating HIV, despite ARV treatment, was higher after 18 months of treatment (5.0 log10 copies/ml) than after 6 months (3.6 log10 copies/ml, unpublished personal results).
The use of the threshold proposed by the 2010 revised WHO recommendations to diagnose virological failure (e.g., 3.7 log10 copies/ml) was more robust than the use of the threshold for HIV-1 viral load detection (e.g., >400 copies/ml) based on comparisons between the 2007 series of children treated for 6 months and the current 2009 series of children treated for 18 months. Whether persistent low levels of viral replication are associated with therapeutic failure in ARV-treated children warrants further investigation. These findings demonstrate that maintaining first-line ARV treatment, despite a detectable viral load, is associated over time with an increased rate of virological failure as well as an increased plasma viral load.
In sub-Saharan Africa, the rate of virological failure is widespread (quantitative threshold of plasma viral load defined as virological failure), and ranges from 17% to 75%. 7,11 –14,20,25 –30 Furthermore, the rate of therapeutic failure appears greater when NNRTI-based regimens are used as a first-line treatment, and then ranges from 20% to 75%, 7,11 –14,20,25,28,29 compared to when a PI-based regimen is used (range: 26–36%). 26,27 In the series of children reported here, who were prescribed mostly with a first-line ARV treatment, including NNRTI, virological failure was frequently associated with major NNRTI-resistance mutations, whereas no major PI-resistance mutations were observed in children treated by first-line PI therapy. These observations emphasize the possibility of using PI more frequently as a pediatric first-line regimen in Africa. 20,30 In particular, the use of an LPV-based treatment could be of interest because of the frequent transmitted drug resistance to NNRTI caused by the common use of single-dose NVP to prevent HIV mother-to-child transmission in sub-Saharan Africa. In addition, there is a higher rate of virological success in PI-treated children versus NNRTI-treated children. However, problems associated with LPV treatment include its high cost and possible side-effects (diarrhea).
To our knowledge, only a few studies have reported on the virological response of HIV-infected children after receiving a second- or third- line regimen in resource-limited settings. 31,32 Although there was a limited number of inclusions in the present series of children receiving a second- or third-line regimen, the rate of virological success was very low, with only 27% of children exhibiting an undetectable plasma viral load. In contrast, virological failure and NRTI- or NNRTI-resistance mutations (even after excluding the M184V mutation) were much greater in children under a second-/third-line treatment than in those under a first-line regimen. These observations indicate that switching from a first- to a second-line ARV treatment is not sufficient by itself to avoid further therapeutic failure. The lack of a genotypic resistance test at the initiation of a second-line regimen prevents assessment of the antiviral activity of ARV drugs used in the new regimen, and may likely increase the risk of virological failure of second-line regimen, especially in a minority of children who harbor viruses resistant to NRTI, recommended as a second-line regimen in Africa. Since the presence of the M184V resistance mutation to 3TC/emtricitabine (FTC) does not further exclude the systematic use of these drugs in a second-line regimen, we can hypothesize that a significant proportion of children taking second-line ARV treatment, as recommended by the WHO, will in fact received two fully active ARV drugs in the context of viruses harboring the M184V mutation, which is thought to decrease viral fitness. 33,34 However, the in vivo impact of the M184V mutation in viruses of children under second-line treatment should be investigated in African cohorts.
Interestingly, wild-type viruses were detected in 15% of children receiving a first-line ARV treatment, resulting in virological failure (plasma viral load >3.7 log10 copies/ml). This finding is similar to the 20% rate found in adult patients displaying virological failure associated with wild-type viruses, as previously reported in Douala. 35 Virological failure associated with wild-type viruses is likely due to poor adherence, which needs urgent correction. Indeed, the level of adherence in ARV-treated children was found to be inversely associated with HIV-1 RNA plasma level after 6 months of ARV treatment. 11 Virological monitoring appears to be of particular concern in HIV-infected children who are known to have difficulty in maintaining good adherence. In addition to poor adherence, the toxicity of ARV drugs may also account for an alternative first-line regimen or second-line regimen, as previously reported in 2% of ARV-experienced children living in Malawi. 36
A high frequency (86%) of resistance mutations has been observed in HIV-infected African children displaying a detectable HIV-1 RNA load while receiving ARV drugs: 96% in Zambia, 14 71% in the Ivory Coast, 12 73% in Mali, 7 and 77% in the Central African Republic. 11 In the present series, the most common resistance profiles were associated with the wide use of 3TC and first-generation NNRTI, as recommended by the WHO as a first-line ARV treatment in sub-Saharan Africa. 2,22 Our findings highlight the need for virological monitoring when the first-generation NNRTIs are used, particularly in the population of children whose plasma viruses could have selected NNRTI resistance mutations due to perinatal prophylaxis drugs, which could further impact the virological outcome of ARV-based treatment. 37 –39 Indeed, the lack of monitoring for HIV-1 RNA load likely delays the diagnosis of virological failure, thus increasing the duration of persisting viral replication under ARV drugs, and, consequently, the risk of accumulating NNRTI mutations.
In the present series, the antiviral activity of ARV drugs in the second-line regimen proposed by the 2010 revised WHO recommendations in case of virological failure was not largely impacted, with a predictive activity of tenofovir, abacavir, and didanosine in more than 80% of cases, respectively. The K65R mutation, which confers high resistance to tenofovir, was observed in 8% of viruses from children receiving a first-line regimen. This resistance mutation was likely selected under the drug pressure of different NRTIs (such as stavudine) in the context of the HIV-1 non-B subtypes.
40,41
The accumulation of at least three TAMs, which confer resistance to tenofovir according to the ANRS algorithm (
Finally, the selection of PI-resistant viruses that occurs during a second-line regimen strongly compromises future therapeutic options as atazanavir is not active against any of the PI-resistant viruses. However, LPV remains active in all cases despite the selection of mutations associated with LPV resistance in some viruses.
Based on results from genotypic resistance tests, interpreted by the ANRS algorithm, the activity of etravirine, a new second-generation NNRTI, has been compromised in around 16% of circulating HIV-1 strains. Such a prevalence of predicted etravirine resistance appears much higher than rates (2.4–3.8%) previously reported in Western countries. 42,43 In the present series, primary resistance to etravirine may reflect possible genetic specificity of HIV-1 non-B subtypes, 44 in addition to the long duration of viral replication under first-generation NNRTI drugs in Africa.
In conclusion, virological failure of first-/second-/third-line ARV regimens, generally associated with major ARV drug-resistance mutations, is frequent in HIV-1-infected children from the Central African Republic, and is treated according to WHO recommendations. This has important public health implications. First, it emphasizes the need to improve the distribution of ARV drugs in order to prevent therapeutic interruption, to increase adherence by treated children, and to offer adequate HIV biological monitoring. Second, these factors should be considered in connection with all further programs for ARV drugs given to HIV-infected children living in the Central African Republic as about 50% of currently ARV-treated children have therapeutic failure: there is a need for new therapeutic options. However, these are likely to be more expensive and difficult to obtain in the context of resource-limited settings.
Footnotes
Acknowledgment
Supported by Grant GIP ESTHER (Ensemble pour une Solidarité Thérapeutique Hospitalière en Réseau), Paris, France.
Author Disclosure Statement
No competing financial interests exist.