
Abstract
A prospective study was conducted in 4339 HIV-positive clients at the Thai Red Cross AIDS Research Centre (TRC-ARC) Anonymous clinic, Bangkok, Thailand between January 2003 and April 2008. A tuberculin skin test (TST) was done for all patients without a previous history of tuberculosis (TB). Nine months of isoniazid (INH) was given for all positive TST/no active TB. TST-negative clients were asked to repeat the TST annually. The study aim was to evaluate the feasibility and efficacy of INH prophylaxis for preventing TB in HIV-positive Thai patients. Of those patients, 4111 (94.7%) had a TST done; 1157 (28.1%) were TST positive and 799 patients started INH prophylaxis. In all, 551 (69%) and 633 (79.2%) patients completed 9 months and 6 months of INH, respectively; 176 (20.2%) patients had a negative TST at baseline and subsequently converted to positive. Only patients with a baseline CD4 >200 cells/μL (p=0.000) and currently on antiretroviral (ARV) treatment (p=0.000) were related to having a positive TST. This baseline CD4 level was also significantly related to higher INH completion rates at 6 months (p=0.000). Interestingly, none of INH completion patients developed active TB. The feasibility of INH prophylaxis in TST-positive patients in this setting is possible. However, the long-term advantage of INH prophylaxis in terms of TB prevention, especially in HIV-1-infected patients on highly active antiretroviral therapy (HAART), is still an issue that needs more research.
Introduction
Tuberculosis (TB) has long been one of the major public health problems in most developing countries, including Thailand. The problem was driven by the wide spread of HIV infection, which facilitates reactivation of latent TB 1 ; at the same time, TB accelerates HIV disease progression. 2 In Thailand, TB is the most common and devastating of the AIDS-defining diseases, as well as the leading cause of morbidity and mortality among HIV-infected individuals. 3 In other words, HIV infection is the strongest known risk factor for developing TB. 4 Moreover, up to 50% of HIV-infected patients diagnosed with TB died during TB treatment due to a TB-associated condition (i.e., immune recovery syndrome, drug resistant TB) (27%), an HIV-associated condition other than TB (35%), and a condition not related to TB or HIV (15%). 5
Therefore, there is a growing concern involving latent TB in people with HIV. Even though the risk of reactivation of latent TB is low in healthy individuals, it is greatly increased in individuals with advancing immunodeficiency, mostly due to HIV infection. 6 The prevalence of latent TB in Southeast Asia was around 46%, which was much higher compared to Europe (14%) and the United States (15%). 7 Latent TB infection is defined by a positive tuberculin skin test (TST) and exhibits no clinical symptoms of TB. 8 Even though the PPD test has limited sensitivity and specificity in advanced HIV-infected individuals, 9 –11 an induration of ≥5 mm is indicative for preventive treatment of latent TB. 12 Reports from Haiti, 13 –15 Uganda, 16 Kenya, 17,18 Zambia, 18 and the United States 19 have shown isoniazid (INH) to be effective in treating latent TB, with a rate as high as 62% in reducing tuberculosis in positive TST individuals [RR, 0.38 (95% CI 0.25–0.57)]. However, the durability of preventive therapy remains unclear, especially in those studies that were conducted before the advent of highly active antiretroviral therapy (HAART). A study from Zambia 20 showed that the risk of developing TB in individuals on INH and rifampicin/pyrazinamide (RIF/PZA) increased over time but remained significantly lower than the placebo arm during the first 2.5 years but not subsequently. TB preventive therapy is also associated with a reduced mortality among individuals with positive TST (26% for INH alone and 31% for INH/RIF). 21 It has been proven that INH prophylaxis (isoniazid preventive therapy, IPT) can be used to treat latent TB infection and its efficacy was equivalent to rifampicin plus pyrazinamide but with a lesser risk of developing severe adverse side effects. 22 Even though IPT is normally used in developed countries and is recommended by WHO, many developing countries with a high TB burden, including Thailand, refuse to widely implement such a program. This hesitation is due to concerns involving drug resistance since there are a limited number of TB drugs currently available in the market. Also, there are limited data on how best to exclude active TB prior IPT treatment to reduce the risk of INH resistance.
As a result of this, the Thai Red Cross AIDS Research Centre Anonymous Clinic (TRC-ARC) started a program using INH prophylaxis for HIV clients in January 2003. This service was added to the exiting voluntary counseling and testing (VCT) for HIV and other services: anonymous CD4, viral load, and primary prophylaxis against Pneumocystis jirovecii pneumonia (PCP), and cryptococcal meningitis. 23 Hence, in this study, we assessed the feasibility and the effect of TST and IPT on the incidence of TB in the HAART era in Thailand, in an area highly endemic for TB.
Materials and Methods
The TST and IPT program, involving a prospective, observational cohort of HIV-infected individuals, was conducted at TRC-ARC, Bangkok, Thailand. All HIV-positive clients attending the TRC-ARC Anonymous clinic after January were asked to participate in this program. Screening for previous TB was done through an interview conducted by the staff and the use of a questionnaire. TST was done for all clients without a previous TB history. To rule out active TB in clients who were TST positive, ≥5 mm induration, chest x-rays and sputum examinations were done at nearby health centers. If the results were positive, clients were referred to a designated hospital for further examination and treatment. On the other hand, if the results were negative and serum alanine aminotransferase (ALT) (serum glutamate pyruvate transaminase, SGPT) was below 2.6 times the upper normal limit, INH was administered for 9 months. The toxicity of INH was monitored by SGPT at baseline and at 3 months and 6 months after starting INH. The severity of SGPT was graded by using the ACTG grading criteria. Terminating INH treatment depended on the physicians and the severity of clinical and laboratory adverse events. TST-negative clients were asked to repeat the TST test annually. A history of active TB was followed annually (up to 3 years) for all participants.
Information obtained from the questionnaire and laboratory test results were recorded in two separate Microsoft Access databases version 2003, which were linked by a number assigned to each client at the time of first contact with the clinic.
The data were analyzed retrospectively by using the SPSS program version 15.0. Data were presented as means (SD), medians (IQR), or percentages in tables and bar graphs.
Multivariate analysis using logistic regression was performed to obtain factors predicting a positive TST test result, TST test conversion, and completion of INH prophylaxis. All tests were two sided and α<0.05 was considered statistically significant.
Results
Patient characteristics
From January 2003 to April 2008, there were a total of 7670 visits (the median was 2 visits per client while the mean was 1.8 visits per client) to the Thai Red Cross Anonymous TB clinic by 4339 clients. There were 2500 (57.6%) males and 1839 (42.4%) females. The mean (SD) age was 33.5 (8.1) years. The median (IQR) age was 33 (28–38) years. Only 148 (3.6%) patients were over 50 years old. As for CD4, around 3 months before or after the date of the TST test, the mean (SD) CD4 was 303.6 (222.6) cells/μL and the median (IQR) CD4 was 283 (124.5–435) cells/μL.
A total of 984 clients (22.7%) reported that they were on antiretroviral (ARV) treatment at the time of the TST test. The median CD4 within 3 months of the TST test was 292 cells/μL and 235 cells/μL for participants reported not on ARV and on ARV treatment, respectively. A flow scheme of patients is shown in Fig. 1.
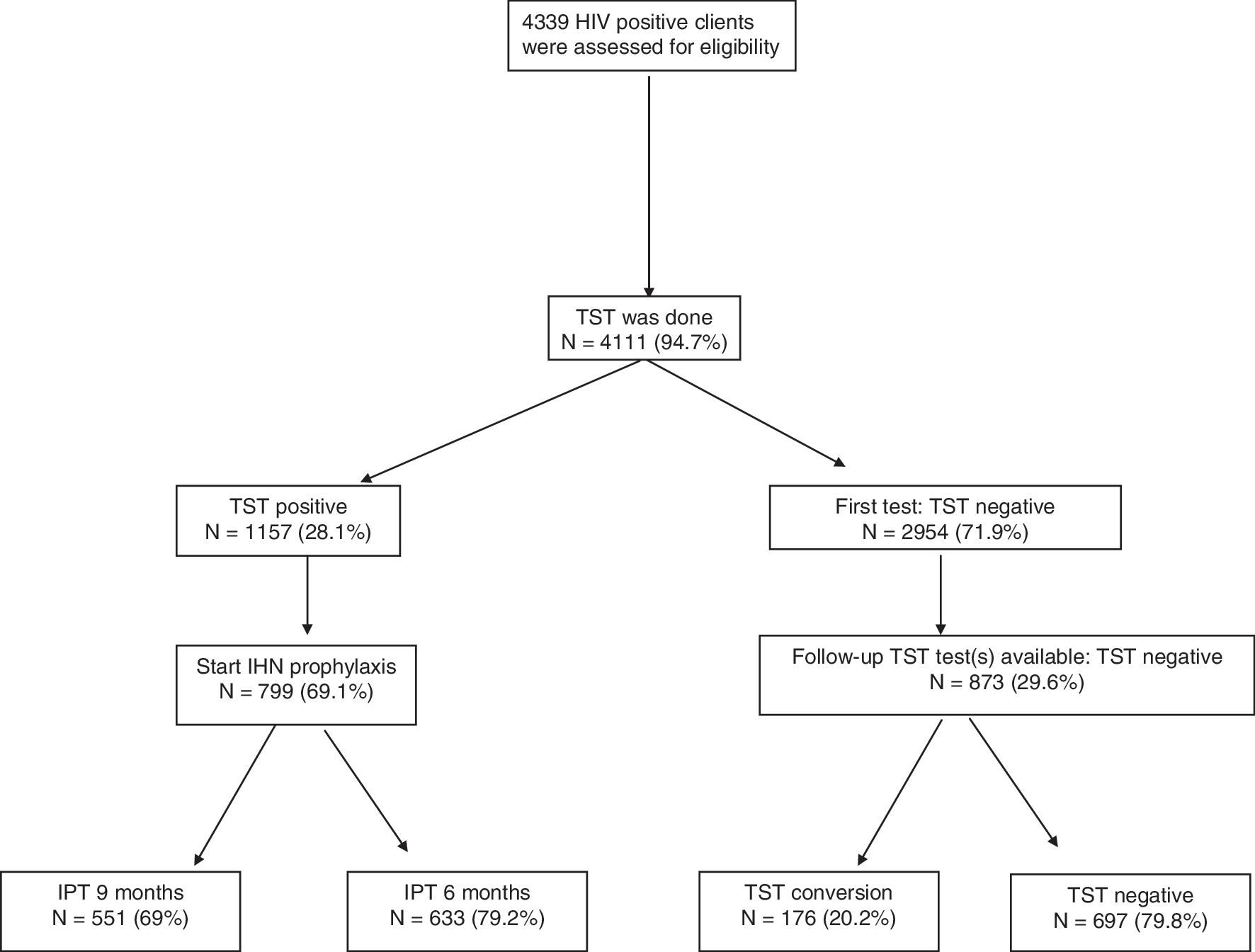
Patient flow.
History of TB prior to entering the study
Regarding a past history of TB treatment and TB contact, 4111 patients (94.7%) reported having no history of TB treatment. Only 14 (0.3%) and 45 (1.1%) had latent TB treatment and active TB treatment, respectively. Of the patients, 460 (11.4%) reported having had prior contact with TB. Among these, 127 (28%) were positive for the TST test (≥5 mm). However, only one patient had TB.
TST
TST tests were administered to a total of 4111 patients without a history of TB at entry. Of these, 1157 (28.1%) tested positive. The mean (SD) diameter of the TST induration was 4.8 (9.7) mm and the median (IQR) diameter was 0 (0–4) mm. In the TST-positive and TST-negative groups, the mean (SD) CD4 was 405.3 (221.3) cells/μL and 267.2 (209) cells/μL (p=0.000), respectively. Positive TST results were highly associated with a CD4 cells count of more than 200 cells/μL (p=0.000). Of the patients who had applied TST on their arms 93 (2.2%) did not return at the appropriate time to read their results. A total of 873 patients (21.2%) had more than one TST test, which was done the following year.
Among these patients, 176 (20.2%) had TST converted. Of the patients, 37 (22.6%) had TST converted in the first year after their first negative TST test and 85 (51.8%) were tested positive in the second year. In the third year, 34 (20.7%) patients were TST positive whereas 8 (4.9%) patients became positive in their fourth year. We could not find any demographic factor that was significantly associated with the conversion. Of these converted patients 63.6% were on ART with a mean (SD) CD4 of 206.9 (16) cells/μL compared to 207.7 (8) cells/μL in the group that did not convert (p=0.264).
The results of the logistic regression model associated with positive TST and TST conversion are shown in Tables 1 and 2.
Baseline Factors Associated with Positive Tuberculin Skin Test Result
p<0.05. Variables in bold were statistically significant, and adjusted for each other in the multivariate analysis. Other variables were adjusted for variables in bold.
TST, tuberculin skin test; OR, odds ratio; ARV, antiretroviral.
Baseline Factors Associated with Tuberculin Skin Test Conversion
p<0.05. Variables in bold were statistically significant, and adjusted for each other in the multivariate analysis. Other variables were adjusted for variables in bold.
INH Preventive treatment of TB infection
INH prophylaxis of latent TB was administered to 799 patients (81.4% of all TST-positive patients). Of IPT patients 551 (69%) had completed 9 months of INH therapy and 633 (79.2%) IPT patients had completed 6 months of INH therapy. A baseline CD4 of >200 cells/μL was significantly associated with higher rates for completing the INH therapy (p=0.000).
Incidence of TB
Only 348 (8.5%) participants who had TST tests could be reached to provide information on active TB. According to the available information, 75 participants developed TB during a total follow-up period of 6,232.02 person-years, which corresponded to an overall incidence of 1.2 patients per 100 person-years. The mean (SD) duration of follow-up was 33.3 (13.5) months. Of the patients who completed 6 months of INH, none developed active TB, compared to two patients (2%) without IPT or an incomplete course of IPT who developed TB (p=0.084). A total of 34 (1.8%) negative TST patients developed TB during the follow-up period. In a multivariate Cox proportional hazard model, the hazard of TB was positively correlated with TST-positive patients with low CD4 (p=0.004) on ART (p=0.030).
Safety
At baseline, 539 (12.4%) participants had a mean (SD) SGPT of 28.7 (20.3) IU/L and 476 (88.3%) had normal SGPT prior to starting IPT. SGPT at 3 months was obtained in 408 subjects. Of these, 1.2% developed SGPT ≥grade 3 at 3 months. A similar trend was also observed at 6 months; 1.01% had SGPT ≥grade 3.
INH was discontinued for all patients with SGPT grade >3 and SGPT returned to normal thereafter. A total of 52 (92.9%) patients with grade 1 SGPT level at baseline started INH and only 35 (67.3%) completed IPT. As for those with grade 2 SGPT at baseline, four (57.1%) started and completed 6 months of INH. Nobody from the 6 months IPT developed TB. When we compared the younger and older groups, with a cut-off of 50 years for the younger group, we found that both groups had similar levels of SGPT (p=0.244). Surprisingly, none of the older patients had any high, abnormal levels of SGPT.
In terms of SGPT result done at approximately 3 months and 6 months after INH intake, the results for both depended on the abnormality of the baseline SGPT. The results are shown in Tables 3 and 4. Elevation of SGPT grading was found to be significantly associated only with baseline CD4< 200 cells/μL [18 (34.6%) vs. 72 (20.5%) p=0.022]. Interestingly, completion of INH, along with all available demographic factors, was not found to be significantly related to increases in SGPT grading.
Serum Alanine Aminotransferase at Baseline and at 3 Months and 6 Months After Starting Isoniazid
SGPT, alanine aminotransferase; INH, isoniazid; IPT, isoniazid preventive therapy; IU/L, international units per liter.
The Affect of Baseline Serum Alanine Aminotransferase on Subsequent Alanine Aminotransferase Levels After Isoniazid for 3 and 6 Months
Discussion
This study involved a large, prospective cohort of TST and IPT patients in the HAART era in Thailand, where there is a high burden of HIV and TB. The estimated annual risk of developing active TB was 12.9 per 100 person-years in HIV-negative compared to 35–162 per 100 person-years in HIV-positive individuals. 24,25 People with HIV and latent TB have ≥30% lifetime risk of developing active TB. Therefore, it is important to identify HIV-1-infected patients with latent TB infection and provide preventive chemotherapy treatment according to accepted treatment guidelines. 12,26
Reducing the incidence of TB among people with HIV is crucial because TB complicates the management of ART-treated patients such as pill burden, drug–drug interaction, overlapping side effects, and immune recovery syndrome. About 28% of our population was diagnosed with latent TBI. These patients are at risk of developing active TB. Interestingly, 20% of these patients were TST negative when they entered the study but converted a year later. Seventy-five participants (1.8%) developed TB during a total follow-up of 6232.02 person-years, which corresponded to an overall incidence of 1.2 patients per 100 person-years. Surprisingly, none of the TS- positive patients who received 6 months of IPT developed active TB compared to those without IPT or an incomplete course of IPT (p=0.084). On the other hand, 1.8% of TST-negative patients developed active TB during the follow-up period.
Furthermore, 12 % out of 539 patients had an abnormal SGPT prior to IPT, but only 1% of 539 patients developed asymptomatic SGPT >grade 3 at 3 and 6 months. Age was not associated with an abnormal SGPT because both young and old patients (>50 years old) had similar SGPT levels. Our study showed that IPT-associated hepatotoxicity was rare when compared to other non-HIV studies. 27,28 However, our findings were based on a small number of patients with hepatotoxicity (N=6).
Despite this, our study had some limitations. One of the limitations was the self-reported questionnaires, which did not cover all potential risk factors such as alcohol intake, adherence of INH intake, etc. Another limitation of the study was the lack of CD4 and HIV RNA information at the time of active TB. Other limitations included time of analysis and lack of INH resistance data for those who developed active TB during the follow-up period. When we had analyzed the data, the study was ongoing. However, if we waited to analyze the data after the study was completed, then it is possible that the completion rate of IPT might be higher compared to the current values.
Regardless of its limitations, our results supported data showing INH's efficacy. 13,15 –17,21 Moreover, our study showed that TST and IPT are feasible in a VCT center in Thailand. Of our patients 81% with latent TBI who initiated INH chemoprophylaxis therapy; 69% and 79% of these patients completed 9 months and 6 months of IPT, respectively. The percentage of INH completion at 9 months in this study was comparable to the 62% and 59% completion rate from Kwara et al. 27 and Hess et al., 29 respectively. In addition, the 6-month completion rate from our study was comparable to other studies, 30,31 but was higher compared to the study conducted by Kwara et al. 27 We also found that patients with CD4> 200 cells/μL had better adherence to IPT. Intensive nurse care management and integration of HIV services along with TST and IPT may explain why we had a high success rate of people completing their IPT at 6 and 9 months at our center.
Aside from that, our study demonstrated that preventive treatment of latent TB was highly successful in our setting. Several studies 21,32,33 pointed out that the use of TST and IPT for patients with positive TST continues to be an efficacious strategy to reduce TB-associated morbidity, even in the era of HAART.
Based on our data, none of the TST-positive patients who received 6 months of IPT developed active TB. Aside from that, based on the three I's strategy of WHO's recommendations (IPT indicated, intensified patients finding for active TB, and TB infection control), IPT is highly recommended in patients who are TST positive. 34 The three I's is important in controlling TB infection in HIV-infected patients, healthcare workers, and the community. Therefore, TST and IPT should be implemented, particularly in high endemic areas of TB and in patients at risk of developing TB, i.e., HIV-infected patients with CD4< 200 cells/μL and positive TST. 34 However, active TB should be extensively excluded prior to IPT to prevent the development of INH-resistant strains. Of note, adherence to preventive treatment is very important to prevent further INH resistance.
In conclusion, these data showed that the use of INH was safe and well tolerated. INH prophylaxis in TST-positive patients in this setting is possible and deserves to be used more widely for the prevention and control of TB. However, the long-term advantage of INH prophylaxis in terms of TB prevention, especially in HIV-1-infected patients on HAART, requires further study.
Footnotes
Acknowledgments
This study was partly sponsored b the Global Fund. Mana Khongphatthanayothin and Anchalee Avihingsanon contributed equally to this work.
Author Disclosure Statement
No competing financial interests exist.