
Abstract
Human immunodeficiency virus type 2 (HIV-2), originally restricted to Western Africa, is now spreading to Western European countries because of migration from endemic areas. Therefore, it is mandatory to enforce the surveillance and improve the diagnostics of this neglected infection. In this report, we describe a case of HIV-2 infection affecting an Italian citizen along with three cases from India. Phylogenetic analysis showed that the viral strain identified in the Italian patient clustered with a strain isolated from an immigrant living in France. Of the three Indian strains, two clustered together and were statistically supported, whereas one clustered with a strain from Guinea Bissau. The description of the first case of HIV-2 infection in an Italian citizen indicates that the virus is spreading from endemic areas to countries involved in migration. A strict monitoring and improvement of the diagnostic molecular tools are necessary to avoid misdiagnosis with relevant clinical consequences.
Introduction
H
The incidence of HIV-2 infection declined over the years 1990–2000, 8,9 with a number of infections mostly caused by groups A or B. Up to now, six groups of HIV-2 have been identified: A to F. 10,11
This infection may be appreciable in countries with a high number of foreign citizens such as Italy where a considerable number of immigrants also come from Western African countries (
The surveillance and correct diagnosis of HIV-2 infection may be important for both appropriate therapy and reductions in the risk of transmission. Here, we describe four cases of suspected HIV-2 infection confirmed by Western blot analysis, real-time polymerase chain reaction (PCR), and phylogenetic analysis.
Material and Methods
Samples collection
Plasma samples from one Italian and three Indian patients tested previously positive to HIV-1/2 antibodies were collected and stored at −80°C until analysis. The Italian sample was collected in Rome, whereas the Indian samples were from the following cities: Bombay (Maharashtra State), Hubli (Karnataka State), and Lucknow (Utter Pradesh State). The demographic and clinical features of the patients are reported in Table 1.
Western blot analysis
To confirm and define the positivity to HIV antibodies, a Western blot assay was carried out according to the manufacturer's instructions (INNO-LIA HIV I/II Score, Innogenetics, Ghent, Belgium).
Real-time PCR and sequencing analysis
HIV-1 was searched by real-time PCR using the Abbott RealTime HIV-1 assay according to the manufacturer's instructions (Abbott molecular, Des Plaines, IL). Plasma RNAs were run on the m2000 system, a platform capable of automated RNA extraction and PCR set-up, followed by amplification/detection.
HIV-2 was instead detected by an HIV-2 Real Time RT-PCR kit (Shanghai ZJ Bio-tech Co., Ltd., Shanghai, China). Plasma samples were extracted by a QIAamp Viral RNA Mini kit (Qiagen, Milan, Italy) and 5 μl was added to the PCR mix according to the indications of the manufacturer. Positive samples were further characterized by amplification and sequencing of a 546-bp fragment of the HIV-2 V3 region. 12
Phylogenetic analysis
The HIV-2 env sequence (V3 region
12
) of four patients (IT1, IN 1, 2, and 3) were aligned and compared using two different data sets: (1) reference sequences downloaded from the Los Alamos database (
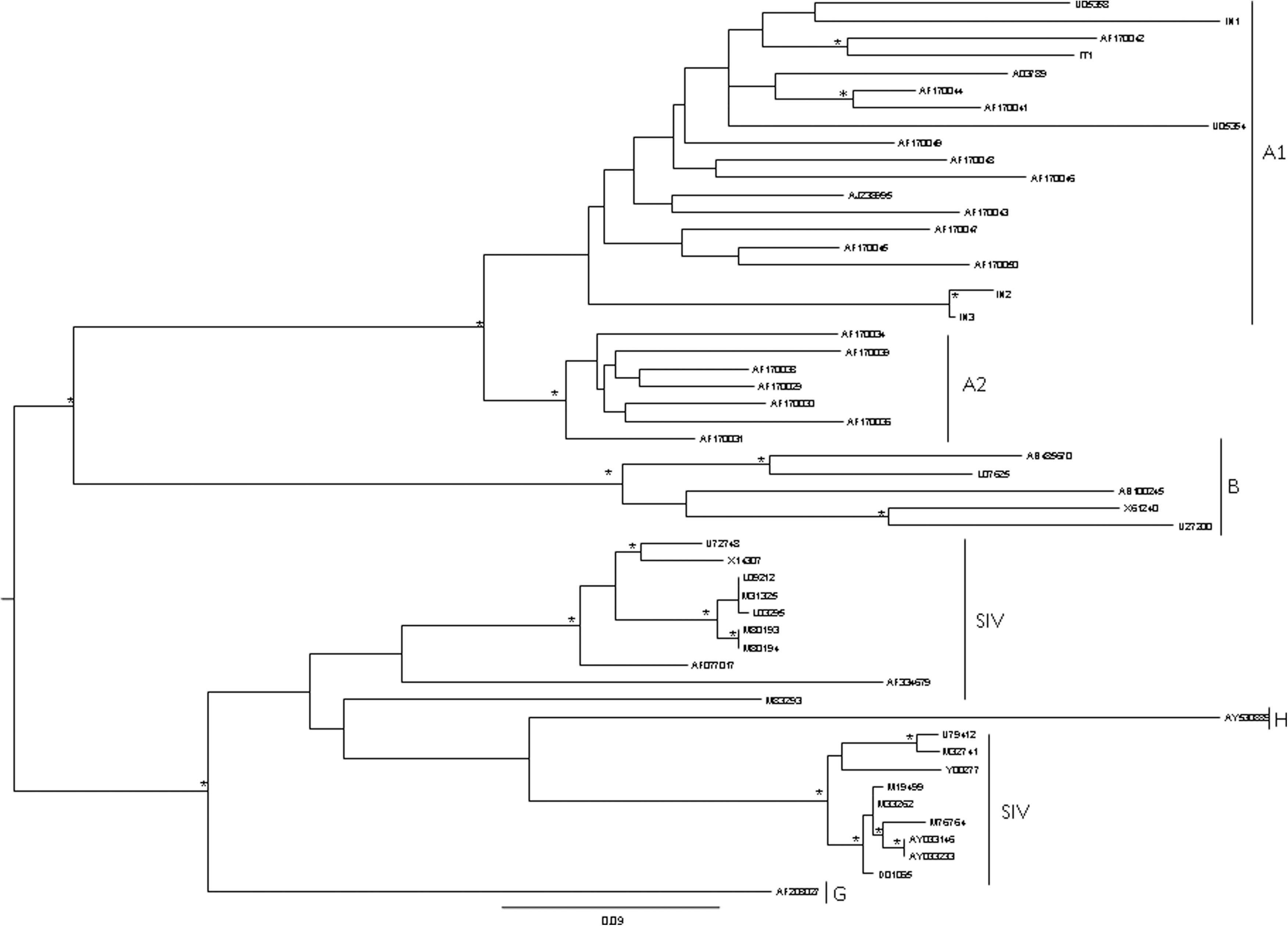
Phylogenetic relationships of the Italian and Indian HIV-2 isolates with the subtype-specific reference sequences downloaded from the Los Alamos sequence database (
The phylogenetic tree was constructed using the PAUP package. 13 We employed the general reversible model (HKY) of nucleotide substitution, incorporating maximum likelihood (ML) estimates of base composition and the shape parameter (ω) of a gamma distribution (γ) model of among-site rate variation as it consistently gave much higher likelihood values using Modeltest v.3.7 implemented in PAUP. 13 The maximum likelihood tree was estimated under this model using tree bisection-reconnection (TBR) branch swapping. The statistical robustness and reliability of the branching order within each phylogenetic tree were confirmed through a bootstrap analysis using 1000 replicates for the neighbor-joining (NJ) tree and through the zero branch length test for the ML tree. 13 The tree was rooted with a midpoint rooting.
Nucleotide sequences accession number
The nucleotide sequences obtained with this study have been deposited in GenBank under the following accession numbers: JF717827–JF717830.
Results
Real-time PCR and Western blot assays showed that the four patients were infected by HIV-2, while HIV-1 was not detected either at the nucleic acid or antibody level. In addition, phylogenetic analysis of the V3 region of HIV-2 12 indicated that the four patients were infected by HIV-2 subtype A, most likely subgroup A1 (Fig. 1). The uncertainty about the subgroup is due to the fact that only a portion of the env gene was analyzed and not the entire viral genome. The sequence obtained from the Italian patient (IT1) clustered with a sequence isolated from a patient living in France. Of the three Indian sequences, one (IN1) clustered with a sequence identified in a patient from Guinea Bissau, while the other two sequences (IN2 and IN3) clustered together and the cluster was statistically supported (Fig. 1.)
Discussion
The circulation of HIV-2 is mainly restricted to countries of West Africa. However, immigration from this African region has led to the spread of the virus to other continents with most of the cases diagnosed in France and Portugal. 14 In Italy, the attention in regard to this neglected infection recently increased, especially among immigrants. 15 To our knowledge, however, no reports have been published on HIV-2 infection among Italian citizens. Here, we describe the first Italian case of HIV-2 infection along with three cases from India. A phylogenetic analysis was carried out to determine the genetic features of these four HIV-2 strains. Of the three Indian strains, two were highly related, suggesting that they shared the same source of infection. The third sequence clustered with a strain from Guinea Bissau. However, the similarity between this Indian strain and the Guinea Bissau strain is not suggestive of a recent common ancestor.
About the Italian strain, it clustered with a sequence isolated in France. 14 It seems that the common ancestor of these two viruses was in Africa with two importations into Europe, indicating that this clade of viruses has been evolving in France and Italy for decades. Likewise, the phylogeny cannot indicate the direction of travel, and it is as likely that the French virus came through Italy as it is that the Italian virus came through France.
In addition, the description of the first Italian case indicates the importance of strengthening the surveillance system for HIV-2 because of the increase in migration from endemic areas to Italy. This problem is clinically relevant because patients whose HIV-2 serostatus is unknown may be treated with inappropriate drugs.Therefore it is important to have valid diagnostic tools, i.e., antibody and Western blot assays, able to distinguish between HIV-1 and HIV-2 infection and valid real-time PCR to determine the HIV-2 viral load.
Footnotes
Author Disclosure Statement
No competing financial interests exist.