
Abstract
The World Health Organizations HIV Drug Resistance (WHO HIVDR) Threshold survey method was used to assess transmitted HIVDR in newly diagnosed HIV-1-infected primigravida women attending the Prevention of Parent to Child Transmission (PPTCT) centers in Kakinada, in whom it is likely that the infection had recently occurred. Out of the 56 consecutively collected eligible specimens, 51 were tested using the ViroSeq RT-PCR method (Abbott Germany) to obtain 47 consecutive sequences for the HIV-1 protease (PR) and reverse transcriptase (RT) region. As per the 2009 WHO list of mutations for surveillance of transmitted HIVDR, only one nonnucleoside reverse transcriptase inhibitor (NNRTI) mutation was detected at K101E from all specimens tested, suggesting a low prevalence (<5%) of resistance to NNRTIs and no mutations were detected at other sites, suggesting a low prevalence (<5%) of resistance to nucleoside reverse transcriptase inhibitors (NRTI) and protease inhibitors (PI) drug classes as well. Phylogenetic analysis showed all sequences belonged to HIV-1 subtype C. In the wake of antiretroviral treatment (ART) scale-up, future evaluation of transmitted HIVDR is essential in Kakinada as well as in other regions of India.
Introduction
A
Providing greater care, support, and treatment to a larger number of people living with HIV/AIDS was one of the primary strategies of the third phase of the National AIDS Control Program (NACP-3) toward achieving the goal of halting and reversing the HIV epidemic in India. 3 The National AIDS Control Organization (NACO) of India launched the National ART Program to provide free treatment to HIV-infected individuals in 2004, with eight centers. 4 By April 2010, there were 270 free antiretroviral treatment (ART) centers in India. 5 The national ART program follows a public health approach for treatment and the standardized first line treatment regimen comprises the fixed dose combination of zidovudine or stavudine plus lamivudine and nevirapine. A second line ART regimen was initiated in 2008 and currently 970 patients are on second line ART across 10 centers. 2 The national ART program has expanded since 2004 and as of December 2009, 283,634 people were alive and on ART. 5
The WHO methodology for assessment of transmitted HIV drug resistance recommends a focus on a specific geographic area in which ART has been widely available for 3–10 years. It utilizes a maximum of 47 specimens to assess the prevalence of transmitted resistance to nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors (PIs) as above or below two thresholds, 5% and 15%. 6 More than one site can be included within a geographic area, as long as the population group assessed is the same. Eligibility criteria [newly diagnosed HIV-1-infected primigravida, age <25 years, and no reported antiretroviral drug (ARV) experience] were developed to minimize the risk of including participants infected with HIV many years previously, and with previous ARV experience. 6
Kakinada is the district headquarters of the East Godavari district of Andhra Pradesh state (Fig. 1). It is a large industrial port city, situated at the east coast of India, with a population of 376,861 (2001 census). 8 Andhra Pradesh is one of the high HIV prevalent states of India, with an estimated adult HIV prevalence of 0.9%. 1 In the capital city of Hyderabad in Andhra Pradesh, the nationally sponsored free ART program has been available since 2004; it became available in Kakinada in 2006. Since 1996, ART has been available in the private sector in India. Hence, this site was one of the ideal locations to assess the prevalence of transmitted HIV DR. The HIV prevalence among pregnant women attending the ANC clinic at Rangaraya Medical College in Kakinada [where the HIV Drug Resistance (HIVDR) survey was done] varied from 3% in 2004 to 2.5% in 2008. 9 During the initial site assessment done in 2006, considering the HIV prevalence of 2.8% at that ANC clinic, and considering the high proportion of young (15–24 years) pregnant women, it was thought that the required sample size could be achieved within a year.
Location of Kakinada in Andhra Pradesh, India.
Preliminary site assessment ensured that the site had excellent record maintenance practices, adequate staff (including a medical officer, counselors, and laboratory technician), adequate facilities for initial specimen processing and storage of specimens at −20°C, and willingness of the staff to participate in the survey. Though the site had a regular power supply, there was no facility for power backup in the case of power failure. In addition, the geographic situation of Kakinada made it a site that was not easy to access. One of the reasons for selecting this site for the HIVDR survey was therefore to gain experience in conducting an HIVDR survey in an area with less well-established infrastructure/access.
During the initial course of the survey, two new Prevention of Parent to Child Transmission (PPTCT) centers (one at Ramchandrapuram and another at Rajahmundry) were operationalized in the vicinity of the Kakinada, due to which it was found that the enrollments were declining. Based on consultations with the local medical officer and assessment of the sites by central coordinators, it was decided to include eligible pregnant women from these two centers as well, which were 30 km and 60 km from Kakinada.
With the rapid scale-up of the national ART program as well as its availability and widespread use, there was the potential risk of the emergence of drug-resistant HIV strains, which could thus jeopardize the longer term success of the ART program in India. Emergence of drug resistance may be either transmitted or acquired. The WHO HIV Drug Resistance Network (HIV ResNet) recommended periodic population-based assessment of transmitted HIVDR among individuals recently infected with HIV. 6 To ensure the success of the first line treatment regimen, India was committed to a countrywide strategy for the prevention and monitoring of HIVDR. The first survey to systematically evaluate the transmitted HIVDR in India, done among newly diagnosed Voluntary Counseling and Testing Center (VCTC) clients in Mumbai, showed a low (<5%) prevalence of HIVDR for relevant antiretroviral drug classes. 7 Continued systematic assessment of the emergence and transmission of HIVDR was recommended across the country. The current study described the second such systematic evaluation for transmission of HIVDR that was carried out among newly diagnosed HIV-1-infected primigravida women, in whom it is likely that the infection had occurred recently, attending the PPTCT centers in Kakinada, Andhra Pradesh.
Materials and Methods
A binomial sequential sampling method is recommended for the HIVDR threshold survey, which classifies HIVDR prevalence as low (<5%), medium (5–15%), or high (>15%). The maximum sample size is 47 consecutive specimens, which is sufficient to classify HIVDR prevalence in one of the three categories. However, sampling can be stopped before reaching the maximum sample size if the HIVDR prevalence can be classified as low or high with the data available using the HIVDR threshold analysis method. 6,11
Informed consent was obtained from every client before blood was collected for HIV testing. No additional consent was obtained for the HIVDR threshold survey as subsequent testing for HIVDR used unlinked and anonymous procedures. Survey eligibility was assessed among newly diagnosed HIV-1-infected primigravida women, 15–24 years of age, who were residents of Kakinada and consecutively attending the PPTCT center. To avoid repeat enrollment of the same individual, only those women were assessed who attended the PPTCT center for the first time during the survey period. Asymptomatic pregnant women who had no prior history of any HIV/AIDS-related illness or of receiving any antiretroviral drug (whether informally or formally) for treatment or for prophylaxis were considered potentially eligible for inclusion in the survey. The blood specimens from pregnant women diagnosed with HIV infection at the PPTCT center were ultimately included in the HIVDR survey.
At the PPTCT center, a routine opt-out approach was being followed. Thus, all the pregnant women attending the ANC clinic were provided with pretest counseling followed by testing, which in turn was followed by posttest counseling. Blood specimens were collected as per routine PPTCT procedure from all consenting pregnant women. For the purpose of the HIVDR survey, an additional 5 ml of blood was collected in an anticoagulant EDTA tube from those women who were potentially eligible for inclusion in the survey. For each of the potentially eligible pregnant women, key demographic variables including age, risk factors, area of permanent residence, parity, and gravidity were abstracted from the corresponding PPTCT record onto a standardized form.
During routine HIV testing, if a potentially eligible specimen was found to be positive for HIV, the corresponding additional blood specimen was marked as eligible for HIVDR testing. It was assigned a unique HIVDR survey code and centrifuged for separation of plasma. To ensure the quality of the HIVDR survey, training of the site personnel, including the medical officer and counselors, was done for the study protocol, emphasizing the identification of eligible individuals, data abstraction, and record keeping. The laboratory technician was trained for additional sample collection, processing, storage, and monthly transport of samples to the Central Laboratory at the National AIDS Research Institute (NARI), including record maintenance. Frequent visits were made by the representative of NARI as well as WHO to monitor the implementation of the survey as per the protocol and also to provide supportive supervision. This survey was approved by the ethics committee of the NARI and Indian Council of Medical Research (ICMR).
Plasma aliquots were stored in cryovials and frozen at −20°C at the PPTCT site laboratory and transported on dry ice to the National AIDS Research Institute, Pune for HIV-1 genotypic drug resistance testing within 30 days of sample collection. Genotypic resistance testing was performed using the ViroSeq HIV-1 genotyping Version 2.0 kit (Abbott, Wiesbaden, Germany) and ABI 3100 Genetic analyzer (Applied Biosystem, Foster City, CA). Sequence data were edited using ViroSeq software (Version 2.7). The edited sequences included the region coding for protease (codons 1 to 99) and reverse transcriptase (codons 1 to 335). The sequence alignment was done by Gene Cutter software (
To categorize the prevalence of transmitted HIVDR to each relevant antiretroviral drug class, the WHO HIVDR Threshold Survey analysis method was utilized.
6,11
In this low-resource surveillance methodology, the prevalence of transmitted resistance was categorized as above or below a threshold level, rather than a point estimate with confidence intervals. By employing a binomial sequential sampling method, this approach permitted the classification of transmitted HIVDR for each drug class at thresholds of <5%, 5–15%, and >15% using a maximum of 47 specimens. Sequences were analyzed in the order of specimen collection. The threshold classification was made for each specific drug class when the total number of specimens with relevant mutations fell below a lower limit or above an upper limit for the number of sequences analyzed. For this survey, the sequences were analyzed according to the WHO recommendations using the Calibrated Population Resistance (CPR) tool of the Stanford University HIV Drug Resistance Database (
Results
Between August 2007 and February 2009, plasma specimens for the HIVDR Threshold survey were collected from 56 eligible pregnant women. The median age of the women was 20 years. A total of 51 specimens were processed for sequencing, out of which four could not be amplified while 47 were successfully sequenced.
As per the WHO SDRM list (2009), analysis of 47 consecutively collected specimens revealed no mutation for NRTIs or PIs; only one sequence showed the presence of the NNRTI mutation at position K101E. Since the lower limit for the number of sequences with relevant mutations among the first 47 sequences was two, transmitted HIVDR to all the three drug classes could be classified as low (<5%) in this survey. 11
Several polymorphic amino acid substitutions were, however, noted in both the protease and reverse transcriptase regions (Tables 1 and 2). For the 47 specimens that were amplified and sequenced successfully, all sequences clustered phylogenetically with HIV-1 subtype C (Fig. 2), the predominant subtype circulating in India.
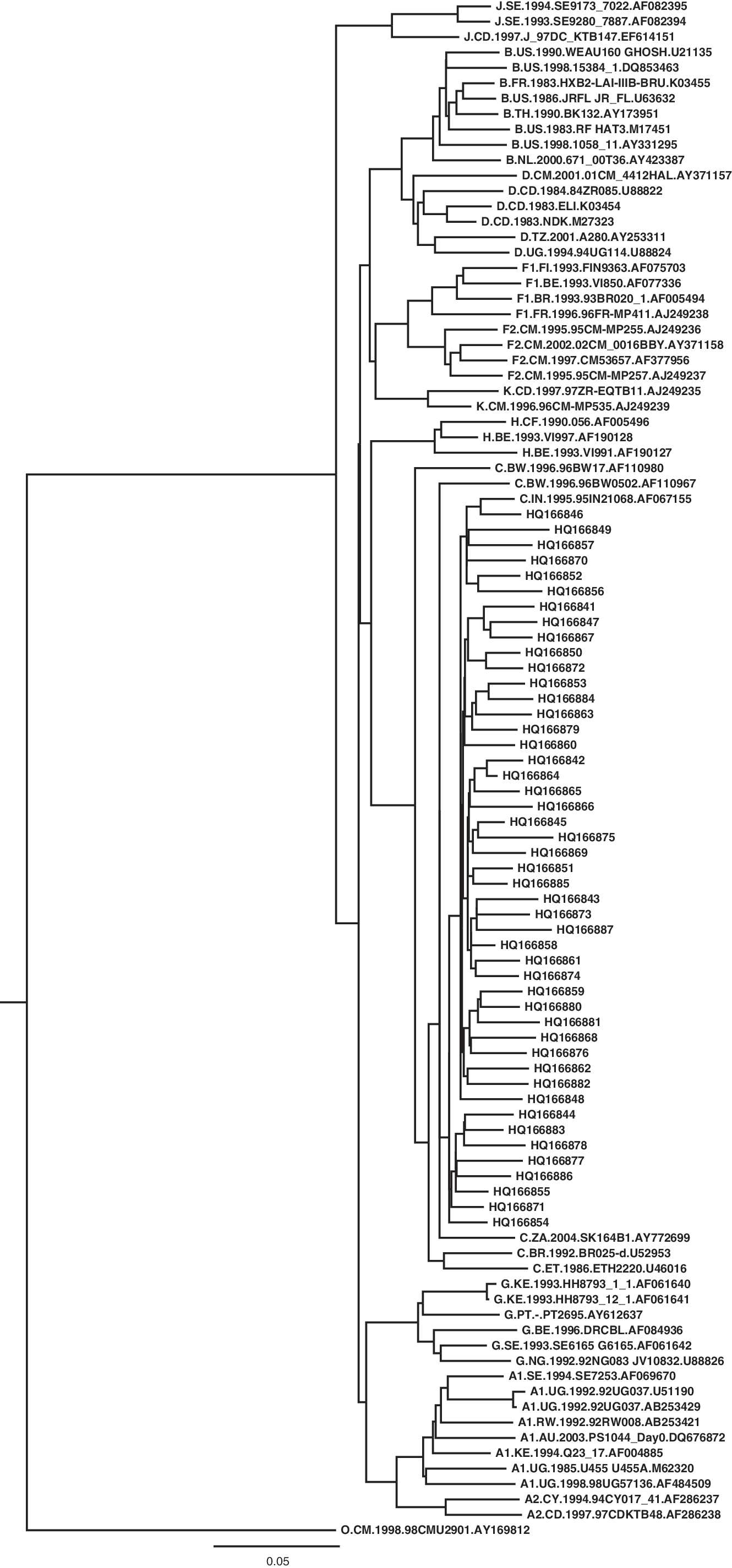
Phylogenetic tree of 47 HIV-1 pol sequences from Kakinada along with reference sequences using PhyML software.
The codons for HIV-1 protease are shown as single-letter amino acid codes followed by specific amino acid positions for the consensus B sequence.
The specific amino acid substitutions are shown as single-letter amino acid codes followed by an Arabic numeral denoting the number of HIV-1 sequences with the substitutions.
The codons for HIV-1 protease are shown as single-letter amino acid codes followed by specific amino acid positions for the consensus B sequence.
The specific amino acid substitutions are shown as single-letter amino acid codes followed by an Arabic numeral denoting the number of HIV-1 sequences with the substitutions.
RT, reverse transcriptase.
Discussion
This study represented the first survey of the estimation of the prevalence of transmitted HIVDR among newly diagnosed HIV-1-infected primigravida women from three PPTCT sites at Kakinada in India and it was a second such survey systematically evaluating the transmitted HIVDR in India. Analysis of the first 47 consecutively collected specimens revealed no NRTI or PI mutations from the 2009 WHO list of mutations for the surveillance of transmitted HIVDR. 12,13 However, as per the 2009 WHO list of mutations for the surveillance of transmitted HIVDR, one sequence among the 47 analyzed had the NNRTI mutation K101E. Although this was located at a polymorphic position, it was included in the list because of its substantial contribution to resistance to commonly used or new NNRTIs. 12 The K101E mutation conferred intermediate resistance to nevirapine and delaviridine and low level resistance to efavirenz and etravirine. 12 Because the lower limit for the number of sequences with pol gene mutations among the first 47 sequences was two, the transmitted NNRTI resistance was classified as <5%. 11 Therefore, the prevalence of transmitted HIV drug resistance for all as well as for each of the three drug classes (NRTI, NNRTI, and protease inhibitor) could be classified as <5% among the newly diagnosed HIV-1-infected primigravida women attending the ANC clinic in Kakinada, India.
Threshold surveys performed in developing countries such as Ethiopia, Swaziland, Malawi, Tanzania, and Uganda among recently HIV-1-infected pregnant women have reported a low prevalence of transmitted HIVDR, 6,14 consistent with our findings.
To enroll the required number of eligible women, the survey needed to be extended and was one of the most important rate-limiting steps of the entire survey. From our experience, we strongly believe that enrolling a sufficient number of eligible newly diagnosed HIV-1-infected primigravida women, which was so crucial for the study, was actually extremely difficult to achieve even when it was factored a priori during site assessment. Future studies should definitely take into account this aspect while assessing the feasibility of a prospective site and should assess the feasibility of including satellite sites and/or extending the duration of the survey. Logistically, extending the survey either in terms of satellite sites or duration would also make it necessary to ensure that adequate training, regular monitoring, and supportive supervision are provided. Transfer out of trained staff during the survey should be avoided.
Kakinada was a remotely located city in which the logistics for specimen transport were limited. The blood specimens in this survey were maintained at −20°C at the site laboratory for which a separate arrangement of power backup was made (for this survey). Plasma specimens were shipped within 1 month of their collection, on dry ice, to NARI. This transport incurred considerable cost as well as facing the difficulty of arranging the dry ice at Kakinada. Therefore, subsequent HIVDR surveys in India at sites with limited options could assess the use of methods other than frozen plasma, such as dried blood spot (DBS), for specimen collection.
Repeat surveys for HIVDR were recommended at the same geographic areas through these sentinel sites to monitor the transmission of HIVDR, while progressively extending to different geographic areas as well as populations with different risk profiles so as to gradually provide information related to the HIV drug resistance pattern in India. In addition to the surveillance of transmitted resistance, NACO also implemented cohort studies at two sites (HIVDR Monitoring surveys) to assess the emergence of HIVDR among those initiating ART. It was also crucial that for the prevalence of transmitted HIV drug resistance to continue to remain low, ART programs should monitor adherence and continuing access to ART, drug quality, drug supply, and prescribing practices to ensure that the emergence of HIV drug resistance was minimized among persons who were on antiretroviral therapy. Systematic evaluation of HIVDR Early Warning Indicators (EWI) to assess ART program factors associated with the preventable emergence of HIVDR is therefore also planned by NACO. Moreover, prevention programs should be active to minimize the transmission of HIV both from persons in treatment and in untreated persons.
With the HIVDR threshold surveys at Kakinada and Mumbai showing a low prevalence of transmitted HIVDR, the current antiretroviral drugs used in the first line ART regimen should continue to be effective if adequate adherence is maintained. With the continued scale of ART, the collection of EWIs as well as surveys at sentinel sites to evaluate transmitted and acquired HIVDR would be important in providing a comprehensive evidence-based recommendation to formulate the overall ART policy in India and thus to ensure the success of the public health approach of ART in India.
Sequence Data
GenBank accession numbers for the Kakinada HIVDR-TS sequences reported in our study were HQ166841 to HQ166887.
Footnotes
Acknowledgments
This study was supported by funds from the World Health Organization South East Asia Regional Office. The National AIDS Control Organization (NACO), Indian Council of Medical Research (ICMR), and Prevention of Parent-to-Child Transmission (PPTCT) centers at Kakinada, Andhra Pradesh provided additional support. We acknowledge the support provided by Dr. Po-Lin Chan from the World Health Organization, India Country Office in New Delhi for her support in completing the work.
Author Disclosure Statement
No competing financial interests exist.