
Abstract
Initiation of combined antiretroviral therapy (cART) is associated with bone loss, which may be more intense with regimens including tenofovir. The underlying mechanisms are not well understood. Cross-sectional data have linked tenofovir with higher parathyroid hormone (PTH) concentrations in patients with vitamin D deficiency. We performed a longitudinal study with a 48-week follow-up to evaluate sequential changes in PTH and 25-hydroxyvitamin D [25(OH)D] levels in patients starting cART with either tenofovir/emtricitabine or abacavir/lamivudine. Fifty-seven patients were included, 31 initiating tenofovir/emtricitabine and 26 initiating abacavir/lamivudine. Median PTH levels turned out to be significantly higher among tenofovir/emtricitabine users at week 4 (p=0.01), week 24 (p=0.008), and week 36 (p=0.02), and were above the upper limits of normal values (ULN) at weeks 24, 36, and 48 only in patients receiving tenofovir/emtricitabine. 25(OH)D, serum and urine calcium and phosphate, and renal-tubular maximum reabsorption of phosphate to the glomerular filtration rate (TmP/GFR) levels did not differ between the two treatment arms over the study period. Among tenofovir/emtricitabine users, median (interquartile range) PTH concentrations were significantly higher in patients with suboptimal 25(OH)D levels (<30 μg/liter) at week 24 [63 (57.8–82.4) ng/liter vs. 54.3 (34.4–63.067.5) ng/liter, p=0.05] and week 48 [67.5 (59.6–86.0) ng/liter vs. 41.9 (37.3–68.8) ng/liter, p=0.03]. A multivariable logistic regression model showed that tenofovir/emtricitabine use was an independent predictor of high PTH levels (≥53 ng/liter). Starting cART with tenofovir regimens is associated with an elevation in PTH plasma concentrations soon after introducing the drug. Suboptimal baseline 25(OH)D levels increase the risk of developing secondary hyperparathyroidism among tenofovir users.
The effects of combination antiretroviral therapy (cART) on bone metabolism constitute an area of ongoing investigation. Tenofovir has been associated with a decrease in bone mineral density (BMD) and increased bone turnover and osteomalacia. 1 –7 The pathogenesis of this bone toxicity remains to be well characterized. Although impaired phosphate balance and vitamin D metabolism related to renal toxicity have been implicated as likely mechanisms, 5,6,8 available information is controversial. 9 Cross-sectional data have suggested a relationship of tenofovir with secondary hyperparathyroidism in patients with low 25-hydroxyvitamin D [25(OH)D] levels. 10,11 However, longitudinal controlled studies assessing the impact of the initiation of a new antiretroviral regimen containing tenofovir on parathyroid hormone (PTH), 25(OH)D, and calcium/phosphate metabolism to support this hypothesis are lacking. Moreover, whether tenofovir exerts a deleterious effect on bone through PTH elevation in patients who lack overt 25(OH)D deficiency remains unknown.
We investigated longitudinal changes in PTH and 25(OH)D plasma concentrations in patients starting cART containing either of the two fixed-dose first-line nucleoside reverse transcriptase inhibitor (NRTI) combinations, tenofovir/emtricitabine or abacavir/lamivudine, during a 48-week follow-up.
Eligible patients were all HIV-infected adults (age, ≥18 years) cared for in the outpatient HIV clinic of a university hospital (Hospital General Universitario, Elche, Spain) initiating cART regimen including either tenofovir/emtricitabine or abacavir/lamivudine from December 2006 through March 2008. Candidates for inclusion were ART-naive patients, patients previously exposed to cART who had discontinued treatment for at least 6 months, and patients on stable cART willing to simplify their regimen. Patients who had ever received either abacavir or tenofovir and those with overt 25(OH)D deficiency (<20 μg/liter) 12 were excluded. Allocation to tenofovir/emtricitabine or abacavir/lamivudine was performed according to the criteria of the doctors in charge. The study was approved by the local Ethics Committee, and informed consent was obtained from all the patients.
Patients were evaluated at baseline and at weeks 4, 12, 24, 36, and 48. At each visit, blood samples were obtained for routine measurements, which also included calcium, phosphate, alkaline phosphatase (ALP), PTH, and 25(OH)D. 25(OH)D and PTH were assayed using a chemiluminescent automated enzyme-linked immunoabsorbent assay (DiaSorin Liaison; reference range for PTH, 4.6–26.8 pg/ml, interassay CV<10%; reference range for 25(OH)D, 30–100 ng/ml, interassay precision approximates 20% CV). Twenty-four-hour urine was collected at each visit, and creatinine, phosphate, and calcium were determined. Renal tubular maximum reabsorption of phosphate to the glomerular filtration rate (TmP/GFR) was calculated.
Differences in baseline characteristics and calcium homeostasis between patients initiating tenofovir/emtricitabine and abacavir/lamivudine were assessed using the chi-squared or Fisher's exact test for categorical variables and Mann–Whitney test for continuous variables. Forward binary multivariable logistic regression models were developed to quantify the association of high PTH levels with the cART backbone (tenofovir vs. abacavir), suboptimal 25(OH)D levels, and demographic and clinical data at the different time points of the study. Multivariate linear regression models with PTH as the dependent variable were also performed; 25(OH)D was here included as a continuous variable. All p values were two-tailed.
Ninety patients were initially included. Of them, 33 patients were excluded because they had ever received either abacavir or tenofovir, or had overt 25(OH)D deficiency (<20 μg/liter) at baseline. A total of 57 patients, 31 in the tenofovir/emtricitabine group and 26 in the abacavir/lamivudine group, were included in the analysis. Baseline characteristics of the patients are shown in Table 1. There were no significant differences in demographic or clinical data between patients starting therapy with tenofovir/emtricitabine or abacavir/lamivudine. Approximately one-third of the patients in each group were simplifying their NRTIs to a fixed-dose combination, and in most cases they were receiving zidovudine/lamivudine. In more than two-thirds of the patients in each arm, the third component of the regimen was a nonnucleoside reverse transcriptase inhibitor (NNRTI), mainly efavirenz. Other drugs accompanying the fixed-dose antiretroviral combinations were lopinavir/ritonavir, darunavir/ritonavir and raltegravir. No patients were receiving steroids, vitamin D or calcium supplements, or antiresorptive drugs, and there was no history of alcohol abuse among any of them.
Baseline Characteristics of the Patients
IDU, intravenous drug use; BMI, body mass index; eCrCl, estimated creatinine clearance; NNRTI, nonnucleoside reverse transcriptase inhibitors; PI, protease inhibitor. Numerical variables are median (interquartile range).
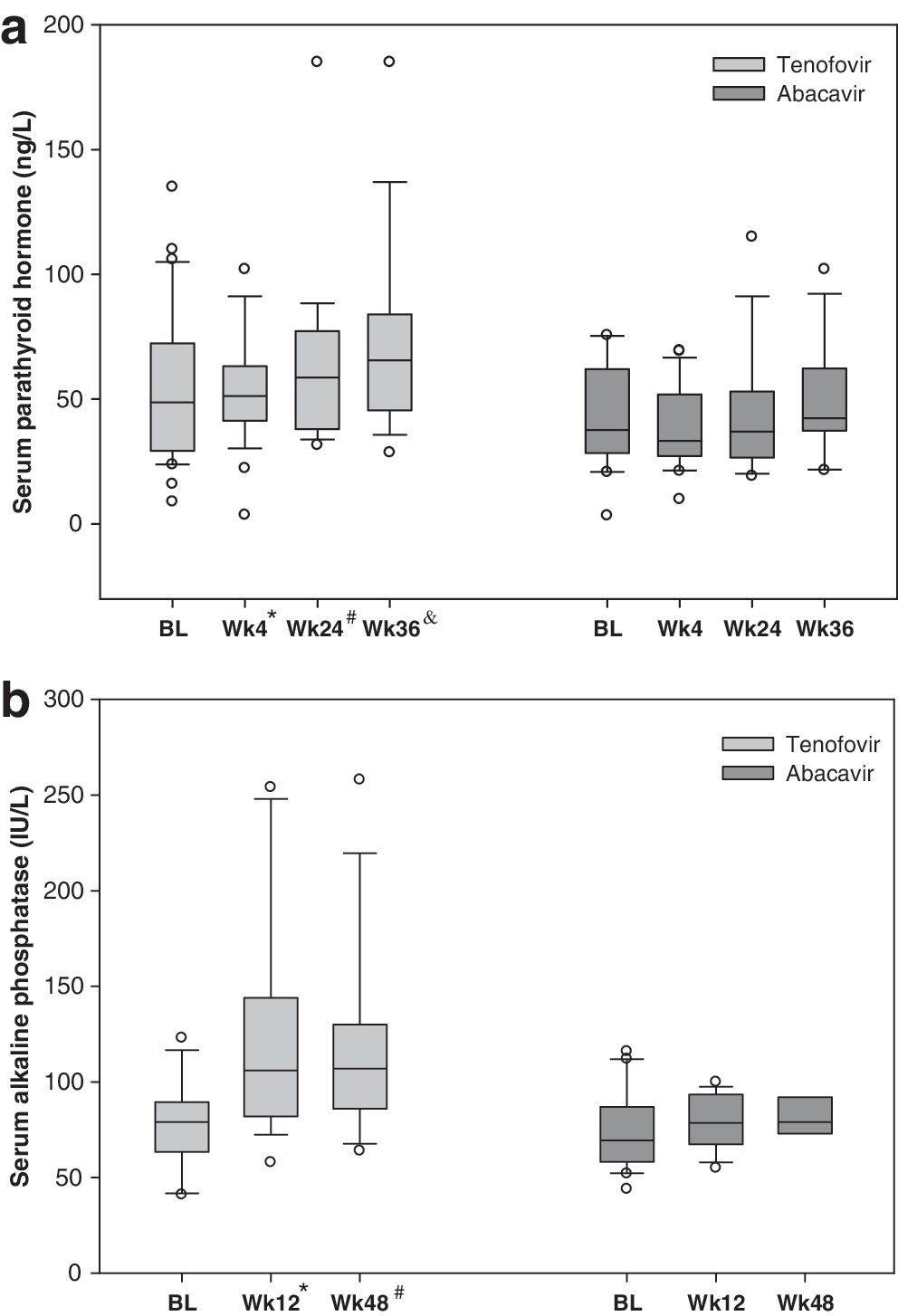
Baseline levels of PTH, 25(OH)D, serum or urine calcium/phosphate, and ALP were not statistically different between patients starting with tenofovir/emtricitabine or abacavir/lamivudine. The frequency of suboptimal 25(OH)D levels was not different between the two treatment arms [18 (58.1%) patients in the tenofovir/emtricitabine and 11 (42.3%) in the abacavir/lamivudine group, respectively, p=0.29]. After starting the new antiretroviral regimen, median PTH levels turned out to be significantly higher among tenofovir/emtricitabine users at week 4 (p=0.01), week 24 (p=0.008), and week 36 (p=0.02) (Fig. 1). Median PTH levels were found to be above the upper limits of normal values (ULN) in patients receiving tenofovir/emtricitabine at weeks 24, 36, and 48, while the same did not occur at any time point in patients initiating abacavir/lamivudine.
Levels of (
The proportion of patients who had PTH levels above the ULN (53 ng/liter) was significantly higher in those starting cART with tenofovir/emtricitabine than with abacavir/lamivudine at week 24 (68.4% vs. 23.5%, p=0.01) or week 36 (70.6% vs. 28.6%, p=0.03), and there was a trend at week 12 (42.1% vs. 17.4%, p=0.09). There were no differences in PTH levels by sex over the whole study period. In contrast to PTH, 25(OH)D levels did not differ between the two treatment groups throughout the study, although among the tenofovir/emtricitabine users there was a significant decrease in 25(OH)D at week 4 compared to baseline levels (p=0.03). No other significant changes in 25(OH)D were observed in any of the study groups.
The proportion of patients with suboptimal 25(OH)D levels was not different between treatment groups during the study. ALP was higher after the beginning of the new regimen among tenofovir/emtricitabine users than in abacavir/lamivudine users at week 12 (p=0.006) and week 48 (p=0.038) (Fig. 1). The percentage decrease in serum calcium from baseline was higher in patients starting abacavir at week 12 than in patients starting tenofovir. No other differences were seen in percentage change in serum calcium or phosphate levels between the study groups. Plasma and urine calcium and phosphate, estimated creatinine clearance, and TmP/GFR remained nonsignificantly different between the groups throughout the study period, and the frequency of low TmP/GFR (<85%) was also not different between the groups during the study.
There was an inverse correlation between PTH and 25(OH)D levels at week 4 (Spearman's rho=–0.28, p=0.05) and week 48 (Spearman's rho=–0.46, p=0.01). Among tenofovir/emtricitabine users, PTH concentrations were significantly higher in patients with suboptimal 25(OH)D levels (<30 μg/liter) 12 than in those with ≥30 μg/liter at week 24 [63 (57.8–82.4) ng/liter vs. 54.3 (34.4–63.067.5) ng/liter, p=0.05] and week 48 [67.5 (59.6–86.0) ng/liter vs. 41.9 (37.3–68.8) ng/liter, p=0.03], while a trend to higher PTH levels at week 48 (p=0.09) was seen in patients with suboptimal 25(OH)D levels receiving abacavir/lamivudine.
Among patients with suboptimal 25(OH)D status, median (interquartile range) PTH was higher among tenofovir/emtricitabine users than among abacavir/lamivudine users at week 4 [52.5 (41.9–60.3) ng/liter vs. 35.6 (30.9–55.9) ng/liter, p=0.04], week 24 [62.4 (55.2–79.8) ng/liter vs. 35.1 (21.8–54.8) ng/liter, p=0.007], and week 36 [56.7 (47.9–101.0) ng/liter vs. 41.2 (37.5–65.7) ng/liter, p=0.09]. To identify predictors of hyperparathyroidism (defined as a PTH ≥53 ng/liter), potential risk factors such as age, sex, smoking habit, weight, lipodystrophy, hepatitis C virus infection, serum calcium and phosphate levels, suboptimal 25(OH) D levels (<30 μg/liter), and cART including tenofovir/emtricitabine vs. abacavir/lamivudine were analyzed.
In univariate analysis, patients with hyperparathyroidism had a higher frequency of lipodystrophy at baseline (45% vs. 11.4%, p=0.008), lower serum calcium levels at week 4 (p=0.04), both lower serum calcium levels (p=0.04) and more frequent tenofovir-containing regimen (p=0.01) at week 24, and more frequent tenofovir-containing regimen (p=0.03) and a trend to a higher frequency of lipodystrophy (p=0.08) at week 36. Multivariable logistic regression models showed that the use of tenofovir/emtricitabine [OR (95% confidence interval) 9.60 (1.86–49.48), p=0.007] and lower serum calcium levels [OR 0.02 (0.001–0.74)] were independent predictors of high PTH levels at week 24, and the use of tenofovir/emtricitabine was the only independent predictor of high PTH levels at week 36 [OR 7.20 (1.35–38.33), p=0.02]. Multivariate linear regression models with PTH concentration as the dependent variable showed that the use of tenofovir/emtricitabine was an independent predictor of PTH levels at week 4 (p=0.02), week 24 (p=0.02), and week 36 (p=0.04), while 25(OH)D levels did not predict PTH values at any time point.
In this study, we demonstrate that the impact on the hormones that regulate calcium homeostasis, and specifically on PTH levels, of a new ART regimen based on tenofovir/emtricitabine differs from that of a regimen including abacavir/lamivudine. Patients initiating cART with tenofovir/emtricitabine achieved significantly higher PTH concentrations at weeks 4, 24, and 36 than patients initiating abacavir/lamivudine-based cART, with median PTH values above the ULN throughout the second half of the study. Additionally, there was a link between the highest PTH values and suboptimal 25(OH)D levels at some time points of the study only among tenofovir/emtricitabine users. ALP levels were also higher among tenofovir/emtricitabine users at weeks 12 and 48. Conversely, we did not find differences in 25(OH)D levels or in the proportion of suboptimal 25(OH)D values between both treatment groups at any of the study visits.
The early increase in PTH observed in our study in patients starting tenofovir might suggest the possibility that the upregulation of this hormone plays a role in the decrease of BMD associated with the initiation of cART containing tenofovir. Such effects start soon after introducing the drug, and last for at least the first 36 weeks of therapy. We also demonstrated a relationship between the highest PTH levels and the lowest 25(OH)D concentrations, as previously suggested in cross-sectional data, 10,11 but, importantly, the elevation of PTH and its relationship with the lowest 25(OH)D concentrations occurred even after excluding subjects with baseline 25(OH)D deficiency. This underscores the role of the interaction between vitamin D and PTH, and suggests that patients with suboptimal, although nondeficient, baseline 25(OH)D levels might be at higher risk for developing hyperparathyroidism than patients with adequate 25(OH)D levels when they begin new cART containing tenofovir.
By contrast, although levels of 25(OH)D or the proportion of patients with suboptimal 25(OH)D were not different among treatment arms, the same effects were not observed among abacavir/lamivudine users. Despite higher PTH levels among tenofovir/emtricitabine users, serum and urine calcium and phosphate concentrations and TmP/GFR were not different between treatment arms during the study. This might reflect the stability of calcium/phosphate homeostasis, and suggests that PTH levels may be a sensitive marker to monitor the effects of cART on bone metabolism.
Our study is limited by its nonrandomized design and small sample size. However, baseline characteristics were similar between treatment groups and despite the small sample size, we were able to detect significant increases in PTH and ALP in patients initiating tenofovir. The strengths of the study are the longitudinal design, the systematic measurement of the hormones and other markers of calcium/phosphate homeostasis from the beginning of the new antiretroviral regimen, and the homogeneity of the NRTI backbone used, which allowed a comparison of the effects on bone metabolism of the current first-line fixed-dose combinations for the treatment of HIV-infected patients.
In conclusion, starting a new cART including tenofovir/emtricitabine is associated with an increase in PTH concentrations, which is not observed when initiating abacavir/lamivudine. This difference can be noticed soon after starting the new regimen, and lasts for at least the first 36 weeks of therapy. Patients with baseline suboptimal 25(OH)D levels are at a higher risk of developing the highest PTH levels, and therefore vitamin D supplementation might be considered in these patients, even in the absence of overt 25(OH)D deficiency, when their doctors are willing to start tenofovir-based cART.
Footnotes
Acknowledgments
Supported in part by FIBELX (05/05, 07/20, 10/11, 10/12, 10/13), FIS (PI081893), Generalitat Valenciana (PI051338, 083/05, AP-091/07, AP-087/10), FIPSE (12655/07), and ISCIII-RETIC RD06/0027-Red Temática Cooperativa de Investigación en SIDA.
Author Disclosure Statement
Mar Masiá Sergio Padilla and Felix Gutiérrez have served as scientific advisers to or have spoken at events sponsored by Gilead, Bristol-Myers Squibb, GlaxoSmithKline and Viiv Healthcare, Abbot, and Janssen-Cilag Laboratories.