
Abstract
More than 50 HIV-1-infected patients, naive of antiretroviral therapy (ART) but eligible for first line ART in JJ Hospital, Mumbai, India were investigated for surveillance drug resistance mutations (SDRMs); all but one virus belonged to subtype C; we could observe SDRMs to nonnucleoside reverse transcriptase inhibitors and protease inhibitors in 9.6% of the patients.
Introduction
F
WHO has published recommendations on the survey of TDR in areas in which ART has been initiated for more than 3 years and has proposed thresholds of TDR (<5%, 5–15%, and >15%) 3 ; in an effort to increase the accuracy of identifying TDR mutations, Bennett et al. have recently updated the surveillance drug-resistant mutation (SDRM) list where, considering B and major non-B subtypes, a distinction is made between TDR mutations and polymorphism substitutions. 4 For example, M36I (methionine converted to isoleucine at protease position 36) is an accessory resistance mutation for subtype B that was reported to increase viral fitness and confer resistance to ritonavir and nelfinavir, but it is also observed as a natural polymorphism in non-B isolates (for example, C and CRF02_AG) from patients who have never been exposed to protease inhibitors (PIs).
Current guidelines in resource-rich settings suggest resistance testing at initiation of care, regardless of whether highly active antiretroviral therapy (HAART) is planned or whether the infection occurred recently. In resource-limited settings, the WHO recommends surveillance of TDR as a comprehensive approach to HIV care. 5
In Mumbai, India, a recent study 6 carried out on clients of voluntary counseling and testing centers (VCTCs) has not demonstrated any SDRM and it was concluded that the prevalence of SDRMs in this population, considered to have been recently infected, was below the WHO 5% threshold.
The aim of our study was to investigate potential HIV resistance in patients naive to ART but eligible for first line therapy.
Materials and Methods
Sixty-eight patients, HIV-1 infected and naive of ART, exhibiting less than 350 CD4 lymphocytes/μl and eligible for first line ART (d4T/AZT-3TC-EFV/NVP) were successively assigned to the study without any bias; their plasmas were blotted on Whatman 903 paper (dry plasma samples: DPS) and the DPS were dried at room temperature before being placed in plastic bags with desiccant for carryover to Bordeaux, France; the viral RNA was extracted and the reverse transcriptase (RT) and protease (Prot) sequences were amplified before being sequenced as previously described. 7 The sequences were aligned with reference sequences of HIV-1 group M from the Los Alamos database and phylogenetic trees were constructed using the Clustal software. The DRMs were deduced from the 2009 list of SDRMs for survey of TDR. 4
The GenBank accession numbers are JF414419 to 414468 (Prot) and 414469 to 414519 (RT).
Results
Out of 68 samples, 52 and 51 could be amplified in Prot and RT regions, respectively. All RT sequences clustered with subtype C while 51 Prot clustered with C and one with A; therefore, based on this analysis which was limited to the RT-Prot region, all isolates were of subtype C but one recombinant was A/C. We could observe SDRMs, which are listed in Table 1; there was no mutation to NRTIs but there were mutations to NNRTIs (K103N and V106M) and to PIs (M46I). Globally, five isolates were bearing SDRMs (9.6%), three to NNRTIs, one to NNRTIs+PIs, and one to PIs alone (Fig. 1).
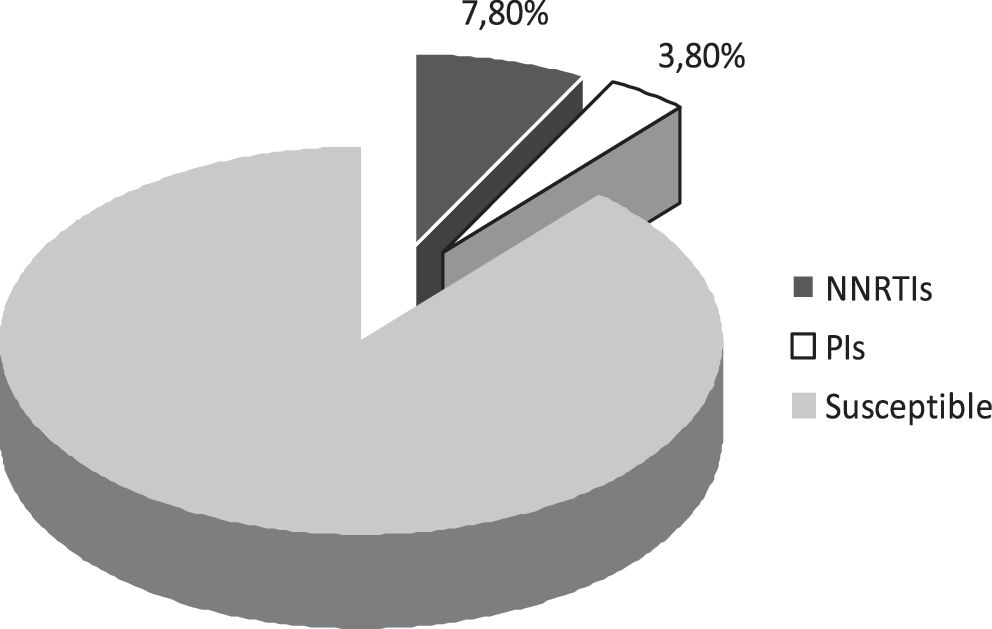
Prevalence of drug resistance to nonnucleoside reverse transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs).
NNRTIs, nonnucleoside reverse transcriptase inhibitors; PIs, protease inhibitors.
Discussion
Clearly, there are SDRMs to two drug classes in these naive patients eligible for first line ART. All of them denied prior use of antiretroviral drugs and they did not include women who had been treated with NNRTIs in the context of PMTCT. The population studied does not fit with the populations recommended by WHO consisting of recently infected patients in VCTCs or pregnant HIV-infected women; nevertheless, the lesson that can be drawn is that 4 out of 51 patients (8% considering the RT sequences available) eligible for first line ART harbor HIV-1 strains that are fully resistant to one drug of the corresponding ART regimen.
We were surprised to find SDRMs to PIs (M46I) and not to NRTIs (particularly M184V/I to 3TC and revertant mutations at position 215 to d4T/AZT). SDRMs have already been described in naive patients of North India, 8 Southeastern India (Chennai), 9 and Western India (Pune). 10 The predominant SDRMs in our study are K103R and V106M, and this figure is similar to what has been described in a cohort of South Africa. 11 In general, NNRTI mutations do not impact viral replicative fitness to the same extent as either NRTI or PI mutations; studies have shown that such mutants can achieve long-term persistence (several years) in blood and genital tract secretions 12 and this is a potential explanation for the presence of SDRMs in these Indian patients having been infected for a long time and eligible for first line ART. In North America and Western Europe, the recommendation is to carry out genotyping analysis of HIV prior to initiation of first line therapy; in the case of India, where this assay is expensive and is still restricted due to financial conditions, we would propose to engage longitudinal random surveys of patients who meet the criteria for first line therapy.
Footnotes
Acknowledgments
This study has been funded through a quadriennal grant to CNRS UMR 5234.
Author Disclosure Statement
No competing financial interest exists.