
Abstract
Few studies have examined the vitamin D status in HIV-infected patients. A cross-sectional retrospective chart review of 2992 HIV-infected patients was conducted from 9/2008 to 5/2009. A total of 274 adult patients had 25-hydroxyvitamin D [25(OH)D] obtained by radioimmunoassay. None was receiving vitamin D (vitD) supplements. Vitamin D status was defined as the following: vitD deficiency (vitDd) as 25(OH)D <25 nmol/liter, vitD insufficiency (vitDi) as 25(OH)D 25–74 nmol/liter, and vitD optimal (vitDo) as 25(OH)D ≥75 nmol/liter. We analyzed demographic/laboratory data. vitDd, vitDi, and vitDo were 21.2% (58 patients, 58/274), 68.6% (188 patients, 188/274), and 10.2% (28 patients, 28/274), respectively. There were significant racial differences. Blacks were 60.3% (35 patients, 35/58), 40.4% (76 patients, 76/188), and 28.6 % (8 patients, 8/28) in vitDd, vitDi, and vitDo, respectively, p=0.002. CD4 T cell count was not different in these three groups. However, HIV viral load was significantly different. Median log 10 HIV viral load was 2.31 with IQR 1.70–409, 1.70 with IQR 1.70–2.96, and 1.70 with IQR 1.70–2.78 in vitDd, vitDi, and vitDo, respectively, p=0.039. Multivariate logistic regression analysis showed that black race [odd ratio (OR) 4.108, 95% confidence interval (CI) 1.462–11.543, p=0.007] and HIV viral load>50 copies/ml (OR 2.396, 95% CI 1.120–5.127, p=0.024) were significantly associated with vitamin D deficiency. Vitamin D deficiency was highly prevalent in HIV-infected patients. Detectable HIV viremia and dark skin (black ethnicity) were significantly associated with vitamin D deficiency. Evaluation of vitamin D status in HIV-infected patients should be considered and further studies are needed to define the effects of vitamin D.
Introduction
Vitamin D is an essential fat-soluble steroid hormone. Humans get vitamin D from exposure to sunlight and from their diet or dietary supplements. Solar ultraviolet B radiation to the skin converts 7-dehydrocholesterol to vitamin D3. Dietary vitamin D is absorbed in the small intestine and it is incorporated into chylomicrons. Both endogenously synthesized vitamin D3 and dietary vitamin D are transported to the liver, where they are metabolized to 25-hydroxyvitamin D [25(OH)D], a major circulating metabolite and a marker for determination of a patient's vitamin D status. 25(OH)D is further metabolized in the kidney by the cytochrome P450 system-mediated (CYP27B1) 25-hydrovitamin D-1α-hydroxylase to its active form, 1,25-dihydroxyvitamin D [1,25(OH)2D]. Bone and skeletal muscle, brain, prostate, breast, and colon tissues as well as immune cells have a vitamin D receptor and respond to 1,25(OH)2D. 1 –3
Vitamin D has been associated with bone growth, regulation of cellular proliferation of both normal cells and cancer cells, differentiation, apoptosis, and angiogenesis. 2 Also recent studies showed that the active form of vitamin D, 1,25(OH)2D, is a potent immunomodulator of both innate and adaptive immunity with receptors found on monocytes, macrophages, as well as T lymphocytes and B lymphocytes. 2,4,5 Low levels of 25(OH)D have been associated with an inability of macrophages to initiate innate immune response. 6
Vitamin D has a significant role in decreasing the risk of chronic illness, including osteoporosis, common cancers, and cardiovascular diseases. 2 These chronic conditions have been increasingly recognized in HIV-infected patients 7 as such patients live longer in the era of highly active antiretroviral therapy (HAART). 8 Vitamin D deficiency has been associated with advanced age, lack of sun exposure, residence at higher latitude, dark skin pigmentation, malnutrition, obesity, and medications leading to increased catabolism of vitamin D such as anticonvulsants and glucocorticoids. 2 In addition, several first-line antiretroviral medications 9 have been associated with altered vitamin D metabolism resulting in lower serum levels of vitamin D. Initiation of an efavirenz-containing antiretroviral regimen has been reported to have decreased levels of 25(OH)D, possibly from efavirenz-induced cytochrome P450 enzymes. 10 Tenofovir has been associated with vitamin D deficiency via tenofovir-linked hyperparathyroidism. 11 HIV protease inhibitors have been shown to impair vitamin D bioactivation by suppressing 25- and 1α-hydroxylase enzymes, which could lead to lower levels of 1,25(OH)2D. 12
Therefore, vitamin D may have an important role in HIV infection, as HIV- infected patients with HAART can live longer and are more likely to develop chronic diseases. However, few studies have examined the vitamin D status in HIV-infected patients. In this study, we examined the prevalence and associated risk factors for vitamin D deficiency among HIV-infected patients in New York City.
Materials and Methods
A cross-sectional observational study was conducted at two urban HIV clinics, Center for Comprehensive Care, St. Luke's-Roosevelt Hospital Center in New York City. From September 2008 to May 2009, serum vitamin D levels were randomly checked. Biochemical testing for vitamin D levels [25(OH)D] was done using radioimmunoassay (ARUP Laboratories, Salt Lake City, UT). Vitamin D status was defined as the following: deficiency as 25(OH)D <25 nmol/liter, insufficiency as 25(OH)D 25–74 nmol/liter, and optimal as 25(OH)D ≥75 nmol/liter. We have adopted this definition of optimal vitamin D levels (≥75 nmol/liter) as growing evidence suggests that vitamin D levels <75 nmol/liter have been associated with an increased risk of osteoporosis and fracture as well as cardiovascular disease and cancer. 2,13 –17 A retrospective medical-chart review was performed.
Demographic characteristics, CD4 T cell count, HIV RNA level, use of HAART, renal function [serum creatinine, estimated glomerular filtration rate (GFR) by Modified Diet of Renal Disease (MDRD)], serum calcium and albumin levels, and body mass index (BMI) at the time of vitamin D level testing were reviewed. Patients were defined as hepatitis B positive if they had a reactive hepatitis B surface antigen test and as hepatitis C positive if they had a reactive hepatitis C antibody serology test at or anytime before the time of checking vitamin D level testing.
Statistical analysis was performed using SPSS, version 15.0 for Windows (SPSS). Continuous variables were compared by the Kruskal–Wallis test and categorical variables were compared by the Linear-by-linear association test to detect differences among three groups of vitamin D status (deficiency, insufficiency, optimal). The Mann–Whitney test was used to compare vitamin D levels between ethnic groups of whites and blacks, stratified by HIV viral load. Multivariate logistic regression was then used to determine factors associated with vitamin D deficiency status. Odds ratio (OR) and 95% confidence interval (CI) were calculated. A p value <0.05 was considered to be statistically significant.
This study was approved by the Institutional Review Board at St. Luke's-Roosevelt Hospital Center, New York, NY.
Results
A total of 2992 patients were evaluated in our center between September 2008 and May 2009 and their medical charts were reviewed. A total of 274 adult patients had their vitamin D levels checked. The study population consisted of 63 females (63/274, 23.0%) with a median age of 47 years. Blacks and Hispanics were the predominant ethnic groups, with 119 patients (119/274, 43.4%) and 83 patients (83/274, 30.3%), respectively. The median CD4 T cell count was 389 cell/mm3. The median log10 HIV viral load was 1.70 and 138 patients (138/274, 50.4%) had an HIV viral load <50 copies/ml. A total of 232 patients (232/274, 84.7%) were receiving HAART. Of vitamin D level measurements (263 patients, 263/274) 96% occurred between October 2008 and March 2009. None of the 274 patients took vitamin D supplements.
These 274 patients were then classified into three groups according to vitamin D levels as vitamin D deficiency group (vitDd) [25(OH)D <25 nmol/liter], vitamin D insufficiency group (vitDi) [25(OH)D 25–74 nmol/liter], and vitamin D optimal group (vitDo) [25(OH)D ≥75 nmol/liter]. The proportions of vitDd, vitDi, and vitDo were 21.2% (58 patients, 58/274), 68.6% (188 patients, 188/274), and 10.2% (28 patients, 29/274), respectively. There were significant racial differences. Whites were 12.1% (7 patients, 7/58), 23.9% (45 patients, 45/188), and 32.1% (9 patients, 9/28) in vitDd, vitDi, and vitDo, respectively, p=0.022. Blacks were 60.3% (35 patients, 35/58), 40.4% (76 patients, 76/188), and 28.6% (8 patients, 8/28) in vitDd, vitDi, and vitDo, respectively, p=0.002. Hispanics were 22.4% (13 patients, 13/28), 33.0% (62 patients, 66/188), and 28.6% (8 patients, 8/28) in vitDd, vitDi, and vitDo, respectively, p=0.329.
The CD4 T cell count was not different in these three groups. The median CD4 T cell count was 390 with IQR 211–647, 386 with IQR 255–552, and 426 with IQR 245–632 cell/mm3 in vitDd, vitDi, and vitDo, respectively, p=0.889. The HIV viral load was significantly different. The median log10 HIV viral load was 2.31 with IQR 1.70–4.09, 1.70 with IQR 1.70–2.96, and 1.70 with IQR 1.70–2.78 in vitDd, vitDi, and vitDo, respectively, p=0.039. Patients with HIV viral load <50 copies/ml were 36.2% (21 patients, 21/58), 53.7% (101 patients, 101/188), and 57.1% (16 patients, 16/28) in vitDd, vitDi, and vitDo, respectively, p=0.026. However, proportions of patients who received HAART were not significantly different in the three groups; 75.9% (44 patients, 44/58), 87.8% (165 patients, 165/188), and 85.7% (24 patients, 24/28) were on HAART in vitDd, vitDi, and vitDo, respectively, p=0.180.
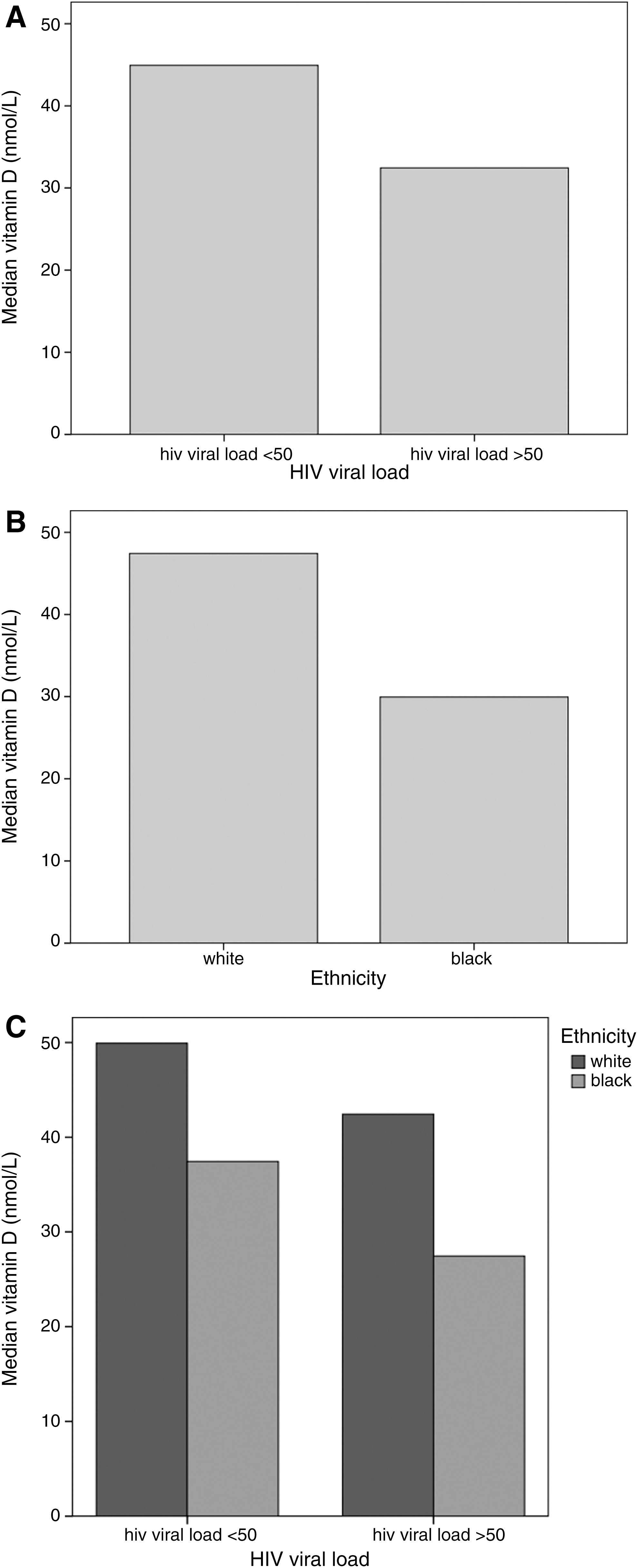
Comparison analyses between patients with detectable HIV viremia (HIV viral load>50 copies/ml) and undetectable HIV viremia (HIV viral load<50 copies/ml) as well as between ethnic groups of whites and blacks were then performed in regard to vitamin D levels. Vitamin D levels were significantly higher in patients with undetectable HIV viremia (median 45 nmol/liter with IQR 30–62 nmol/liter) than in patients with detectable HIV viremia (median 32 nmol/liter with IQR 22–50 nmol/liter), p<0.001. Significant differences in vitamin D levels between ethnic groups of whites and blacks were noted. The median vitamin D levels were 47 nmol/liter with IQR 35–64 nmol/liter and 30 nmol/liter with IQR 22–47 nmol/liter in whites and blacks, respectively, p<0.001.
Analysis of vitamin D levels according to the ethnic groups of whites and blacks stratified for HIV viral load was then performed. Within the black ethnic group, vitamin D levels of patients with HIV viral load<50 copies/ml (median 37 nmol/liter with IQR 25–56 nmol/liter) were significantly higher compared to patients with HIV viral load >50 copies/ml (median 27 nmol/liter with IQR 20–40 nmol/liter), p=0.021. However, no significant differences in vitamin D levels were found in the white ethnic group between patients with HIV viral load<50 copies/ml (median 50 nmol/liter with IQR 35–65 nmol/liter) and patients with HIV viral load>50 copies/ ml (median 42 nmol/liter with IQR 17–63 nmol/liter), p=0.291. These are shown in Fig. 1.
Stratified analysis controlled for HIV viral load<50 copies/ml was then conducted to evaluate the relative contribution of HAART in regard to vitamin D levels. Patients who remained on HAART with HIV viral load<50 copies/ml were analyzed. Combinations of HAART were classified into eight different regimens. The median months of HAART were 16 months with IQR 6–25 months, 19 months with IQR 7–28 months, and 14 months with IQR 7–20 months in vitDd, vitDi, and vitDo, respectively, without statistical difference, p=0.628. Among combinations of HAART, a nonnucleoside reverse transcriptase inhibitor (NNRTI) plus tenofovir (TDF)-based nucleoside/nucleotide reverse transcriptase inhibitor (NRTIs)-based regimen was associated with significant difference. In all, 61.1% (11 patients, 11/18), 30.9% (30 patients, 30/97), and 18.8% (3 patients, 3/16) of patients were on NNRTI plus TDF-based NRTIs in vitDd, vitDi, and vitDo, respectively, p=0.008. No significant differences were found among other combinations of HAART as well as other demographic, clinical, and laboratory variables. These are shown in Tables 1 and 2.
Baseline Characteristics of HIV-Infected Patients According to Vitamin D Levels
Vitamin D deficiency group (vitDd), vitamin D insufficiency group (vitDi), vitamin D optimal group (vitDo).
Age, age median with interquartile range (IQR) (years); ethnicity other, Asian and other ethnic groups; HIV risk factor Hetero, heterosexual contact; IVDU, intravenous drug abuse; MSM, men who have sex with men; Other, transfusion, perinatal and others; Ca, serum calcium levels median with IQR (mg/dl); Albumin, serum albumin levels median with IQR (mg/dl); BMI, body mass index median with IQR (kg/m2); GFR, glomerular filtration ratio (ml/min/1.73 m2) median with IQR; GFR < 60, GFR < 60 (ml/min/1.73 m2); HepB, positive hepatitis B; HepC, positive hepatitis C; HAART, highly active antiretroviral therapy; CD4, CD4 T cell cell count median with IQR (cells/mm3), log10 HIV, log10 HIV viral load median with IQR; HIV < 50, HIV viral load < 50 copies/ml.
Stratified Analysis Controlled for HIV Viral Load < 50 Copies/ml for HAART in Regard to Different Groups of Vitamin D Levels
Vitamin D deficiency group (vitDd), vitamin D insufficiency group (vitDi), vitamin D optimal group (vitDo).
Duration of HAART, duration of highly active antiretroviral therapy (HAART) median with IQR (months); NNRTI, nonnucleoside reverse transcriptase inhibitor; TDF, tenofovir-based nucleoside/nucleotide reverse transcriptase inhibitor; non-TDF, non-tenofovir-based nucleoside/nucleotide reverse transcriptase inhibitor; Others, other combinations of HAART includes using raltegravir, enfuvirtide, etc.
Multivariate logistic regression analysis was then conducted using the variables of age, sex, HIV risk factors, ethnicity, calcium and albumin levels, BMI levels, GFR, presence of hepatitis, CD4 T cell count, HIV viral load, and HAART regimens. Black race [odd ratio (OR) 4.108, 95% confidence interval (CI) 1.462–11.543, p=0.007] and HIV viral load>50 copies/ml (OR 2.396, 95% CI 1.120–5.127, p=0.024) were significantly associated with vitamin D deficiency status while HAART regimens did not show significant correlation in the multivariate logistic regression model, as shown in Table 3.
Logistic Regression Analysis of Variables Associated with Vitamin D Deficiency Status in HIV-Infected Patients
Ethnicity Other, Asian and other ethnic groups; HIV risk factor Hetero, heterosexual contact; IVDU, intravenous drug abuse; MSM, men who have sex with men; Other, transfusion, perinatal and others; Ca, serum calcium levels; Albumin, serum albumin levels; BMI, body mass index; GFR, glomerular filtration ratio (ml/min/1.73 m2); HepB positive, hepatitis B positive with hepatitis B negative as reference; HepC positive, hepatitis C positive with hepatitis C negative as reference; HAART, highly active antiretroviral therapy; NNRTI, nonnucleoside reverse transcriptase inhibitor; TDF, tenofovir-based nucleoside/nucleotide reverse transcriptase inhibitor; non-TDF, non-tenofovir-based nucleoside/nucleotide reverse transcriptase inhibitor; Others, Other combinations of HAART includes using raltegravir, enfuvirtide, etc.
Discussion
Low vitamin D [25(OH)D] levels were highly prevalent in this HIV-infected patient cohort in New York City, in the northeastern United States. Our cohort, an ethnically diverse population with most patients receiving HAART, was likely to represent the current HIV epidemic observed in large cities in the United States. A total of 21.2% of the patients had vitamin D deficiency and vitamin D insufficiency was noted in 68.6%. Only 10.2% of the patients were noted to have optimal vitamin D levels. The results of the present study correspond to previous studies, 18 –22 which reported a high prevalence of low vitamin D levels in HIV-infected patients, between 74% and 91%.
An association with dark skin color (black ethnicity) and vitamin D deficiency was also consistent with earlier studies 11,19,21,22 and remained as a strong predictor of vitamin D deficiency status in the multivariate logistic regression analysis. Also our stratified analysis demonstrated the great contribution of dark skin pigmentation in vitamin D deficiency in addition to detectable HIV viremia.
Our study did not find any relationship between vitamin D levels and CD4 T cell count. These results are in agreement with those of previous studies 19,23 in which no association between vitamin D [25(OH)D] levels and CD4 T cell count was found. However, detectable HIV viremia was significantly associated with vitamin D deficiency. Our hypothesis for this observation is based on the likely interactions among HIV viremia, lipopolysaccharide (LPS), proinflammatory cytokines, and toll-like receptor (TLR) signaling pathways with activation of CYP27B1 (25-hydrovitamin D-1α-hydroxylase) in macrophages.
LPS and proinflammatory cytokines are increased with uncontrolled HIV viremia due to compromised gut-associated lymphoid tissues and increased microbial translocation into the plasma. 24,25 TLR signaling pathways in macrophages are activated by LPS (TLR-4) and HIV viral RNA (TLR-7) leading to more increased levels of proinflammatory cytokines including tumor necrosis factor (TNF) and interferon (IFN)-gamma. 25,26 The latter can induce CYP27B1 (25-hydrovitamin D-1α-hydroxylase) in macrophages synergistically along with activated TLR-2/1 (LPS), which further leads to decreased levels of vitamin D [25(OH)D] 27 by hydroxylation of 25(OH)D into 1,25(OH)2D. This induction of CYP27B1 in macrophages by activated TLR-2/1 was noted even in the absence of vitamin D [25(OH)D], while up-regulation of cathelicidin (an antimicrobial peptide) mRNA and 1,25(OH)2D receptor-specific Cyp24 mRNA did not occur in the absence of vitamin D [25(OH)D]. 6 Taken together, the significance of HIV viremia associated with vitamin D deficiency in our study can be explained by the hypothesis that active HIV viremia induces LPS and proinflammatory cytokines including IFN-gamma, which further induce CYP27B1 directly and indirectly via TLRs, leading to a vicious cycle of positive-feedback loops resulting in lower levels of vitamin D [25(OH)D] without the optimal beneficial effects of activated vitamin D [1,25(OH)2D] from lack of up-regulation of cathelicidin and a specific 1,25(OH)2D receptor. These are shown in Fig. 2.
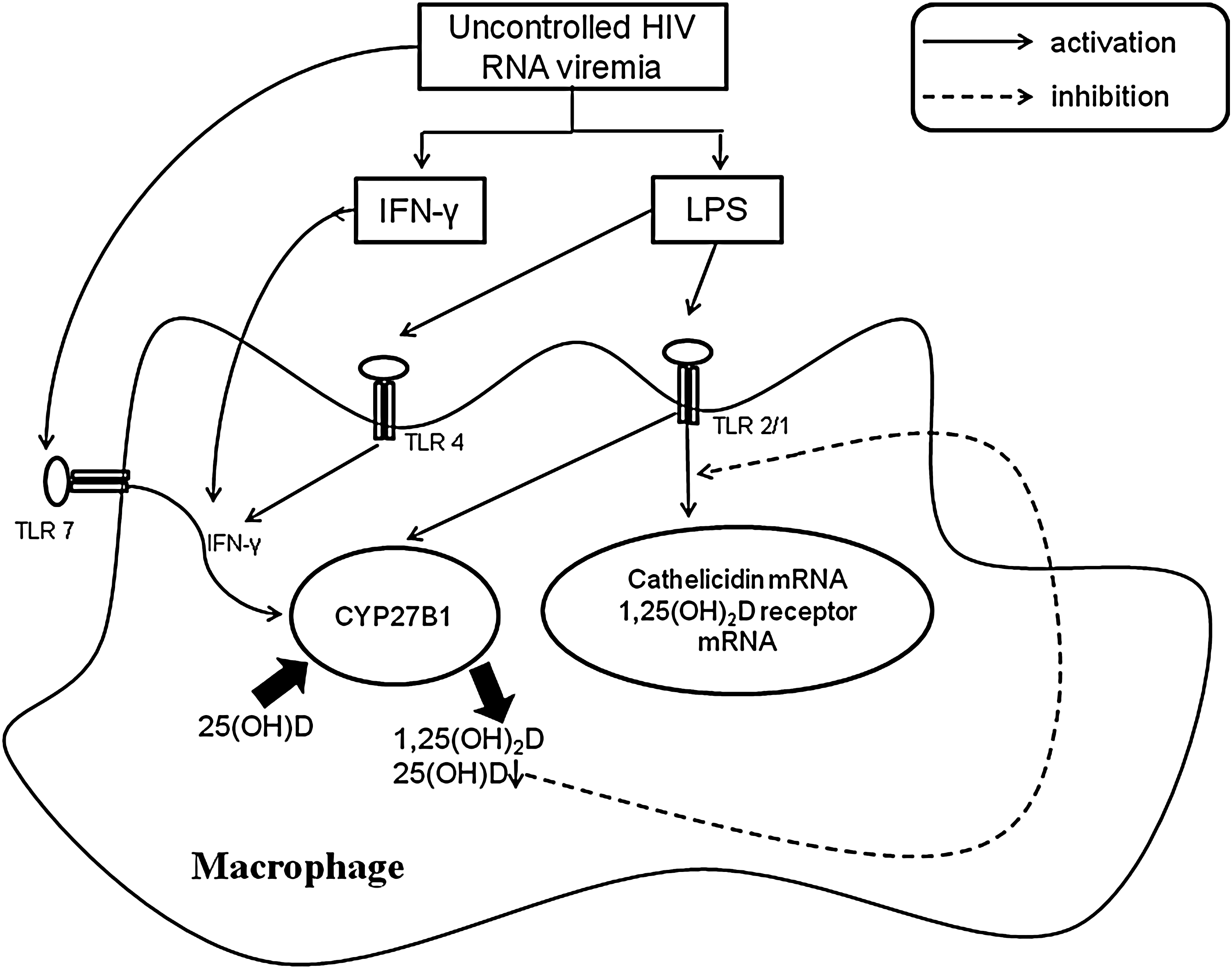
Hypothesis illustrating the role of uncontrolled HIV RNA viremia in the contribution to vitamin D [25(OH)D] deficiency via TLRs in macrophages. Active HIV viremia induces LPS and proinflammatory cytokines including IFN-gamma, which further induce CYP27B1 directly and indirectly via TLRs, leading to lower levels of vitamin D [25(OH)D] without the optimal beneficial effects of activated vitamin D [1,25(OH)2D] from lack of up-regulation of cathelicidin and specific 1,25(OH)2D receptor. IFN-γ, interferon gamma; LPS, lipopolysaccharide; TLR, toll-like receptor; CYP27B1, 25-hydrovitamin D-1α-hydroxylase.
Although HAART comprising different regimens was not one of the significant predictors for vitamin D deficiency in our multivariate logistic regression analysis, a stratified analysis, controlled for HIV viral load<50 copies/ml, revealed a significant association with vitamin D deficiency and HAART (an NNRTI and TDF-based NRTI regimen). NNRTI including efavirenz has been associated with vitamin D [25(OH)D] deficiency 18,19,22 on the basis of the induction of CYP3A4 and CYP24 as well as the reduction of CYP2R1 transcription, which may result in decreased vitamin D levels. 22 TDF has been linked to hyperparathyroidism in the presence of vitamin D deficiency. 11,28 Parathyroid hormone (PTH) increases the metabolism of 25(OH)D to 1,25(OH)2D, which further exacerbates vitamin D deficiency. 2 Therefore, our results suggest that an NNRTI plus TDF-based antiretroviral regimen could further increase vitamin D deficiency by the additive effects of NNRTI-induced vitamin D deficiency plus TDF-induced hyperthyroidism in the presence of vitamin D deficiency.
This study has some limitations, however, mostly stemming from its cross-sectional retrospective study design and the fact that it is limited to a single medical center experience in the northeastern United States. Of vitamin D level measurements 96% occurred from October 2008 to March 2009, which might have been resulted in slightly lower vitamin D levels in the patients due to seasonal variations of less exposure to sunlight during the study period. Lack of 1,25(OH)2D, CYP27B1 level, PTH, and alkaline phosphatase (ALP) measurements prevented further analyses to test the hypothesis of HIV viremia and activated vitamin D [1,25(OH)2D] via induction of CYP27B1 and to identify possible additive effects from TDF on secondary hyperparathyroidism in the presence of vitamin D deficiency.
Although our study showed that the prevalence of vitamin D deficiency was higher in Hispanics than in whites, it did not show a statistical difference largely due to a lack of information on skin pigmentation of Hispanics due to the retrospective nature of the study. Because skin pigment absorbs sunlight, 29 an important source of vitamin D, blacks as well as Hispanics are considered to be at risk for vitamin D deficiency depending on their levels of skin pigmentation. Nonetheless, the diversity of the patient population with access to care likely represents the current trend of the HIV epidemic in large cities in the United States as well as other developed countries, such as in Europe.
Although there might have been some slight seasonal and geographic variations of vitamin D levels, our study results have provided valuable assistance for evaluating the prevalence of vitamin D deficiency in HIV-infected patients with identifying risk factors. In summary, we found that vitamin D deficiency was highly prevalent in HIV-infected patients. Detectable HIV viremia and dark skin (black ethnicity) were significantly associated with vitamin D deficiency. Among different combinations of HAART, use of an NNRTI and TDF regimen was associated with vitamin D deficiency in patients with HIV viral load<50 copies/ml. Therefore, HIV-infected patients may benefit from vitamin D supplementation and vitamin D status should be evaluated in HIV-infected patients, especially in patients with dark skin and/or detectable HIV viremia to diagnose vitamin D deficiency and offer treatment early.
Further prospective studies involving larger number of HIV-infected patients are needed not only to define the effects of vitamin D on PTH, HAART, and innate immune response against progression of chronic HIV infection and other chronic diseases, but also to define the optimal management of vitamin D deficiency.
Footnotes
Author Disclosure Statement
No competing financial interests exist.