
Abstract
Estimation of HIV-1 incidence is an important public health tool for understanding the status of the epidemic, identifying high-risk populations, and assessing various intervention strategies. Several laboratory-based methods have been developed for distinguishing recent from long-term HIV-1 infection; however, each exhibits some degree of misclassification, particularly among AIDS patients and those taking antiretroviral therapy (ART). To improve upon the limitations associated with measuring responses to a single analyte, we have developed a bead-based, multiplex assay for determination of HIV recent infection based on total antibody binding and antibody avidity to multiple analytes. An HIV-specific, multiplex panel was created by coupling the recombinant HIV-1 proteins p66, gp120, gp160, and gp41 to Bio-Plex COOH microspheres. Longitudinal plasma specimens from recent seroconverters were tested for reactivity to the coupled microspheres using the Bio-Plex 200 System. For each analyte, HIV-specific antibody binding and avidity increased for 1–2 years post-seroconversion, leading to a significant difference in reactivity between recent and long-term specimens. While the potential for misclassification of individuals diagnosed with AIDS or receiving ART appears to be minimal with avidity measures, the impact on total antibody binding was variable, depending on the individual analyte. This bead-based, HIV-specific multiplex assay measures several distinct immune responses in a single assay plate, allowing for sampling of multiple analytes in the determination of recent infection, which could aid in the development of improved statistical methods or algorithms that will more accurately estimate HIV incidence.
Introduction
To date, surveillance of the HIV epidemic has primarily involved enumeration of newly diagnosed infections over a specified interval of time, i.e., cross-sectional descriptions of the prevalence in a given population. HIV prevalence, however, does not provide an accurate representation of the evolution of the epidemic, as duration of infection and predictors of transmission are usually unknown. Estimation of HIV incidence, or the rate of new infections in a population, is essential for monitoring changes in transmission rates, evaluating prevention strategies, and identifying high-risk populations. While HIV prevalence can be measured using standard serological tests, identification of recent HIV infection has proven more challenging.
Janssen et al. were the first to describe the use of a serological testing algorithm for determining recent HIV-1 infection, based on the modification of a standard enzyme immunoassay (EIA). 1 The ability to identify recent infection in cross-sectional samples, as opposed to monitoring seronegative individuals for potential seroconversion, has proven invaluable for HIV surveillance. 2 Several serological assays have since been adapted or developed, relying on the characteristics of the evolving HIV-1 antibody response for differentiation between recent and long-term infection. 3 –5 One such approach involves measurement of antibodies to specific HIV antigens, given that HIV-1 IgG levels increase steadily during early infection. 6,7 For example, the commercially available BED-CEIA measures reactivity to an oligopeptide derived from an immunodominant region of HIV-1 gp41. 8,9 Another approach, as described by Suligoi et al., employs the use of an avidity index (AI), or a measure of antibody reactivity in the presence of a dissociative agent. HIV antibody avidity continues to strengthen during the first 15 months post-seroconversion, allowing for a measurable distinction between recent and established infection. 10
Although use of these laboratory-based assays for the identification of recent HIV-1 infection has facilitated the estimation of HIV incidence, several limitations still exist. Assays based on the evolution of immune responses are subject to some degree of misclassification due to individual variation in antibody production or reactivity and factors that affect the immune response to HIV. Individuals who have progressed to AIDS may be problematic for assays that quantify antibody, given that immunologic failure and subsequent declining antibody levels increase the rate of misclassification as recent infection. 1,9,11,12 Early antiretroviral treatment (ART) has also been shown to prevent the maturation of the HIV-1 antibody response, resulting in lower antibody titers and avidity. 13 –15 Furthermore, assay performance characteristics may vary depending on the subtypes in the target population. Studies indicate that the mean recency duration, or duration of time from seroconversion to recent/long-term cutoff value, may be subtype-specific. 16,17 To circumvent some of the potential problems associated with these individual assays, an additional approach that has been proposed is to use an algorithm of assays for distinguishing recent from established infections. 18,19
To improve upon the limitations associated with serologic measurements of HIV incidence, we developed a novel bead-based, multiplex assay for the determination of HIV-1 recent infection. This assay can simultaneously measure antibody binding and avidity to multiple HIV antigens in a single assay plate, allowing for the estimation of recent infection based on multiple measurements. In this study, the assay performance characteristics are described, using well-characterized specimens from seroconversion panels, AIDS patients, and individuals on ART.
Materials and Methods
Conjugation of recombinant HIV-1 proteins to microspheres
HIV-1 subtype B recombinant proteins p66 (Protein Sciences Corp., Meriden, CT), p24, p31, gp120, gp160, and gp41 (Immunodiagnostics, Inc., Woburn, MA) were conjugated to Bio-Plex COOH microspheres (Bio-Rad Laboratories, Hercules, CA), using a Bio-Plex Amine coupling kit (Bio-Rad Laboratories), according to the manufacturer's protocol. For each coupling reaction, containing 1.25×106 microspheres, 10 μg of recombinant protein was added. Conjugated microspheres were resuspended in phosphate-buffered saline (PBS) with 1% bovine serum albumen (BSA) and 0.05% sodium azide at a concentration of 1×107microspheres/ml and stored protected from light at 4°C. For sample addition and nonspecific binding controls, coupling reactions were also performed using goat anti-human IgG (Invitrogen, Carlsbad, CA) and BSA (Sigma-Aldrich, St. Louis, MO), respectively.
HIV-1 Bio-Plex assay
Plasma samples were diluted 1:50 in preincubation buffer [PBS with 1% BSA, 0.5% polyvinylalcohol (PVA, Sigma-Aldrich), and 0.8% polyvinylpyrrolidone (PVP, Sigma-Aldrich)], as described. 20 Diluted samples were incubated for 15 min at room temperature on a titer plate shaker. A working microsphere mixture was prepared by combining 1×105 microspheres/ml of each coupled microsphere set. The microsphere mixture and prediluted plasma samples were added to duplicate wells of a 1.2-μm filter membrane 96-well plate (Millipore, Danvers, MA) at a volume of 50 μl of each/well. The plate was incubated for 30 min on a shaker with protection from light. Following vacuum aspiration, the microspheres were washed twice with assay buffer (PBS with 1% BSA), resuspended in 100 μl of assay buffer containing 4 μg/ml phycoerythrin (PE)-labeled, goat anti-human IgG (Sigma-Aldrich), and incubated for 30 min on a shaker with protection from light. The microspheres were washed twice, resuspended in 125 μl of assay buffer, and analyzed on the Bio-Plex 200 System (Bio-Rad Laboratories).
A calibrator for the assay was prepared by combining multiple HIV-1-positive samples from commercially available panels. The samples combined to create the calibrator include 12008-13, 9014-5, 9014-7, 9017-11, and 6246-19 (Zeptometrix Corp., Buffalo, NY). The calibrator was added to each assay plate to control for run-to-run variation by normalizing the data. The mean fluorescent intensity (MFI) values obtained by the Bio-Plex System were normalized by dividing by the MFI of the calibrator. Cutoff values were calculated for each analyte to determine antibody positivity. The cutoff values for each analyte were estimated using the following formula: average normalized MFI value of HIV seronegative samples+2 standard deviations.
Calculation of antibody avidity
To estimate antibody avidity, the Bio-Plex assay was performed as described above with an additional incubation step with diethylamine (DEA), following incubation of the plasma samples with the microsphere mixture. Briefly, the microspheres were washed with assay buffer, and 100 μl of 0.1 M DEA was added to two wells for each sample. For a sample-treatment control, 100 μl of assay buffer was added to duplicate wells. The microspheres were incubated for 15 min on a shaker with protection from light, washed twice, and incubated with the PE-conjugate as above.
An avidity index was calculated for each analyte using the following formula: (normalized MFI value of DEA-treated well/ normalized MFI value of buffer-treated well) ×100.
Study cohorts and samples
Initial evaluation of recombinant HIV-1 proteins and assay optimization was performed using commercially available seroconversion panels (Zeptometrix Corp., Buffalo, NY) and an Incidence/Prevalence performance panel (PRB601, Seracare, Milford, MA). Performance characteristics of the Bio-Plex assay were determined by testing plasma samples from HIV-1-infected individuals obtained from various prospective studies (Table 1). Longitudinal specimens from recent seroconverters were collected as part of the Vaccine Preparedness Study for the HIV Network for Prevention Trials (HIVNET). 21,22 The study included high-risk, HIV-negative participants who were monitored by serological testing every 6 months for a total of 18 months. Last negative/first positive Western blot test dates and ART initiation dates, if any, are known for all HIV-1-infected participants. Of the 105 HIVNET study participants evaluated in this study, 67 received ART at some point during follow-up. The timing of ART initiation ranged from immediately following HIV diagnosis up to approximately 2.5 years from the estimated seroconversion date. Ninety-four of the study subjects were included in analyses where ART was excluded, as the subjects were ART naive or samples were available for these subjects at time points prior to the initiation of ART. All HIV-1 infections from the HIVNET cohort are from subtype B virus. For all longitudinal specimens, an estimated date of seroconversion was determined by calculating the midpoint between the last negative and first positive Western blot test dates.
Characteristics of Study Cohorts
Of the 67 subjects, 56 are also included in the HIVNET seroconversion subject count.
MSM, men who have sex with men; ART, antiretroviral therapy.
A second set of longitudinal specimens came from seroconverters identified by the Recruiting Acute Cases of HIV (REACH) study. This study was conducted in Nigeria between May 2003 and March 2010 in collaboration with the Nigerian Federal Ministry of Health (FMOH). Briefly, patients seeking voluntary HIV counseling and testing at a variety of sites in six states in Nigeria consented to HIV serologic testing with a rapid HIV antibody test algorithm, and, if negative, pooled RNA testing using the Roche Amplicor 2.5 HIV-1 RNA assay (Roche Diagnostics, Branchburg, NJ), modified to be used with 25-member pools. Individuals with evidence of HIV-1 RNA and no antibody to the HIV virus were enrolled in the second phase of the study, which included clinical follow-up at 7–10 days, 3, 5, 7, and 9 weeks, and 3, 4, 6, 8, 10, 12, 15, 18, 21, and 24 months after the screening visit. Near full-length genomic sequencing of these specimens has shown that they are predominantly subtypes G and A/G, with several having evidence of multiple recombinations between these subtypes (data not shown).
Long-term (infected>1 year) and AIDS specimens were obtained from a prospective study involving HIV-1-infected men who have sex with men (MSM) with lymphadenopathy syndrome. 23,24 Participants were enrolled in the study in 1982 and 1983 and monitored at 3- to 6-month intervals for clinical and immunological evaluation of progression to AIDS. Since seroconversion dates are unknown, samples were considered long-term if the sample collection date was >1 year from the time of enrollment into the study. Additionally, 254 samples from HIV-seronegative donors, collected as controls for the described study, were tested to evaluate background reactivity to the conjugated microspheres and to determine positive/negative cutoff values for each analyte.
Statistical analysis
Differences in normalized MFI values and avidity index values between known recent and long-term specimens and between long-term and AIDS specimens were evaluated using the Wilcoxon rank sum test. Similar analyses were performed to evaluate the differences in reactivity of long-term specimens from individuals who were untreated versus treated with antiretroviral therapy.
Results
Bio-Plex assay optimization
Initial optimization experiments were performed using the following recombinant HIV-1 antigens conjugated to microspheres: p24, p31, p66, gp120, gp160, and gp41. Commercially available plasma samples of known duration of infection were tested to determine and compare reactivity to recent and long-term specimens. Direct antibody binding to the microspheres and avidity index were measured for each analyte. Reactivity to p24 and p31, including both antibody levels and avidity, showed little or no discrimination between recent and long-term samples (data not shown) and these analytes were not further analyzed. The analytes that provided robust distinction between recent and long-term specimens (data not shown) included p66-normalized MFI value (n), gp120-n, gp160-n, p66-avidity index (a), gp120-a, gp160-a, and gp41-a.
HIV-specific antibody reactivity
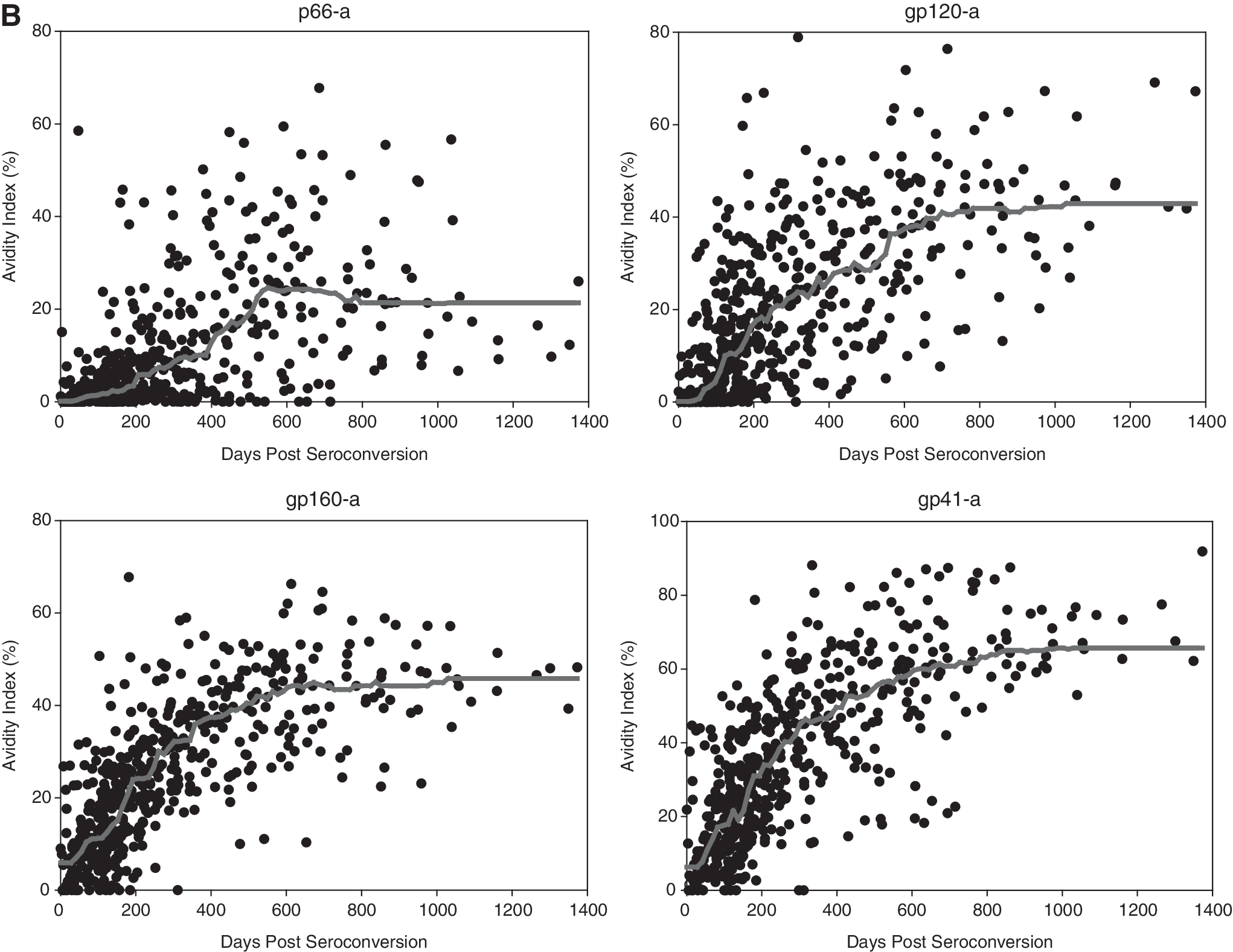
After initial optimization experiments, temporal trends in reactivity were evaluated using longitudinal plasma specimens from recent HIV-1 seroconverters, including 396 subtype B specimens from 95 individuals and 131 Nigerian specimens from 14 individuals. These specimens span a period of up to 1373 days postseroconversion. Normalized MFI values and avidity index for each antigen, plotted over days since seroconversion, are shown in Fig. 1. Smoothed lines, representing the moving median value, are included in each plot to visually demonstrate the pattern of reactivity over time. For all analytes, there is an initial, steady increase in normalized values and avidity index over days since seroconversion, followed by an eventual plateau. Although each analyte displayed a similar temporal pattern, the magnitude and breadth of response vary depending on the particular antigen.

HIV-1-specific antibody reactivity as measured by the Bio-Plex assay. The normalized values
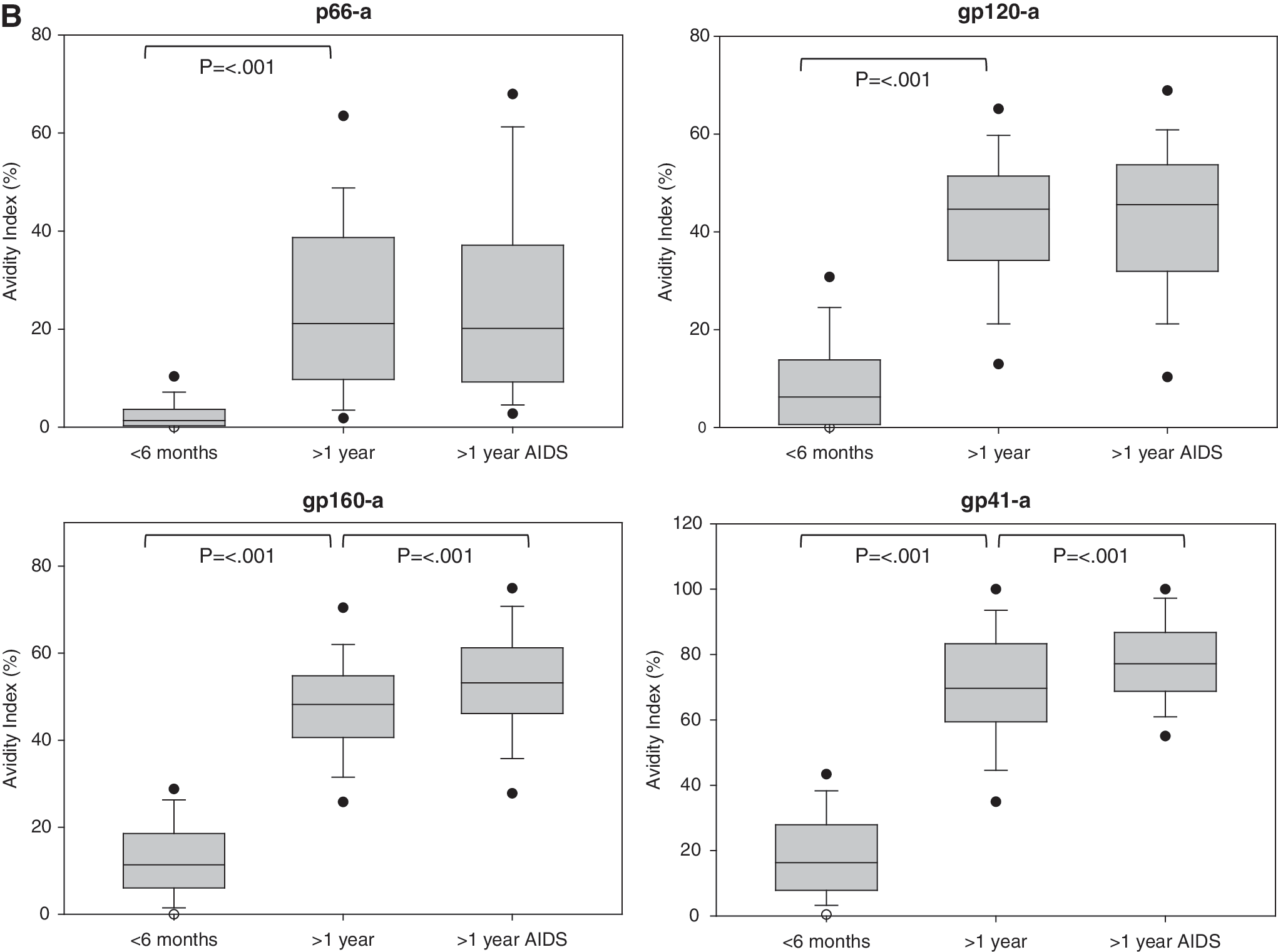
To evaluate the ability of each analyte to distinguish recent from long-term infection, the reactivity of known recent (infected <6 months) and known long-term (infected >1 year) specimens was compared. For comparison purposes, box plots, representing the 25th to 75th percentile and median values, were plotted for the normalized values and avidity index of recent and long-term specimens (Fig. 2). For all analytes, reactivity was significantly higher in the long-term specimens as compared to the known recent (p<0.001). Additionally, the 25th to 75th percentile of reactivity did not overlap between the two groups for all analytes, except p66-n. The distinction between recent and long-term reactivity was greater with the avidity measures as compared to the normalized values.
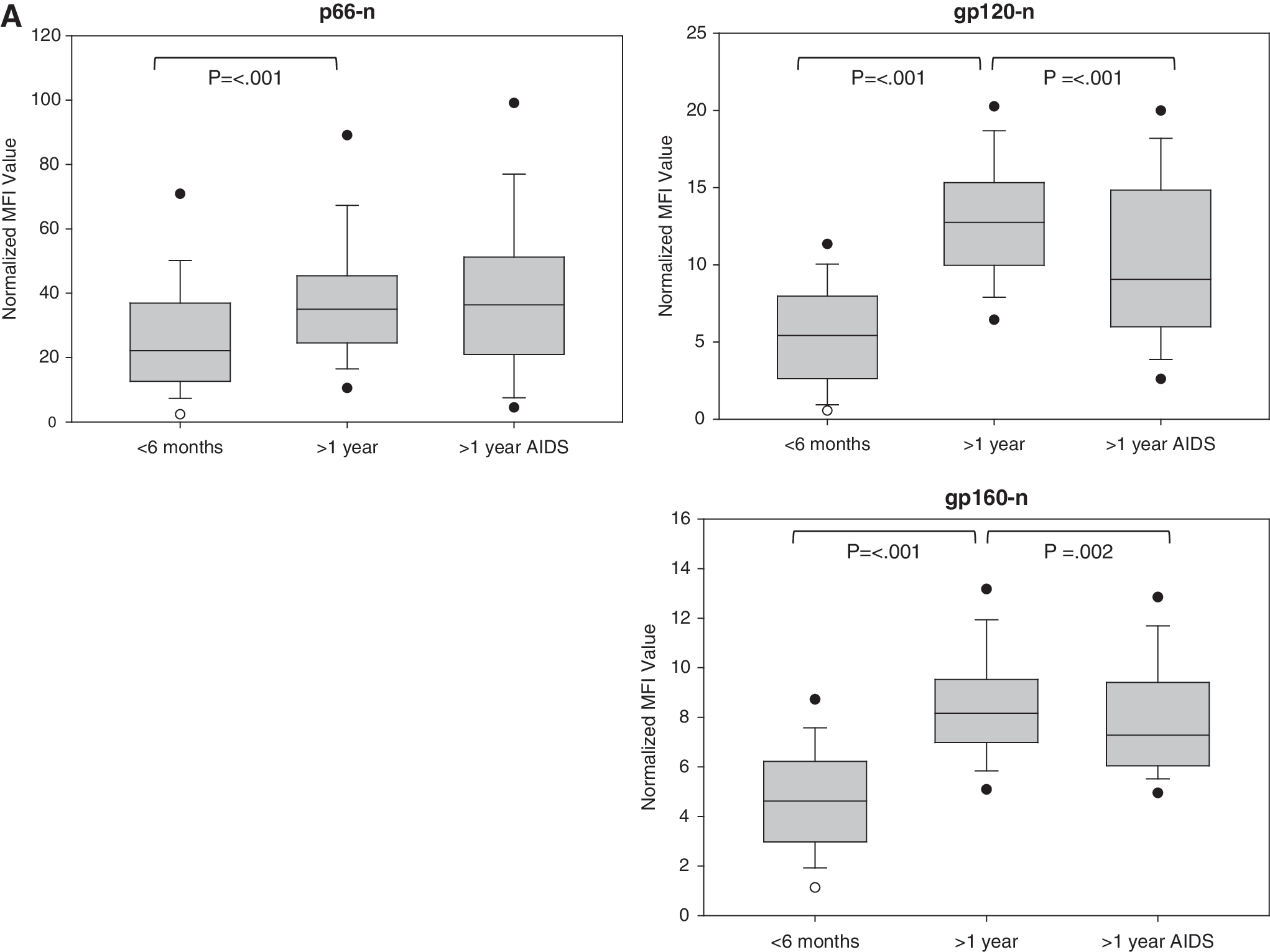
Comparison of known recent, long-term, and AIDS specimens. The normalized values
Effects of AIDS on antibody reactivity
The reactivity of 163 specimens from 68 long-term individuals diagnosed with AIDS was also evaluated (Fig. 2). For all avidity measures, the AIDS specimens showed indices similar to the long-term, non-AIDS individuals, with a measurable distinction between AIDS and recent specimens, indicating no increased risk of misclassification as recent. A significant difference was noted between AIDS and long-term, non-AIDS for gp160 and gp41; however, the avidity index was actually higher for the AIDS specimens. Reactivity was much more variable for the normalized MFI values, with a slight to moderate reduction in median reactivity to p66, gp160, and gp120 (in order of increasing severity) for the AIDS specimens as compared to long-term, non-AIDS. A significant difference between the groups was noted for gp160 and gp120 (p=0.002 and p<0.001, respectively, Fig. 2A).
Effects of antiretroviral therapy on antibody reactivity
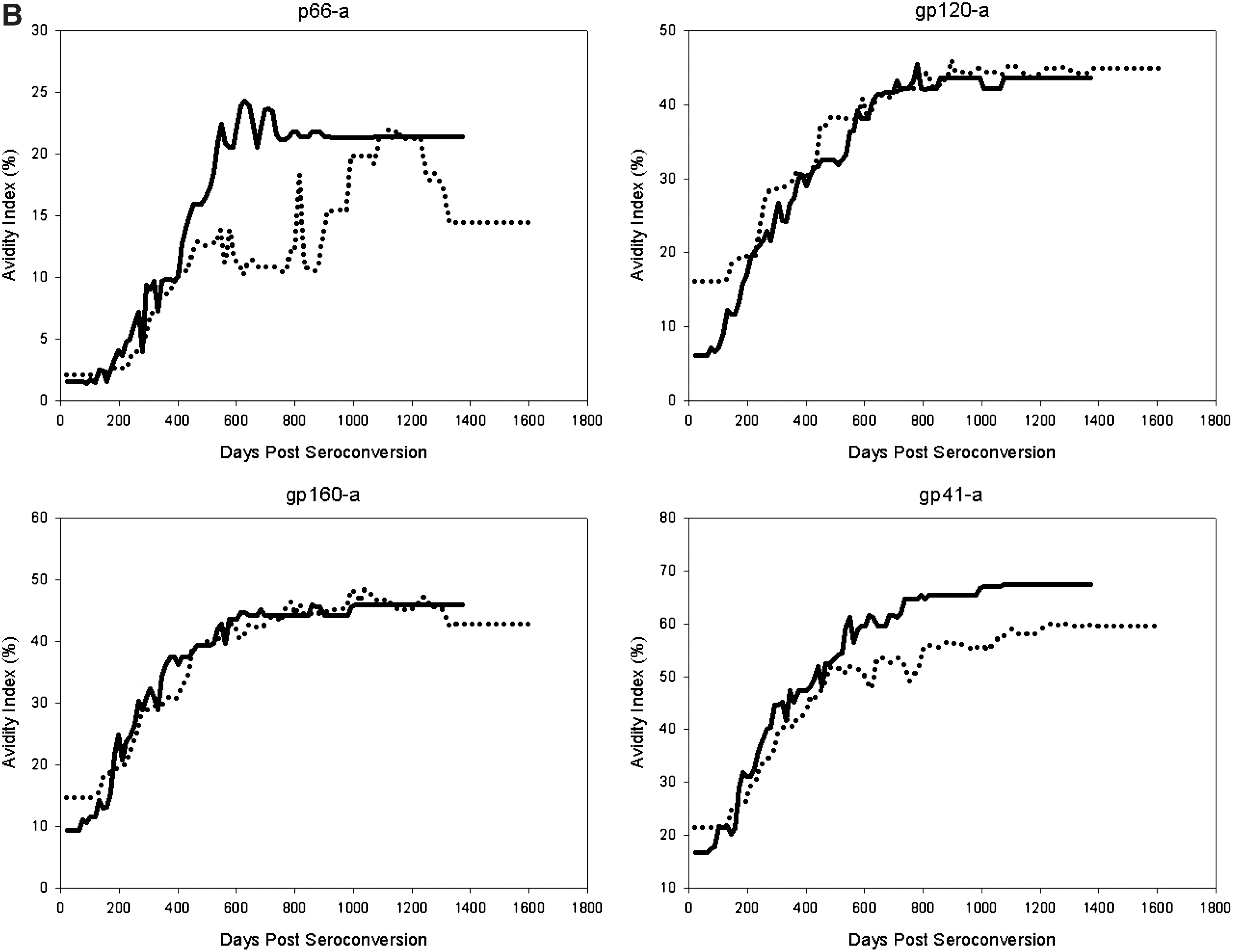
The effect of ART on antibody reactivity, as measured by the Bio-Plex assay, was evaluated using the HIVNET cohort. The reactivity of 396 specimens from untreated individuals (n=95) was compared to that of 394 specimens from individuals receiving ART (n=67). The median normalized values and avidity index over days since seroconversion for both study groups are displayed in Fig. 3. ART was associated with lower median normalized values as compared to untreated subjects for all antigens. This reduction in antibody reactivity, as compared to the untreated subjects, was more apparent at later time points, where the individual would most likely be classified as long-term. Comparison of all long-term specimens (infected >1 year) indicated that reactivity in the ART group was significantly lower than the untreated group for all antigens (p<0.001). The avidity index was less affected by antiretroviral therapy; however, treatment was associated with significantly lower avidity indices for p66 and gp41 in long-term specimens (p=0.021 and p<0.001, respectively).

Impact of antiretroviral therapy on antibody reactivity. The normalized values
Discussion
We describe the development of a bead-based, multiplex assay for the determination of recent HIV-1 infection. This Bio-Plex assay allows for the detection of multiple analytes in one well and measurement of total antibody binding and avidity in the same assay plate. One major advantage of the Bio-Plex system is the ability to rapidly screen multiple analytes with small sample volumes. Additionally, the assay can be easily modified, allowing for the addition or removal of analytes without altering the assay procedure. Our approach is unique in that previously developed assays for detecting recent HIV infection rely on a single assay measure, either HIV-specific antibody levels or avidity, to determine recent infection. Furthermore, most previously described avidity assays have relied on the modification of preexisting, commercially available tests, which may be problematic if a company discontinues manufacturing the product. 10,25,26
In determining cutoff values and the mean recency duration for each analyte, we sought to evaluate assay performance of different candidate analytes using well-characterized longitudinal specimens. Both antibody levels and avidity increase steadily over time, allowing for a measurable distinction between early and late infection. In general, antibodies and/or antibody avidity to the envelope proteins gp120, gp160, and gp41 provided the greatest distinction in reactivity. Surprisingly, gp41 antibody levels exhibited a small dynamic range and, therefore, poor discrimination between recent and long-term specimens. This phenomenon may be explained by the fact that antibodies to gp41 are among the earliest to appear postinfection, 27 leaving a small window to differentiate the reactivity of acutely infected individuals.
Initial analyses suggest that avidity measures are less subject to variation due to AIDS and antiretroviral therapy, which have been shown to be problematic with other assays. 1,11,14 Antibody levels were affected by these “problem” samples to varying degrees, depending on the specific analyte. Further research will determine whether the binding antibody measures will provide any additive value to the assay or whether evaluation of additional analytes is warranted. It is also not known at this point whether the reduction in normalized values associated with AIDS and antiretroviral therapy will lead to an increase in misclassification for this assay. Furthermore, it is likely that the timing of ART initiation postinfection or seroconversion will determine the degree of impact on the performance of the assay. Overall, the Bio-Plex assay described here appears to offer an improvement over other available testing methods.
One of the major challenges of using a single biomarker for estimating HIV-1 incidence in a population is identifying which biomarker accurately determines recent infection. The BED assay, which is the only commercially available assay designed exclusively for the purpose of identifying recent infection, relies on a single optical density reading based on the proportion of IgG that is directed against gp41 oligopeptides. 28 Studies have shown that the BED assay may overestimate HIV incidence in some populations. 17,29 In such populations, the discrepancy between the BED and surveillance-derived incidence estimates led to the issuance of a cautionary statement by UNAIDS, recommending that the assay not be used for surveillance purposes and calling for the evaluation or development of additional assays for determining recent infection. 30 Known causes for discrepant incidence estimates include misclassifications of individuals with advanced HIV infection as recent due to factors that are associated with declining anti-HIV antibodies, such as progression to AIDS or receiving antiretroviral treatment. 31 Additionally, false-recent misclassifications may occur with individuals who never reach the assay threshold or cutoff value despite having established infection. Assay approaches based on a single biomarker leave little room for immunological variation, leading to significant false-recent rates in some settings. 17,32
To improve upon the limitations associated with a single-analyte method for determining recent infection, the use of an algorithm of two or more biomarkers or recent assays for determining recent infection has been proposed. 18,33 We describe an HIV antibody-based Bio-Plex assay, which provides multiple measures for each sample that can be used to develop an intraassay algorithm. The recency status of an individual can be determined based on an antibody reactivity profile, as opposed to relying on a single measure with potentially greater variability.
Given the public health importance of accurately estimating HIV incidence, novel assays aimed at determining recent infection should be developed and carefully validated. We are currently evaluating cutoff values and the corresponding mean recency duration for each analyte. The positive predictive value and false recent rate will be determined for all individual analytes described in this study and compared to various algorithms or combinations of analytes. These data will facilitate selection of the most predictive analytes for further development of the multiplex assay. Furthermore, additional cohorts will be evaluated, including specimens of diverse HIV-1 subtypes. Although no obvious difference in reactivity between B and non-B subtypes (G and A/G) was observed in this study (data not shown), further analysis is needed to look at additional subtypes.
In summary, the bead-based, HIV-specific Bio-Plex assay can measure multiple antibody responses, allowing for consideration of single or multiple analytes in determining recent HIV infection. This assay, which incorporates multiple analytes into a single testing format, could reduce the classification errors often associated with immunological variation and factors that affect the maturation of the serological response to HIV.
Footnotes
Acknowledgments
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.