
Abstract
Combination antiretroviral therapy (cART) can cause potentially stigmatizing facial lipoatrophy. Encouraging preliminary results have been reported with 2.5% polyacrylamide hydrogel for facial reconstruction. The aim of this multicenter, open-label noncomparative pilot study was to evaluate the efficacy and safety of intradermal facial injections of polyacrylamide hydrogel in HIV-infected patients with severe facial lipoatrophy. The patients received between two and six injections every 4 weeks, according to the aesthetic results. Clinical efficacy was evaluated by means of facial ultrasonography and photography at baseline and months 6, 12, and 24. Adverse events, patient satisfaction, and quality of life were also assessed. One hundred and eleven patients were enrolled and received at least one injection. Mean cheek skin thickness was 9.7 mm [95% CI: 9.1 to 10.2] at baseline. It rose by an average of 4.4 mm [95% CI: 3.9 to 4.9; p<0.001] at month 12 and a further 0.87 mm [95% CI: 0.52 to 1.23; p<0.001] at month 24. The Overall Treatment Satisfaction scale showed an improvement in more than 88% of patients at all visits, based on the appreciations of the patients, their close relatives and physicians, and on independent assessment of facial photographs. Quality of life improved significantly over time, as shown by the lipodystrophy-specific ABCD scale. No severe adverse effects related to the polyacrylamide hydrogel were noted. Polyacrylamide hydrogel injections were well tolerated and significantly improved the aesthetic aspect and quality of life of HIV-infected patients with facial lipoatrophy.
Introduction
Since its introduction in 1996, combination antiretroviral therapy (cART) has drastically reduced HIV-associated morbidity and mortality in rich countries. 1 –4 However, cART can have metabolic adverse effects such as lipodystrophy, hyperlipidemia, and insulin resistance. 5,6 Lipoatrophy of facial subcutaneous tissue is potentially stigmatizing and can undermine adherence to antiretroviral treatment. 7 –9 Although newer nonthymidine nucleoside reverse transcriptase inhibitors (NRTIs) are associated with a lower incidence of lipodystrophy, 10,11 preexisting lipoatrophy is extremely slow to resolve after switching to nonthymidine NRTIs. 12 –18
Polylactic acid implants (PLA) have been approved for the correction of facial lipoatrophy. 19 –24 They act by enhancing collagen synthesis in the treated dermal area but can cause subcutaneous micronodules and indurations; in addition, treatment must be repeated in the medium term in a large proportion of patients. 20,22,25
Polyacrylamide gel contains 2.5% cross-linked polyacrylamide in 97.5% pyrogen-free water. After subcutaneous injection, the inert, relatively viscous gel encapsulates, thereby increasing subcutaneous volume. Several observational studies suggest that 2.5% polyacrylamide hydrogel is safe and effective for correcting facial lipoatrophy in HIV-infected patients. 25 –27 The aim of this study was to confirm and extend these reports.
Materials and Methods
Study design
The LIPOPHILL study was an open-label, prospective multicenter trial designed to evaluate the efficacy and safety of 2.5% polyacrylamide hydrogel in HIV-infected patients with severe facial lipoatrophy. The patients received between two and six injections of 2.5% polyacrylamide hydrogel (Eutrophill, Procytech, Martillac, France) every 2 to 4 weeks until month 6, according to the aesthetic results. With the patient in a seated position, the sunken areas are carefully drawn on the face using level lines. Injections were performed subcutaneously in the more sunken areas of the middle third of the face, which usually extend from the inner part of the suborbicularis area to the medial cheek, laterally to the nasolabial fold, which is not naturally affected by the fat atrophy. Injection is performed continuously and evenly from one side to the other in the deepest part of the sunken area at the subcutaneous level. At each cycle, a dose of 1–3 ml was injected on each side. Follow-up lasted 24 months after inclusion. The study conformed to the International Conference on Harmonization guidelines for Good Clinical Practice and the Declaration of Helsinki.
Study population
Patients were recruited between November 2005 and March 2007 in two French clinical centers, located in Paris (Hôpital Européen Georges Pompidou) and Lyon (Hôpital Edouard Herriot). HIV-infected adults were eligible for inclusion if they met the following criteria: HIV-infected men and nonpregnant women aged 18 years or more, with ART-related severe facial lipoatrophy, taking the same cART regimen for at least 3 months prior to inclusion, and CD4 cell count >100/mm3. Patients with ongoing opportunistic infections, any facial skin disease (including Kaposi's sarcoma), or previous treatment with facial implants were not eligible. Baseline peripheral fat loss or abdominal fat accumulation was evaluated by the investigator by using a questionnaire.
All the patients gave their written informed consent prior to enrollment, and the protocol was approved by the ethical review board of Hôpital Européen Georges Pompidou, Paris, France.
Assessment and monitoring
The endpoints included both objective and subjective measures assessed at week 0 (inclusion) and months 6, 12, and 24.
The primary endpoint was to evaluate the change in the thickness of Bichat's fat pad region, as determined by facial ultrasonography performed by the same radiologist using the same digital multifrequency 7.5–13 MHz transducer. Total cheek skin thickness was measured at the mid-point of the line joining the middle of the orbit and the wing of the nose. The recorded value was the mean of four measurements on each cheek (=eight measures).
Secondary endpoints comprised the following: (1) the changes in Overall Treatment Satisfaction (OTS) score, as noted by the patient, close relatives, and physician, and ranging from −7 (worst) to +7 (best); (2) qualitative pre- and posttreatment comparisons by three independent reviewers based on standardized photographs and the OTS scale; and (3) changes in quality of life, as evaluated with a self-administered questionnaire validated for HIV-infected patients with lipodystrophy (Adult AIDS Clinical Trials Group Assessment of Body Change and Distress; ABCD questionnaire). 26 The ABCD questionnaire comprises 28 items: items 1 to 6 are used to discriminate patients who report body changes, item 7 analyzes overall satisfaction with body appearance, and the remaining 21 items analyze quality of life related to lipodystrophy, divided into four dimensions: Dimension A (control and coping with the disease, and satisfaction with body appearance), Dimension B (psychosocial, social, and relational impact), Dimension C (fear of future), and Dimension D (relation with cART); (4) changes in anxiety and depression (HAD questionnaire); and (5) safety of the treatment. Safety was assessed at each visit, based on an interim medical history, a physical examination, and an interview focusing on adverse events. Specific adverse events were particularly assessed (e.g., local infection, local inflammation, local hematoma, subcutaneous nodules).
Sample size
Forty-five patients were required to detect a change of one-half a standard deviation in total cheek skin thickness with a power of 90% and a type 1 risk of 5%. The sample size was set at 100 patients in order to take account of dropouts and to permit multivariable and subgroup analyses.
Statistical analysis
The characteristics of the study population are reported for the modified intent-to-treat (mITT) population, which included all patients who received at least one injection of 2.5% polyacrylamide hydrogel.
Changes in total cheek skin thickness (month 12 versus inclusion and month 24 versus month 12) were assessed with a mixed model taking account of repeated measurements in each subject. Interindividual variability in cheek skin measurements at inclusion was considered by using a random intercept, and the correlation between repeated measurements was modeled with a spatial covariance structure taking account of the observed time between ultrasonography evaluations. The model included as fixed effects the natural logarithmic transformation of time since the first injection (logarithmic time trend), the participating center, the number of injections, and the total quantity injected in both cheeks since the beginning of the study, and all interactions of order 2 with time. The analysis was performed in three populations: the mITT population, the population of patients without major protocol deviations and no missing measurements at month 12 (change at month 12), and the population of patients with no major protocol deviations and no missing measurements at both month 12 and month 24 (change between months 12 and 24). In the mITT population, we imputed missing data based on the minimum relative change observed in patients with no missing data at the relevant time point; the model did not include the number of injections or the cumulative quantity injected in order to avoid a new imputation. Ninety-five percent confidence intervals (95% CI) and p values were adjusted for multiple comparisons by using Scheffé's method.
OTS scores, signs of lipodystrophy and the overall “satisfaction with body appearance” score in the ABCD questionnaire, scores for anxiety and depression, and the proportions of patients with high anxiety and depression scores (≥8) in the HAD questionnaire were analyzed with nonparametric tests, without replacement of missing data and without adjustment for multiple comparisons. The overall changes in scores and proportions over time were assessed with Friedman's test and Cochran's Q test (in subjects with no missing data); when the global test was significant, pairwise comparisons were made with the signed rank test or MacNemar's test. OTS scores were compared across the patients, close relatives, and physicians at each time point by using the Kruskall–Wallis test. The concordance of the OTS scores of the three external reviewers was evaluated by calculating Kendall's tau coefficient. The scores for the four dimensions of the ABCD questionnaire (items 8 to 28) were analyzed among patients evaluated at inclusion by using a mixed model including the dimension and the type of follow-up visit, and their interaction (fixed effects), a random intercept on subject, and a covariance structure taking account of the correlation among the dimension scores for a given patient. Pairwise comparisons with the scores at inclusion were adjusted with Dunnett's method.
p values below 0.05 were considered to denote statistical significance. SAS software (release 9.1; SAS Institute Inc., Cary, NC) was used for all analyses.
Results
Study population
One hundred and fifteen patients were enrolled in this trial. One hundred and eleven of these patients received at least one injection of 2.5% polyacrylamide hydrogel (mITT population), 101 patients were followed until month 6, 97 patients were followed until month 12, and 88 patients were followed until month 24 (Fig. 1). One major deviation occurred: a patient having previously received a facial implant was treated with 2.5% polyacrylamide hydrogel.
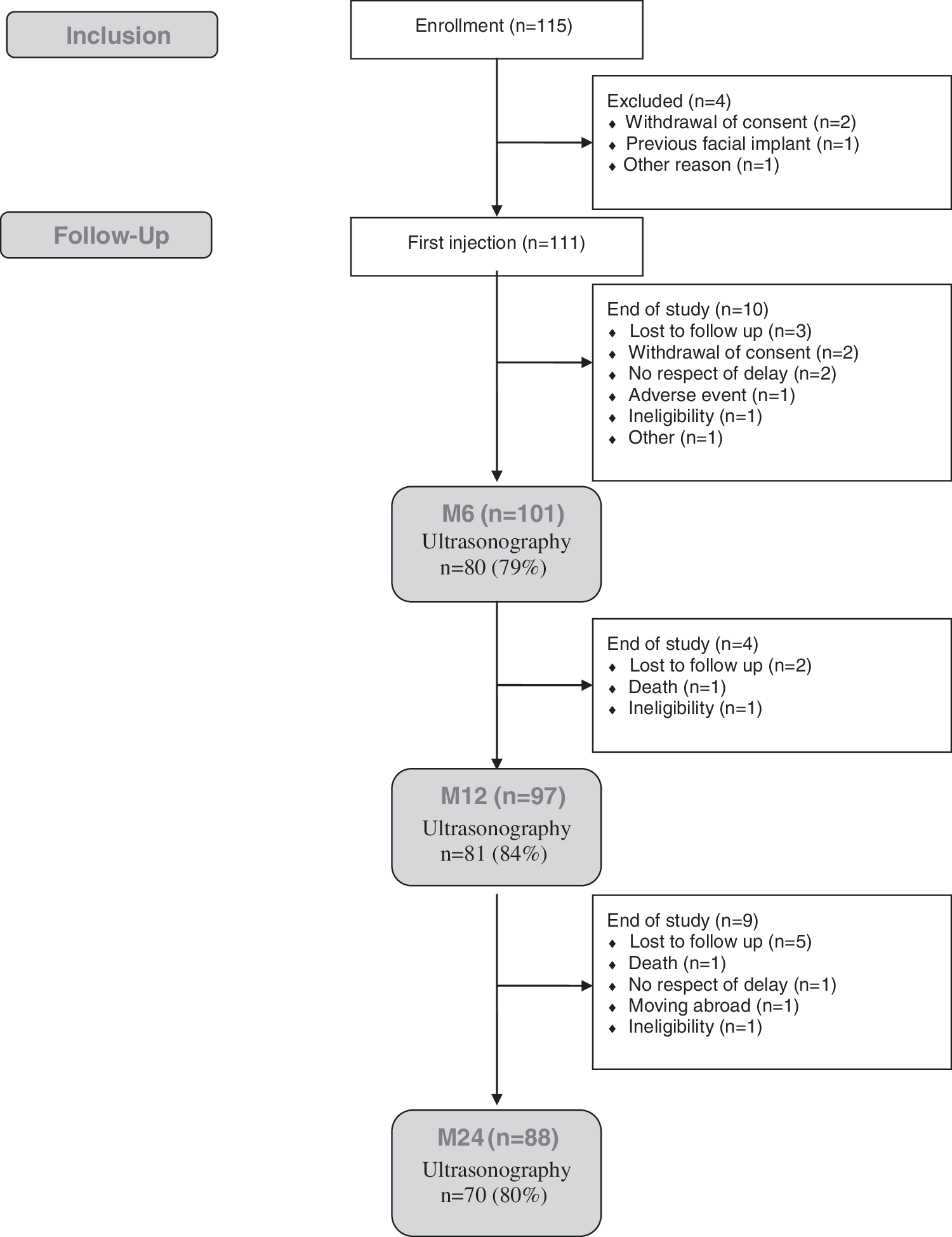
Flowchart.
Baseline characteristics of the 111 patients in the mITT population are shown in Table 1. The median age was 46 years. The median duration of antiretroviral treatment was 9 years, and 75% of the patients had been exposed to stavudine. The median cheek skin thickness was 9.8 mm.
Baseline Characteristics of the 111 Patients Who Received at Least One Injection of Polyacrylamide Hydrogel
Injections follow-up
The median number of injections was three (one to eight) and the median cumulative quantity of product injected was 17 ml (2 to 49 ml). Both these parameters differed significantly between the clinical centers: three injections (one to six) versus five (one to eight) (p<0.001) and 15 ml (2 to 36) versus 20 ml (2 to 49) (p=0.006). Among the 101 and 97 patients who were still participating in the study at months 6 and 12, 26 patients (26%) had at least one injection between month 6 and month 12, and 34 (35%) patients had at least one injection between month 12 and month 24.
Changes in cheek skin thickness
Changes in cheek skin thickness, as measured by ultrasonography, are shown in Table 2 and Supplementary Fig. S1 (Supplementary Data are available online at
Changes in Mean Cheek Skin Thickness
Derived from the mixed model with Scheffé's adjustment for multiple comparisons. Estimated mean cheek skin thickness was adjusted for the time since the first injection, the clinical center, the number of injections and the cumulative quantity injected into both cheeks, and all interactions of order 2 with time. In the mITT population, missing measurements were imputed by using the minimum relative change observed in patients with available values; mean cheek skin thickness was not adjusted for the number of injections or the quantity injected (see Materials and Methods for details).
One patient with a previous facial implant was subsequently excluded.
mITT, modified intent-to-treat.
All 111 patients in the mITT population had an ultrasonographic examination at inclusion. Excluding the patient with a previous facial implant, 80 patients had ultrasonography at month 12, and 61 patients at both month 12 and month 24.
Mean cheek skin thickness was 9.67 mm [95% CI: 9.10 to 10.24] at inclusion and 14.04 mm [95% CI: 13.58 to 14.50] at month 12 in the 80 patients evaluated at both time points, representing a statistically significant average increase of 4.37 mm [95% CI: 3.89 to 4.85; p<0.001]. Mean cheek skin thickness was 14.02 mm [95% CI: 13.49 to 14.54] at month 12 and 14.89 mm [95% CI: 14.29 to 15.49] at month 24 in the 61 patients with both evaluations, representing a statistically significant average increase of 0.87 mm [95% CI: 0.52 to 1.23; p<0.001] between month 12 and month 24. Similar results were obtained in the mITT population after imputation of missing data (Table 2).
Overall treatment satisfaction and analysis of facial photographs
Completion rates were 67% (68/101), 80% (78/97), and 86% (76/88) at months 6, 12, and 24, respectively. The median OTS score at months 12 and 24 was 5 according to the patients and close relatives and 6 according to the physicians (Fig. 2a). None of the patients, close relatives, or physicians considered that the facial aspect had worsened at month 6, 12, or 24, with the exception of one patient who gave himself a score of −5 and whose physician gave him a score of −6. However, a significant improvement of facial photographs was noted by the three external reviewers associated with an increase in cheek skin thickness measured at month 24. All the observers noted an improvement in more than 90% of patients at all time points. No significant change in the OTS scores was noted between month 6, month 12, and month 24 by the patients (p=0.44), close relatives (p=0.40), or physicians (p=0.22). The physicians gave higher OTS scores than the patients and close relatives.
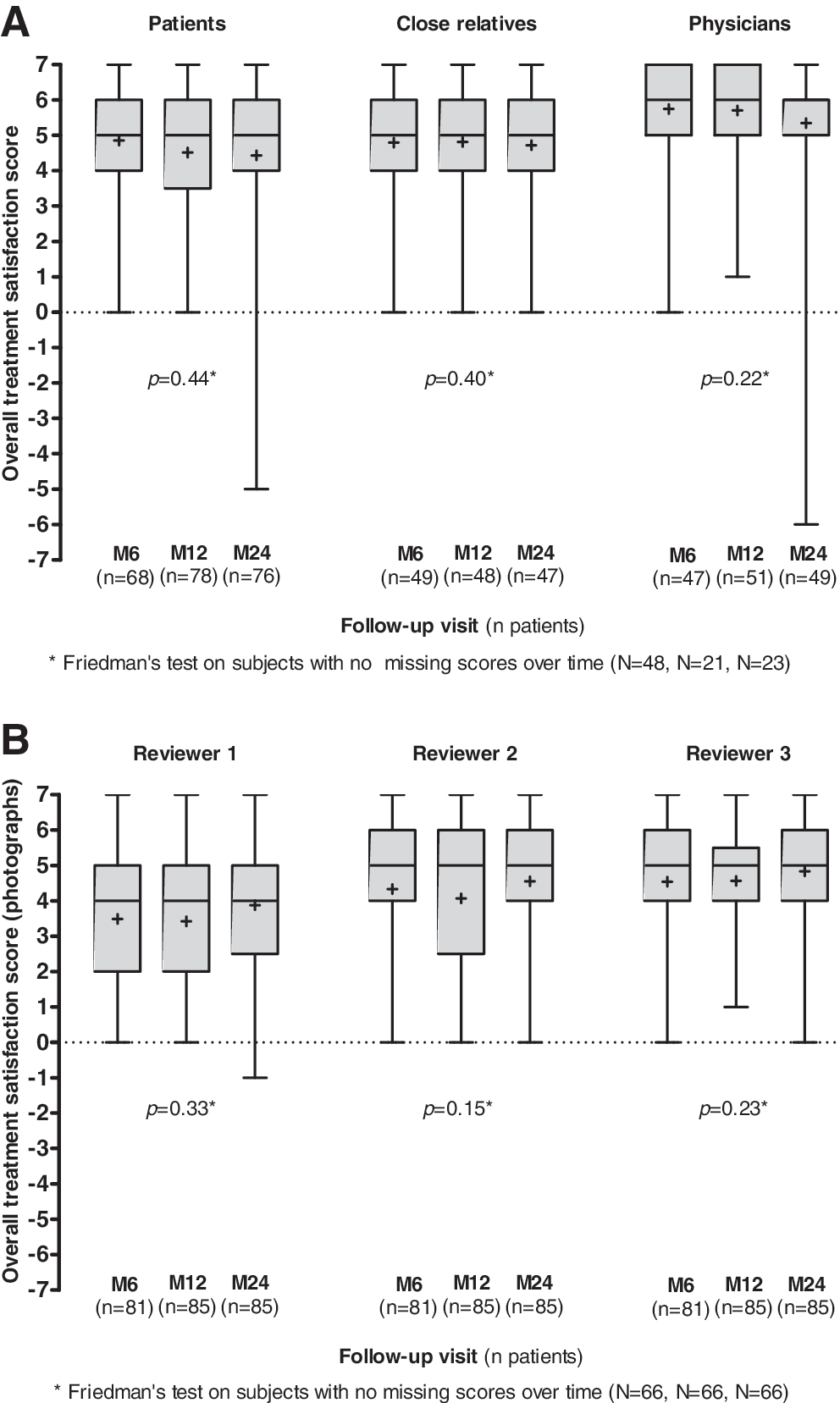
Overall treatment satisfaction.
A total of 251 facial photographs were analyzed by the three external reviewers (81 at month 6, 85 at month 12, and 85 at month 24) (Fig. 2b). The median OTS score was 4 at months 12 and 24 according to first reviewer, and 5 according to the other two reviewers (Kendall's tau=0.70, 0.66, and 0.69 at months 6, 12, and 24, respectively). None of the reviewers considered that the facial aspect had worsened at month 6, 12, or 24, except for one reviewer who scored one patient −1 at month 24. All the reviewers noted an improvement in more than 88% of patients at all the time points.
ABCD questionnaire
Completion rates were 91% (101/111), 66% (67/101), 81% (79/97), and 87% (77/88) at inclusion and months 6, 12, and 24, respectively. At inclusion the median scores for signs of lipodystrophy (items 1 to 6) and overall satisfaction (item 7) were both 3. There was a significant increase in satisfaction at months 6, 12, and 24 compared to inclusion (p<0.001). The quality-of-life (QoL) scores for the four dimensions differed at inclusion, but the changes over time were similar (interaction term p=0.85). The mean global QoL score was 64.9 [95% CI: 61.5 to 68.4] at baseline, and rose by 3.9 [95% CI: 0.6 to 7.3, p=0.015], 3.0 [–0.1 to 6.2, p=0.060], and 3.8 [0.6 to 7.0, p=0.016] points, respectively, at months 6, 12, and 24 (Fig. 3).
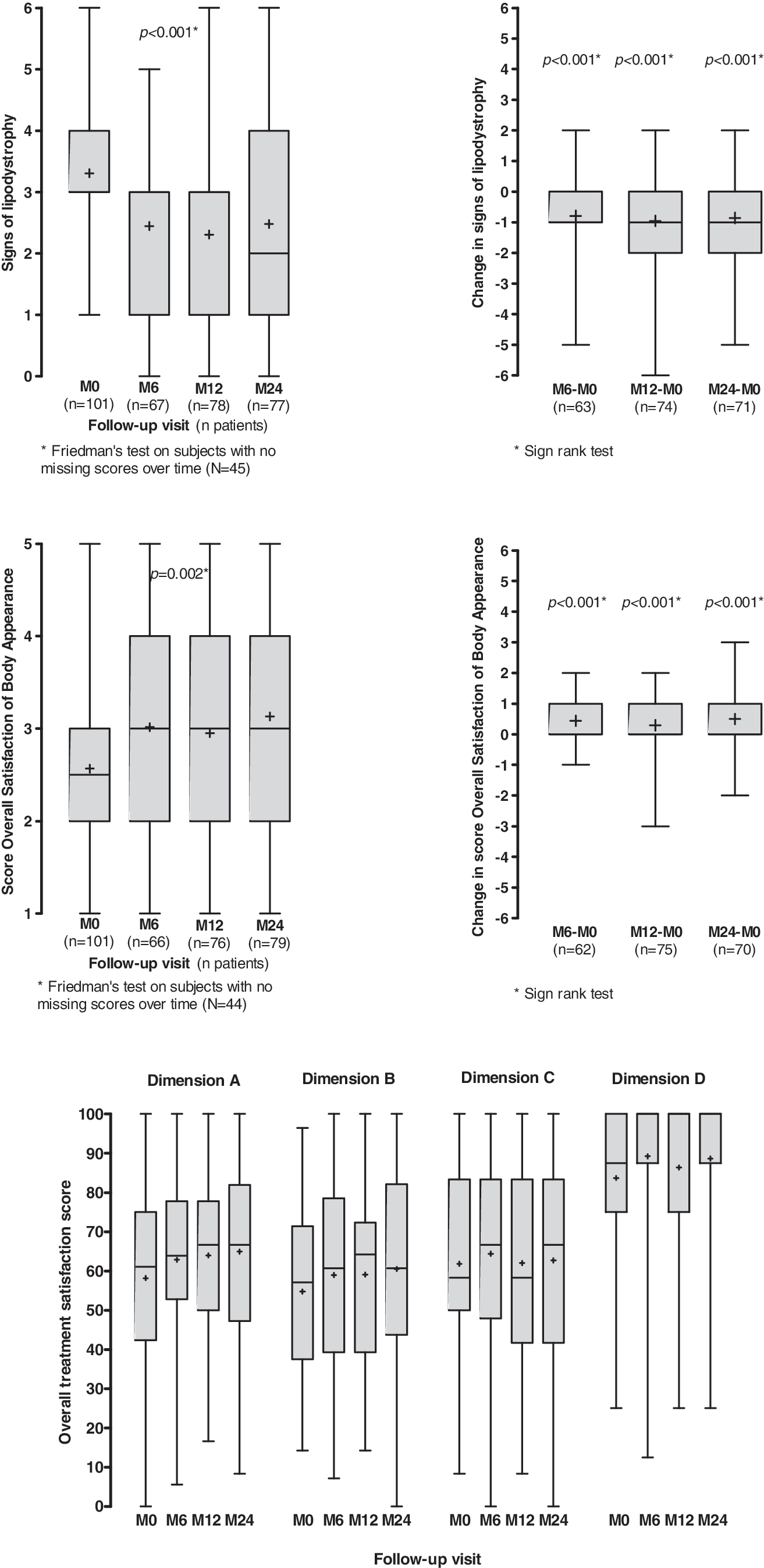
ABCD questionnaire. Box plots present mean (cross), median (line), 25th and 75th percentiles (box), minimum and maximum values (whiskers).
HAD questionnaire
Completion rates were 91% (101/111), 67% (68/101), 78% (76/97), and 87% (77/88) at inclusion and months 6, 12, and 24, respectively. The median anxiety and depression scores at inclusion were 7 (range: 0 to 17) and 4 (range: 0 to 15), respectively; 48% of patients (48/101) had high anxiety scores and 25% of patients (25/101) had high depression scores. Neither score improved over time (p=0.12 and p=0.08), and the proportions of patients with high anxiety scores and high depression scores were similar at all the time points (p=0.37 and p=0.49) (Supplementary Fig. S2).
Adverse events
Twelve serious adverse events occurred in nine patients, comprising epidermoid carcinoma of the skin, hepatocellular carcinoma, pulmonary tuberculosis, pneumonia, coronary artery disease (three cases), bone fracture related to osteomalacia, suicide, aortic valve replacement, and odontogenic maxillary sinusitis (two cases). None of these events was considered to be linked to the polyacrylamide hydrogel injections. No infections occurred at the injection sites. Subcutaneous nodules related to hydrogel injections were observed in three patients and transient local inflammatory reactions were observed in three patients. The injections were generally well tolerated and never had to be interrupted because of adverse effects.
Discussion
This open-label, multicenter, noncomparative trial suggests that 2.5% polyacrylamide hydrogel significantly improves the looks and quality of life of HIV-infected patients with facial lipoatrophy at months 6, 12, and 24 of follow-up. Sonographically measured facial subcutaneous thickness rose significantly, from 9.78 mm at baseline to 14.02 mm at month 6, stabilizing thereafter (14.26 mm at month 12 and 14.50 mm at month 24). These changes were clinically relevant, as shown by the Overall Treatment Satisfaction scores and the ABCD questionnaire. Indeed, at months 6, 12, and 24, the median OTS scores were 5 (“a good deal better”) according to the patients and close relatives and 6 (a great deal better) according to the physicians. The OTS scores were within the same values according to the analysis of standardized photographs by three independent reviewers. In addition, the ABCD autoquestionnaire showed a significant decrease in signs of lipodystrophy and a significant increase in overall satisfaction with body appearance at months 6, 12, and 24. In contrast, the correction of facial lipoatrophy did not improve the anxiety and depression scores. Median HAD questionnaire scores remained low during the 24 months of follow-up. However, the HAD questionnaire measures general anxiety and depression and might not capture specific effects of stigma and lipodystrophy.
These effects were not due to discontinuation of thymidine analogues, 13,28,29 as none of the patients was switched from thymidine analogues during the study period or less than 1 year prior to inclusion.
No serious adverse events related to the polyacrylamide hydrogel injections occurred, including injection-site infections. A mild and transient local inflammatory reaction was observed in three patients, and small subcutaneous nodules occurred in three patients.
PLA implants approved in Europe and the United States for the correction of HIV-related facial lipoatrophy are associated with the occurrence of palpable subcutaneous nodules in between 10% and 44% of patients. 19,20,22,24 The incidence of subcutaneous nodules seems to be lower with polyacrylamide hydrogel. 26 Polyacrylamide hydrogel is a stable, nonresorbable aqueous gel containing no microparticles or microspheres. The filling effect is exclusively due to the volume of the gel itself, unlike other tissue fillers. PLA implants, for example, act by increasing collagen synthesis.
Previous reports suggest that the effect of polyacrylamide hydrogel is more durable than that of PLA implants. 22,25 Lafaurie et al. reported a 45% probability of PLA reinjection 15 months after initial treatment. 22 In a comparative trial, a new round of injections at week 48 was necessary in respectively 84% and 8% of patients treated with PLA implants and polyacrylamide hydrogel. 25 In our trial, respectively 26% and 35% of patients required at least one new injection at months 6–12 and 12–24.
In conclusion, the efficacy, safety, and simple administration of polyacrylamide hydrogel make this filling material an attractive option for correcting facial lipoatrophy in HIV-infected patients. Randomized trials are now needed to compare the short-term and long-term efficacy and safety of PLA implants and polyacrylamide hydrogel.
Footnotes
Acknowledgments
This work was sponsored by Assistance Publique Hôpitaux de Paris, Paris, France. It has been presented in part at the 5th IAS Conference on HIV Pathogenesis, Treatment, and Prevention, Cape Town, South Africa, July 2009. We thank PROCYTEC for helpful discussions and financial/logistic support, as well as the patients who participated in the LIPOPHILL study.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.