
Abstract
The prevalence of susceptibility to etravirine was investigated among clinical samples submitted for routine clinical testing in the United States using two separate weighted genotypic scoring systems. The presence of etravirine mutations and susceptibility to etravirine by phenotype of clinical samples from HIV-1-infected patients, submitted to Monogram Biosciences for routine resistance testing between June 2008 and June 2009, were analyzed. Susceptibility by genotype was determined using the Monogram and Tibotec etravirine-weighted genotypic scoring systems, with scores of ≤3 and ≤2, respectively, indicating full susceptibility. Susceptibility by phenotype was determined using the PhenoSense HIV assay, with lower and higher clinical cut-offs of 2.9 and 10, respectively. The frequency of individual etravirine mutations and the impact of the K103N mutation on susceptibility to etravirine by genotype were also determined. Among the 5482 samples with ≥1 defined nonnucleoside reverse transcriptase inhibitor (NNRTI) mutations associated with resistance, 67% were classed as susceptible to etravirine by genotype by both scoring systems. Susceptibility to etravirine by phenotype was higher (76%). The proportion of first-generation NNRTI-resistant samples with (n=3598) and without (n=1884) K103N with susceptibility to etravirine by genotype was 77% and 49%, respectively. Among samples susceptible to first-generation NNRTIs (n=9458), >99% of samples were susceptible to etravirine by phenotype (FC <2.9); the remaining samples had FC ≥2.9–10. In summary, among samples submitted for routine clinical testing in the United States, a high proportion of samples with first-generation NNRTI resistance was susceptible to etravirine by genotype and phenotype. A higher proportion of NNRTI-resistant samples with K103N than without was susceptible to etravirine.
T
Several etravirine-weighted genotypic scoring systems have been developed, including the Monogram Biosciences genotypic scoring system and the Stanford University genotypic scoring system. 3 –5 A weighted genotypic scoring algorithm for etravirine has also been developed by Tibotec. 6 These scoring algorithms aid interpretation of resistance test results, and therefore can help guide treatment decisions. Each of the systems uses a score calculated from a list of mutations, each with its own weight factor, associated with reduced susceptibility and/or response to etravirine. According to the Tibotec etravirine-weighted score, a cumulative value of two or less indicates susceptibility to etravirine and, in the DUET trials, 77% of etravirine-treated patients with this score achieved plasma viral load <50 HIV-1 RNA copies/ml at week 48. 1
The objective of the current analysis was to examine the susceptibility to etravirine in routine clinical practice, using a U.S.-based commercial database. As such, the prevalence of susceptibility to etravirine by genotype was investigated in clinical samples referred for routine resistance testing over a 1-year period using both Monogram Biosciences' and Tibotec's etravirine-weighted genotypic scoring systems. The susceptibility of the samples to etravirine was also evaluated by phenotype, and by subtype [B versus non-B; subtypes included in the non-B set (with at least 15 instances) were A, A1, AE, AG, C, D, G, and Complex]. Further, the susceptibility of HIV clinical isolates carrying individual mutations (such as the K103N mutation) to etravirine was also evaluated.
Clinical samples from HIV-1-infected patients submitted to Monogram Biosciences (San Francisco, CA) for routine viral resistance testing from June 2008 to June 2009 were analyzed.
Genotypic testing was performed using the Phenosense/GT HIV assay (Monogram Biosciences, San Francisco, CA). Based on previous work, samples were defined as NNRTI resistant if they carried at least one of the following known NNRTI mutations: A98G, L100I, K101E, K101P, K103N, K103S, V106A, V106M, Y181x, Y188x, G190x, P225x, F227x, M230L, and P236L, where x represents any amino acid substitution. 4
Two different systems were used to define susceptibility to etravirine by genotype (the Monogram and Tibotec scoring systems). At the time of the analysis, the weighted score developed by Monogram incorporated 30 NNRTI mutations, each assigned a relative weight according to its impact on phenotypic susceptibility. For this system, a genotypic score ≤3 denotes full susceptibility. 3 The full list of 30 mutations (and their respective scores) is as follows: V90I (1), L100I (4), K101E (2), K101H (1), K101P (4), V106A (2), V106M (1), E138A (3), E138G (3), E138K (2), E138Q (1), V179D (1), V179E (3), V179F (1), V179L (2), V179M (1), Y181C (4), Y181F (1), Y181I (4), Y181V (4), Y188L (2), V189I (1), G190E (1), G190Q (3), G190T (1), H221Y (1), P225H (1), M230L (3), K238N (3), and K238T (1).
At the same time, the weighted score developed by Tibotec consisted of 17 etravirine resistance-associated mutations (RAMs). For this system, a genotypic score ≤2 denotes full susceptibility. 6 The full list of 17 RAMs (and their respective scores) is as follows: V90I (1), A98G (1), L100I (2.5), K101E (1), K101H (1), K101P (2.5), V106I (1.5), E138A (1.5), V179D (1), V179F (1.5), V179T (1), Y181C (2.5), Y181I (3), Y181V (3), G190A (1), G190S (1.5), and M230L (2.5). In addition, the impact of the K103N mutation on genotypic susceptibility to etravirine was investigated.
It should be noted that the individual weight factors were derived using different statistical approaches and as such, differences in the absolute value of the weight factors, as well the clinical significance of the total score, are not completely unexpected.
Susceptibility to etravirine by phenotype was determined using the PhenoSense HIV assay (Monogram Biosciences, San Francisco, CA). Lower and upper clinical cut-off values of 2.9 and 10, respectively, were used to indicate the degree of etravirine susceptibility. The Monogram lower and upper clinical cut-offs were calculated using PhenoSense data derived from a subset of etravirine recipients in the DUET sample set and exploring these data in relation to virologic response. 7
A total of 14,940 routine clinical samples were submitted to Monogram during the stated time period (June 2008 to June 2009) and were included in the analysis. NNRTI resistance was identified in a total of 5482 samples (36.7%), as indicated by the presence of at least one mutation from the list of NNRTI mutations described above. Most of the individual etravirine RAMs identified in the Monogram or Tibotec weighted scores occurred at a frequency of less than 5% in the 14,940 submitted samples, including E138K, which was observed in 0.6% of samples. Three etravirine RAMs occurred at a frequency greater than 5%: V90I (detected in 952 samples, 6.4%), Y181C (981 samples, 6.6%), and G190A (761 samples, 5.1%). V106I occurred at a frequency of 4% and P225H at 3.8%; all other RAMs occurred at 3% or less. Of the most frequently occurring individual etravirine RAMs, only Y181C has a substantial impact on weighted score, with a weight of 4 and 2.5 in the Monogram and Tibotec scoring systems, respectively.
In samples displaying NNRTI resistance (n=5482), 76.4% were classified as susceptible to etravirine by phenotype [fold-change in 50% effective concentration (FC) <2.9 according to the Monogram lower clinical cut-off], with a median FC of 0.9; 10.7% of samples had FC ≥10. In addition, among NNRTI-susceptible samples (n=9458), 99.5% had etravirine FC <2.9 (median 0.8) and the remaining 0.5% had FC <10 (median 3.5; Table 1). A very low frequency (<0.4%) of other NNRTI mutations was observed in the 9458 samples that harbored none of the first-generation NNRTI RAMs. Of 49 samples (0.5%) with no NNRTI mutations (i.e., without any of the previously defined mutations), but with etravirine FC >2.9 (all were FC <10), other NNRTI mutations were observed in 48 of 49 samples. The most common mutation was E138A (including mixtures), occurring in 71.4% of samples; the E138K mutation occurred in 4.1% of these samples. In the remaining 9409 NNRTI-susceptible samples (with etravirine FC <2.9), there were 454 samples (4.8%) with mutations at position E138, most of them E138A (69%, including mixtures).
N/A, not applicable; NNRTI, nonnucleotide reverse transcriptase inhibitor. Defined NNRTI RAMs: A98G, L100I, K101E, K101P, K103N, K103S, V106A, V106M, Y181x, Y188x, G190x, P225x, F227x, M230L, and P236L, where x represents any amino acid substitution.
Figure 1 shows the proportion of samples by Monogram and Tibotec weighted score. Of the 5482 samples displaying NNRTI resistance, 67.2% and 67.5% were classified as susceptible to etravirine by genotype as determined using the Monogram (susceptible=weighted score ≤3) and Tibotec (susceptible=weighted score ≤2) weighted scores, respectively (Fig. 1). When samples with evidence of NNRTI resistance were analyzed by subtype (B versus non-B), the proportion of samples classed as genotypically resistant to etravirine was similar, regardless of subtype and weighted scoring system used. Among subtype B samples, 32.9% were classed as resistant according to the Monogram scoring system, compared with 32.6% according to the Tibotec scoring system. Furthermore, in non-B samples, 35.2% tested as resistant to etravirine by genotype according to the Monogram scoring system versus 31.0% with the etravirine-weighted scoring system.
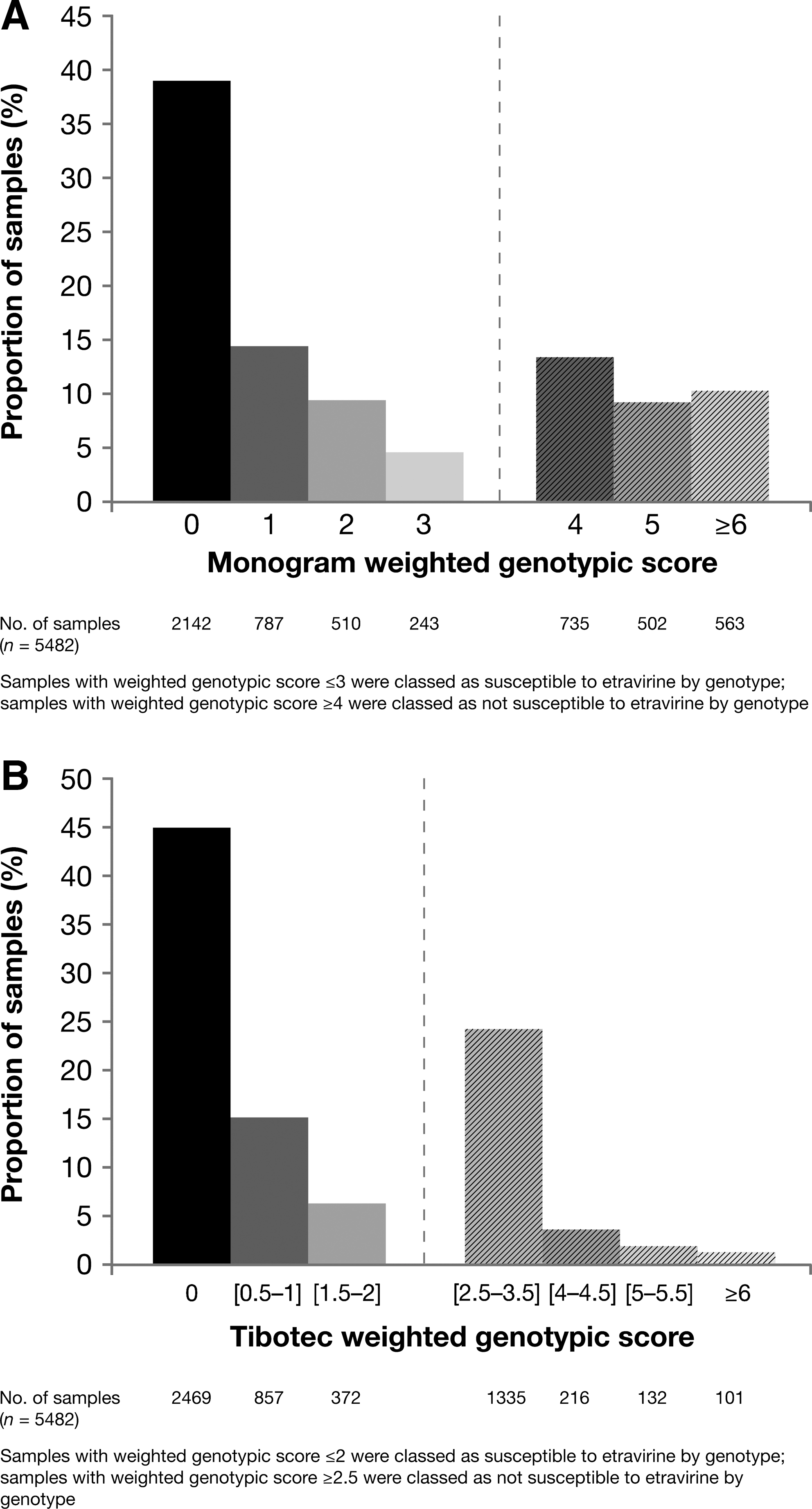
Proportion of samples with defined nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance showing genotypic susceptibility or reduced susceptibility to etravirine, as determined by
Among samples with NNRTI resistance, the K103N mutation was present in 3598 samples (65.6%). Among the samples with the K103N mutation, 76.9% were susceptible to etravirine by genotype applying the Monogram-weighted score (Fig. 2). In contrast, in the subset of NNRTI-resistant samples without the K103N mutation (n=1884), the proportion of samples susceptible to etravirine by genotype was 48.6%. Similar results were obtained using the Tibotec weighted score, with 77.5% and 48.2% of samples with and without the K103N mutation, respectively, showing susceptibility to etravirine by genotype. Among NNRTI-resistant samples, the median etravirine FC was 1.0, regardless of the presence of the K103N mutation.
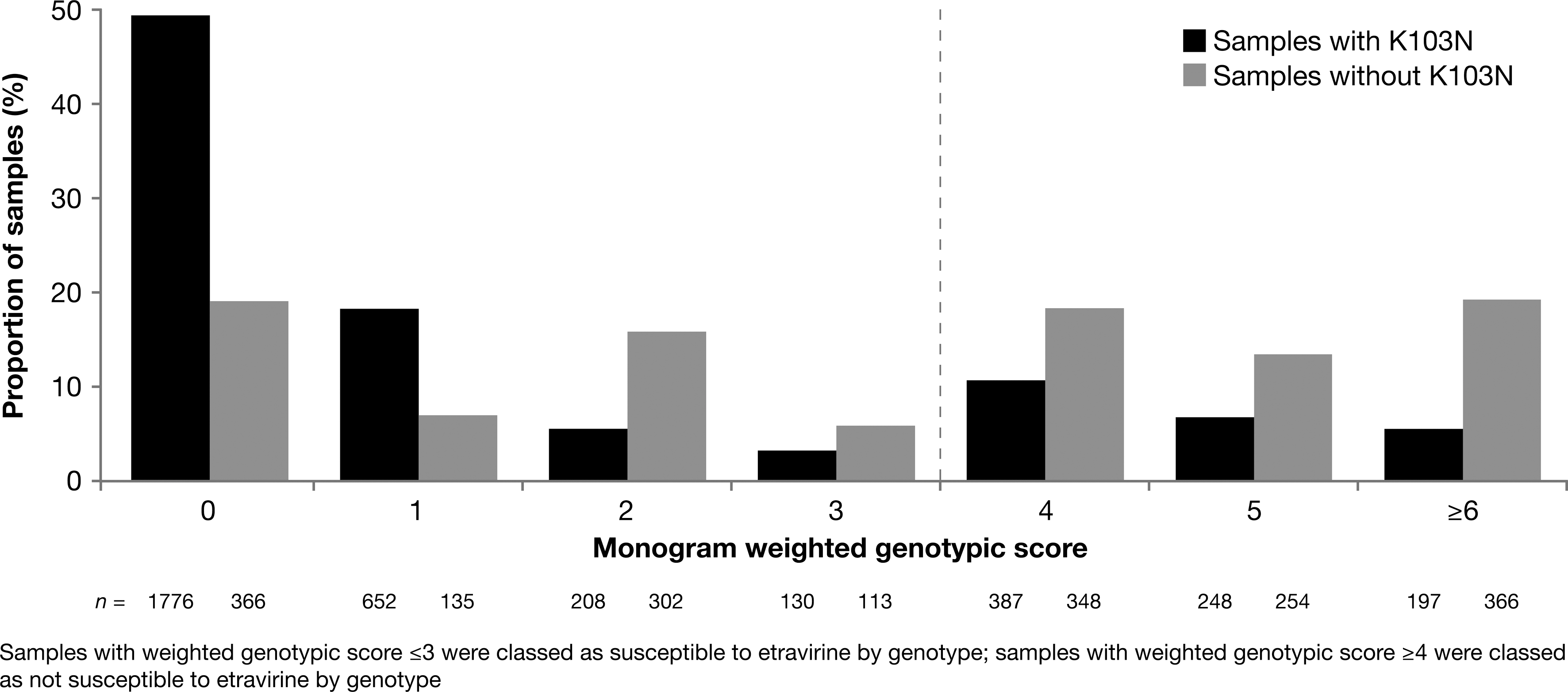
Influence of the K103N mutation on susceptibility to etravirine by genotype in samples with defined NNRTI resistance, as determined by Monogram weighted score.
Our results show that the majority of samples received for routine resistance testing were found to be susceptible to etravirine. Even in the presence of resistance to first-generation NNRTIs (37% of samples), approximately 67% and 76% of samples retained susceptibility to etravirine by genotype and phenotype, respectively. Similar proportions of samples susceptible to etravirine by genotype were obtained with the Monogram and Tibotec interpretation systems; importantly, however, this does not prove that the methods are necessarily equivalent since a head-to-head comparison between them (including clinical outcomes) was not conducted. Furthermore, our study did not account for the presence of minority variants, not readily detectable by population sequencing, which can contribute to etravirine resistance. It should also be noted that increased levels of resistance to NNRTIs over time are potentially likely to occur due to an increase in the use of second-generation NNRTIs, such as etravirine. In addition, the samples analyzed were exclusively sourced from the United States, somewhat limiting the scope of our study, as no comparable data in resource-limited settings are included. Indeed, available data in resource-limited settings indicate that susceptibility to etravirine in patients who have failed first-line NNRTI therapy may be reduced. 8
As expected, almost all samples (99.5%) with none of the defined first-generation NNRTI mutations were susceptible to etravirine by phenotype. Among samples with none of these NNRTI mutations, modest increases in etravirine FC above the lower clinical cut-off were associated primarily with the presence of the E138A mutation (including mixtures), and minimally with E138K, in the reverse transcriptase gene, which were not part of the list of NNRTI mutations used to define NNRTI resistance, but are considered etravirine RAMs. 9 However, the majority of samples with an E138A mutation were susceptible to etravirine by phenotype, suggesting that the effect of mutations at this position on etravirine susceptibility may be isolate specific.
Similar results have been reported from other groups investigating etravirine susceptibility. In a Spanish cohort of 3299 patients, a total of 4813 genotypes were derived, of which 1343 (28%) belonged to patients who had failed prior therapy with efavirenz or nevirapine. Eighty-one percent of samples with NNRTI resistance showed susceptibility to etravirine by genotype, based on the Tibotec weighted score. 10 Several additional studies have produced similar results, i.e., a high percentage of samples remains susceptible to etravirine, even after development of resistance to other NNRTIs. In a number of independent studies, at least 90% of clinical samples displaying resistance to efavirenz or nevirapine were found to retain susceptibility to etravirine. 11 –13 Similarly, over 75% of patients with documented resistance to efavirenz or nevirapine were predicted to retain susceptibility to etravirine. 14 –16
As previously reported, the K103N mutation, known to be associated with resistance to first-generation NNRTIs, has no effect on the virologic activity of etravirine. 6 Interestingly, in this analysis, the presence of the K103N mutation in NNRTI-resistant samples was associated with a greater frequency of etravirine susceptibility by genotype, relative to samples with other NNRTI mutations. This is not completely unexpected since it has been reported that the selection of K103N is associated with pathways of NNRTI resistance that include mutations with less effect on etravirine susceptibility. In this regard, Y181C, for example, was rarely seen in patients failing efavirenz, which is usually associated with the emergence of the K103N mutation. 17 The Y181C mutation is, however, the single and most prevalent mutation likely to have the highest impact on etravirine resistance in the study population analyzed, and is frequently found in patients failing nevirapine. 18 Another observation made in our study is that susceptibility to etravirine was more frequently reported by phenotype than genotype. This could be in part attributed to the effect of cooccurring nucleoside reverse transcriptase inhibitor (NRTI) mutations on NNRTI hypersusceptibility, not taken into account by the etravirine genotypic interpretation systems used in this study. 19 Indeed, in a separate study by the current author, hypersusceptibility to etravirine was observed among HIV-1 isolates carrying nucleoside-associated mutations, M184V or both. 20 Similarly, Napolitano and colleagues reported that the NRTI mutations K65R, L74V/I, and M184V were associated with hypersusceptibility to the NNRTIs efavirenz, nevirapine, delavirdine, and etravirine. 21
This analysis provides further evidence, using different interpretation systems, that most HIV isolates in the routine clinical practice setting are susceptible to etravirine, regardless of the presence of first-generation NNRTI resistance.
Footnotes
Acknowledgments
The authors acknowledge Eric Lefebvre, Benny Baeten, David Anderson, Frank Tomaka, and Steven Nijs for their important contributions to the manuscript. They also acknowledge Karen Pilgram (medical writer, Gardiner-Caldwell Communications, Macclesfield, UK) for providing medical writing support and collating author contributions. Funding for this service was provided by Tibotec Pharmaceuticals Ltd. Data were presented at the International AIDS Conference, Vienna, Austria, July 18–23, 2010. Abstract MOPDB105.
Author Disclosure Statement
G.P., J.V., L.T., and J.W. are full-time employees of Tibotec. M.H. is a full-time employee of Monogram Biosciences. E.C. was a full-time employee of Monogram Biosciences at the time the research was carried out.