
Abstract
In Nigeria, the country with the second largest number of HIV-1-infected people globally, antiretroviral therapy rollout is now widespread with an increasing number of individuals and communities benefitting. However, the drug resistance profile of patients initiating or failing on antiretroviral therapy is not well characterized. Here we studied the molecular variability of the protease and reverse transcriptase region of isolates from therapy-naive pregnant women in North-Central Nigeria (one of the geopolitical zones with the highest prevalence of HIV in Nigeria) to identify baseline mutations with potential drug resistance implications. We observed the predominance of CRF02_AG and subtype G in the North-Central Nigerian epidemic and the presence of both primary and secondary drug resistance mutations. Contrary to observation from other geopolitical zones, a decreased frequency of reverse transcriptase mutations/polymorphisms was observed, thus suggesting regional differences in level of transmitted drug resistance that require more study.
N
Characterization of the PR and RT sequences was carried out by amplifying, cloning, and sequencing DNA after reverse transcription of plasma RNA. Briefly, after extracting RNA from plasma using the QIAamp Viral RNA mini kit (Qiagen) according to the manufacturer's instructions, reverse transcription was carried out as described previously. 2 DNA amplification of PR and RT was modified from Ojesina et al. (2006) using the following PCR conditions: for the first round reaction, initial denaturation at 94°C for 10 min, followed by 40 cycles at 94°C for 30 s, 48°C for 35 s, and 72°C for 60 s, and same for the second round reaction except that the annealing temperature was 45°C. Cloning of RT was modified from Singh et al. 3 using the TOPO TA Cloning Kit (with pCR2.1-TOPO vector) with One Shot TOP10 Chemically Competent E. coli (Invitrogen). Sequences were assembled and edited with Sequencher 4.8 and aligned with reference sequences obtained from the Los Alamos HIV database using BioEdit 5.0.9, with manual editing as necessary. The GTR (general time reversible) model was chosen to be the best fitting nucleotide substitution model using a web-based tool, FindModel. Maximum likelihood (ML) trees were obtained by starting with a neighbor-joining tree and using SPR (subtree pruning and regrafting) heuristic search algorithms. Calculations were performed with Phylogenetic Analysis Using Parsimony (PAUP*) 4.0b10 written by David L. Swofford. Statistical support for ML phylogeny structures was evaluated by bootstrapping analysis of the original sequence alignments (1000 NJ replicates). Trees were rooted by outgroup (HXB2) and presented using the program FigTree 1.3.1 written by Andrew Rambaut.
Of 28 samples amplified, 14 (50%) were found to be concordantly CRF02_AG in both genes. Though one of the isolates did not cluster within the other CRF02_AG isolates on the RT ML tree, it was confirmed to be CRF02_AG using a combination of Recombinant Identification Program: RIP 3.0 from the Los Alamos HIV database and SimPlot version 3.5.1. The other predominant subtype was subtype G, which was found to be 39.93% (n=11) of both genes. Also concordantly obtained in both genes were one subtype C and one subtype F2. However, the last isolate was classified as subtype G in PR and CRF06_cpx in RT. We speculate that the isolate is likely to be CRF06_cpx, because the same isolate was seen in our previous study 2 to be CRF06_cpx in gag (though CRF02_AG in env) and CRF06_cpx PR is identical to subtype G PR. 4 This result (Fig. 1) shows that the diversity of HIV-1 in North-Central Nigeria is complex and is consistent with other regions in Nigeria. 2
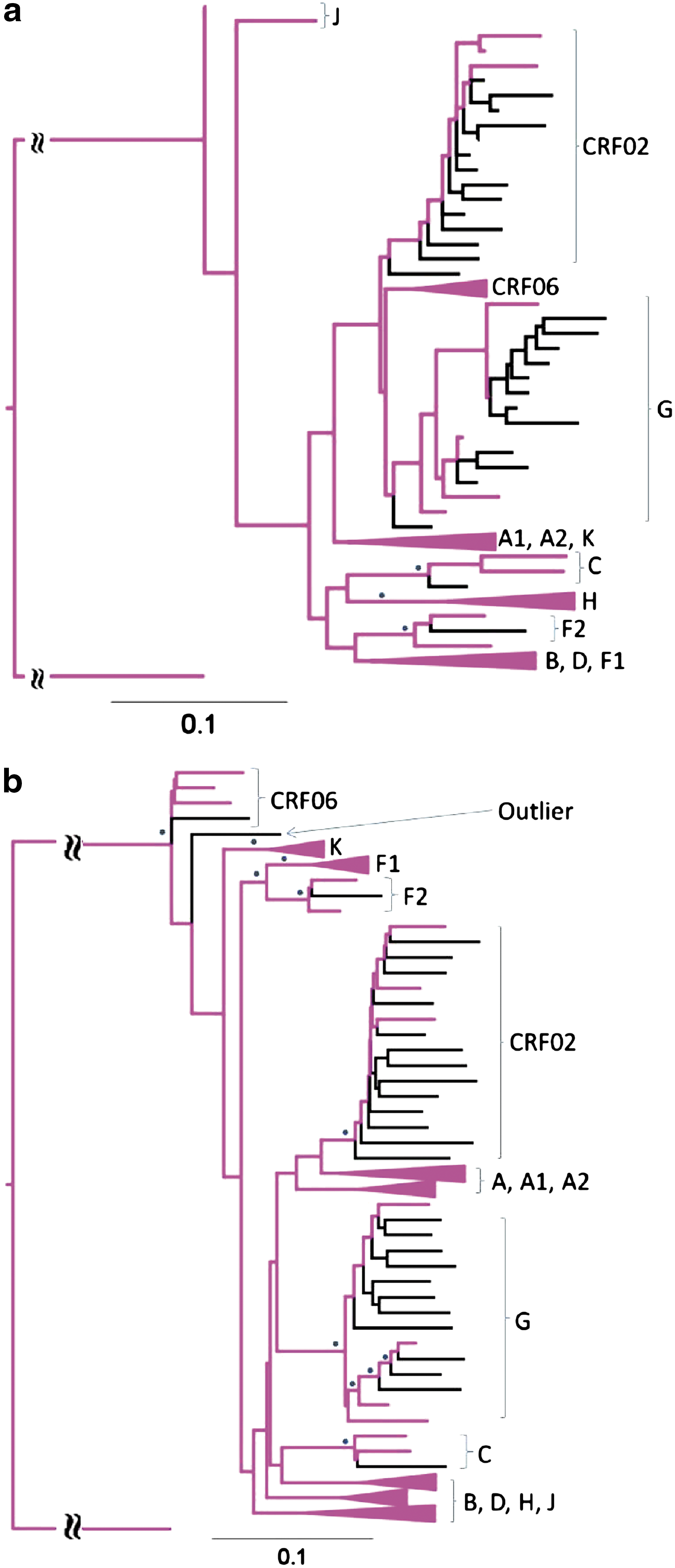
Maximum likelihood tree of
The PR and RT nucleotide sequences were translated to amino acid sequences using Molecular Evolutionary Genetics Analysis (MEGA) software version 4.0.2 and submitted to the Stanford HIV Drug Resistance Database (
As expected for therapy-naive HIV-1 isolates, all showed full potential susceptibility to protease inhibitors, except one subtype C that may have potential low resistance to nelfinavir due to T74S, a minor mutation that can be present in untreated patients with subtype C, which has been found to restore fitness of multidrug-resistant viruses in both subtypes B and C. 5 Minor polymorphic mutations associated with resistance to protease inhibitor in subtype B (usually when present in combination with other mutations) were present but had no effect on resistance according to the database algorithms. The important polymorphic mutations included L10I (in two subtype G samples), which is associated with resistance to most PIs when present with other mutations and found in 5–28% of therapy-naive viruses, 6 V11I (in one subtype G sample), which is one of the 11 mutations associated with a decreased response to darunavir in the POWER trials, 7 and two minor tipranavir resistance mutations 8 (L10V and M36 I). The L10V was found in two CRF02_AG and the only subtype F2, whereas M36I was found in all isolates. Other polymorphic mutations present were I13V [in all subtype G and most (13/14) of CRF02_AG], G16E [in some (6/14) CRF02_AG], K20I/R (in all except subtype C), L33V (in the subtype F2), D60E (in one CRF02_AG and subtype F2), I62V (in subtype F2), L63P (in three CRF02_AG and two subtype G), V82I (in all subtype G), L89M (in all except subtype F2), and I93L (in subtype C).
Figure 2 shows the proportion of the various accessory (polymorphic) mutations observed in all CRF02_AG and subtype G isolates. Our findings on the high prevalence of K20I/R (27/28) and M36I (28/28) are consistent with previous studies 9,10 on DRMs in therapy-naive viruses from Nigeria. Also, the presence of V82I in all our subtype G isolates and the presence of L63P in approximately 20% of both our CRF02_AG (3/14) and subtype G (2/10) isolates is consistent with previous observations on Nigerian therapy-naive isolates of the respective subtypes. 10 V82I has previously been documented in 20.7% (6/29) of subtype G sequences from different parts of the world, and in combination with K20I and M36I was found to result in 2.9-fold decreased susceptibility to amprenavir. In the presence of the three substitutions and L63P, 3.9-fold decreased susceptibility to both nelfinavir and ritonavir was observed. Expectedly, the only Nigerian sequence in the same study had K20I, M36I, and V82I polymorphisms. 11 Decreased susceptibility to protease inhibitors in CRF02_AG isolates has also been linked to polymorphisms at protease positions 20, 36, and 63. 12 These data suggest that salvage therapy regimens, which usually contain protease inhibitors, may not fully benefit Nigerian patients because of the presence of crucial baseline polymorphisms.
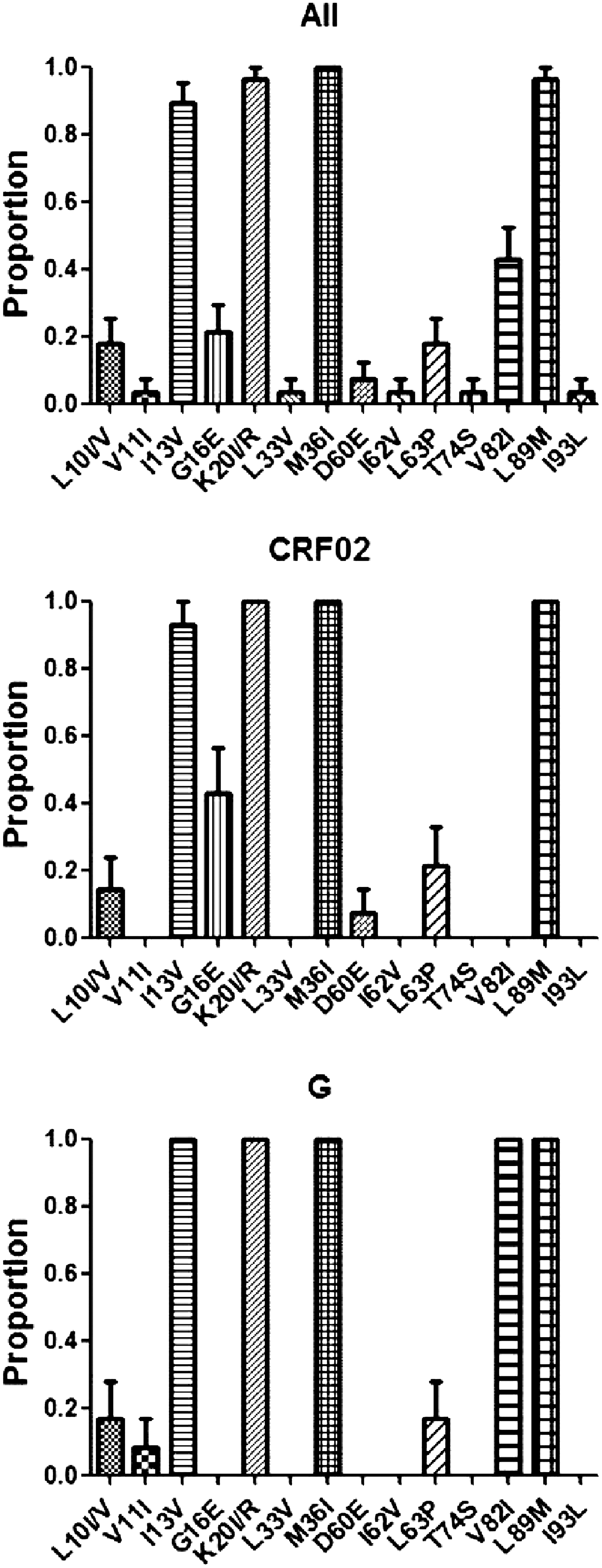
Prevalence of polymorphic mutations in protease associated with resistance in subtype B, observed in all the sequences, CRF02_AG sequences alone and subtype G sequences alone.
All the RT sequences were shown to be fully susceptible to nucleoside reverse transcriptase inhibitors (NRTI). However, minor mutations associated with resistance to NRTI whose effect on NRTI susceptibility are unknown were seen. These mutations were T69S found in one subtype G and a highly unusual M184T found in one CRF02_AG. While there was no major DRM against protease inhibitors and NRTI, DRM against nonnucleoside reverse transcriptase inhibitors (NNRTI) were found at three RT sites (K101E, V179E, and Y181C), predicting low to high level resistance against NNRTI for the isolates concerned. 13 K101E, which is associated with intermediate level resistance to delavirdine and nevirapine and low level resistance to efavirenz and etravirine, was found in one CRF02_AG. V179E and Y181C, associated with high level resistance to delavirdine and nevirapine and intermediate level resistance to efavirenz and etravirine were found in the only CRF06_cpx RT sequence. Minor NNRTI mutations that do not reduce NNRTI susceptibility were also found; A98S in one CRF02_AG, V179I in the only subtype C and a highly unusual M230T in one CRF02_AG. Our finding on CRF06_cpx is consistent with a previous study on DRMs in therapy-naive viruses from Nigeria, 10 which has shown that CRF06_cpx therapy-naive isolates had significantly more DRM for RT inhibitors than other subtypes.
The observation on the presence of PR DRMs in these therapy-naive HIV-1 isolates from North-Central Nigeria corroborates what has been observed previously on Nigerian therapy-naive HIV-1 isolates from different geopolitical zones. 9,10 Since the presence of mutations/polymorphic substitutions observed in therapy-naive isolates could lead to a reduction in the response to antiretroviral therapy, proper monitoring (in term of at least genotypic analysis of viral population) of Nigerian patients before and during administration of antiretroviral therapy is important. Although this monitoring is not presently routinely carried out, it is important considering that the Nigerian HIV-1 epidemic is driven by different subtypes.
These different subtypes may have different levels of response to antiretroviral drugs or different pathways to resistance. However, contrary to previous observations 10 we found a decreased frequency of RT DRMs. The reason for this discrepancy could be the result of differences in the level of transmitted drug resistance (TDR) in the different geopolitical zones sampled, theirs being from South-West and ours from North-Central. Another difference is that Ojesina and colleagues sampled from one state in the South-West, while we sampled from four states, which may not all have antiretroviral therapy widely available. It is also possible that antiretroviral drug resistance has accumulated and been transmitted more in South-West Nigeria due to older and more widespread HIV intervention programs in the South compared to the North. 14 Unlike in developed countries where the TDR rates are known to be as high as 25%, 15 the prevalence of NRTI and NNRTI TDR is largely unknown in Nigeria. There is hardly any phenotypic data available from therapy-naive patients in Nigeria, and the diversity of circulating subtypes is unique, making extrapolation of data from elsewhere difficult.
This study contributes to the scarce data on HIV in North-Central Nigeria (and Nigeria as a whole) and has shown that the complexity of HIV-1 in North-Central Nigeria is similar to other regions in the country. In agreement with previous studies, this study showed the presence of important PR mutations/polymorphic substitutions in isolates from antiretroviral therapy-naive North-Central Nigerians, which could lead to a reduced response to antiretroviral therapy. This study also suggests that there are regional differences in TDR rates that require more study.
Sequence Data
The GenBank accession numbers for the sequences reported in this article are HM854101–HM854128 for the protease sequences and HM854129–HM854156 for the reverse transcriptase sequences.
Footnotes
Acknowledgments
H.O.A. was supported by the Third World Organization for Women in Science (TWOWS) postgraduate fellowship from the Third World Academy of Sciences (TWAS). This study was supported by funding from the Hasso Plattner Foundation and the South African Research Chair in Systems Biology of HIV/AIDS to T.N.
Author Disclosure Statement
No competing financial interests exist.