
Abstract
We sought to identify and summarize the incidence and prevalence of neuropathy among HIV patients and subgroups. A systematic search of the literature was performed using MEDLINE and EMBASE. The relevant literature was identified based on predefined criteria. Prevalence data were collected from cross-sectional and cohort studies. Incidence data were collected from cohort and case-control studies. Thirty-seven studies were included of which there were 23 cohort studies, 13 cross-sectional studies, and one case-control study. The prevalence of neuropathy among HIV patients derived from 25 studies varied from 1.2% to 69.4%. Regarding the development of neuropathy among HIV-positive patients, standardized by study duration, the rates per 100 person-years ranged from 0.7 to 39.7. Among older patients there is a greater risk of neuropathy. The same seems to be the case for patients with more severe disease. Currently available studies providing information on the incidence and prevalence of neuropathy among HIV patients suggest a significant burden, but there is a great variation in results across studies. There is no definitive explanation for the variation. However, it underscores the fact that complexity of the disease, along with absence of standardized diagnostic criteria, has considerably influenced the methodologies and outcomes of the studies.
Introduction
HIV
Distal sensory polyneuropathy (DSP) is the most common form of peripheral neuropathy (PN) experienced by HIV-positive patients. Although it is predominantly found in advanced stages of infection, pathological evidence of neuropathy is universal among HIV-infected patients at autopsy. 5,6 DSP is marked by nerve damage affecting motor and sensory function, with spontaneous or evoked pain that may follow an acute or chronic pattern, including symptoms of numbness, weakness, burning pain, pins and needles sensations, and reduced reflexes. 7 Symptoms present in the peripheral extremities commonly progress in severity and location over time in chronic cases. 8,9 Pain associated with PN may lead to anxiety, depression, sleep disturbances, and other comorbidities, reducing an individual's quality of life. 10 –13 Neuropathic pain may also adversely affect productivity and is associated with substantial costs. 10 –14
Patient- or clinician-administrated screening tools, such as the Brief Peripheral Neuropathy Screen (BPNS), have been developed to aid in the identification of HIV-infected individuals suffering from neuropathy and reporting symptoms. Quantitative sensory tests (QST) provide improvement in the diagnosis of DSP when utilized in combination with clinical measures. However, a “gold standard” test for HIV-associated neuropathies does not exist. 15,16
The occurrence of DSP is thought to be influenced by several factors. 10,17 –24 The abnormal peripheral nerve function is suspected to be caused indirectly by HIV. 13 It is believed that DSP is immune-mediated (i.e., resulting from abnormal activity of the immune system). It has also been proposed that DSP may result from an immune reaction caused by the release of potentially neurotoxic compounds, including cytokines, free radicals, and lipid membrane derivatives. 18 Since the mid-1990s HAART, which is a combination of at least three antiretroviral (ARV) drugs, has become a mainstay of HIV treatment. 19,20 On the one hand, HAART improves immunosuppression, which in turn reduces the risk of neuropathy, but on the other hand, nucleoside reverse transcriptase reverse inhibitors (NRTIs) and protease inhibitors (PIs), which are part of HAART, are known to increase the risk of neuropathy. 10,11,22 Age has also been reported to be associated with HIV-related neuropathy. 21
To quantify the burden of HIV-related neuropathy at a population level it is essential to assess incidence and prevalence. 25 However, given the complexity of HIV-related neuropathy and the lack of consensus on diagnostic criteria, the epidemiology of the disease is unclear. The objective of the present study was to perform a systematic literature review to identify and summarize the incidence and prevalence estimates of neuropathy among HIV-infected patients.
Materials and Methods
Literature data sources and search strategy
To identify relevant studies regarding the epidemiology of HIV-related neuropathy, a systematic search of the literature was conducted using MEDLINE and EMBASE databases. The search was performed with keywords pertaining to the study population (human immunodeficiency virus or HIV or AIDS), study condition (neuropathy or neuropathic pain or paresthesia or numbness or tingling or sensitivity), and study design and outcomes (epidemiology or incidence or risk or prevalence or population). The relevance of each citation identified from the databases was based on title and abstract according to a predefined selection criteria: patients who are HIV or AIDS positive (population); cross-sectional and cohort studies (study design); and cumulative incidence, incidence rate, or prevalence of neuropathy (outcomes measures). For the abstracts that met these criteria, publications were obtained if available. Based on these full text reports, each study was evaluated for inclusion based on the selection criteria. The reference lists of identified publications were searched for pertinent literature as well.
Outcomes and data extraction
For each selected study, prevalence and incidence data were extracted. Any study that reported the number of subjects with neuropathy among HIV-positive patients at any point in time was considered for prevalence estimates, calculated as the percentage of cases out of all patients along with the 95% confidence interval (95% CI). Studies for which the population was at risk of neuropathy at baseline (i.e., did not have neuropathy) were not considered for prevalence estimates. These studies reported the occurrence of new cases of neuropathy and were used for incidence estimates. Cumulative incidence of neuropathy was calculated as the new number of cases out of the population at risk at baseline. Since cumulative incidence is a function of the duration of follow-up, which varies by study, the incidence rate of neuropathy was presented to facilitate comparisons across studies. The incidence rate is the number of cases per (100) person-year(s) and was calculated as the number of new cases divided by the total person-years at risk in that study. Corresponding 95% CI were calculated as well. For studies with a dynamic population, a cumulative incidence cannot be calculated and only the incidence rates were calculated.
If sufficient data were available in the included studies, prevalence and/or incidence estimates were presented for different subgroups of HIV patients. Subgroups of interest were not prespecified but reported as available in the included studies. If possible, the differences in the prevalence of neuropathy by subgroup within a study were expressed with the odds ratio (OR) along with a 95% CI. For incidence estimates, relative risk (RR) estimates or the hazard ratio (HR) were presented.
Apart from prevalence and incidence estimates information on design, study population patient characteristics, assessment of neuropathy, and type of neuropathy were extracted and recorded in evidence tables.
Results
Study selection
The literature search identified 1331 abstracts and 27 additional references from manual searches on reference list of reviews and other studies. The first review of abstracts excluded 1298 of the potentially relevant studies, of which 442 were excluded for studying a non-HIV population, 266 for not reporting data regarding prevalence or incidence, and the remaining abstracts excluded did not consider the reporting of a specific study. The full-text review of the 60 remaining studies excluded 23 of them, primarily because they did not provide data regarding the outcomes of interest. Thirty-seven studies were included in the review. The full text was not available for Villelabeitia et al. but the abstract contained epidemiologic estimates and was therefore included in the systematic review. 26 More detailed information is provided as a flow diagram in Fig. 1.
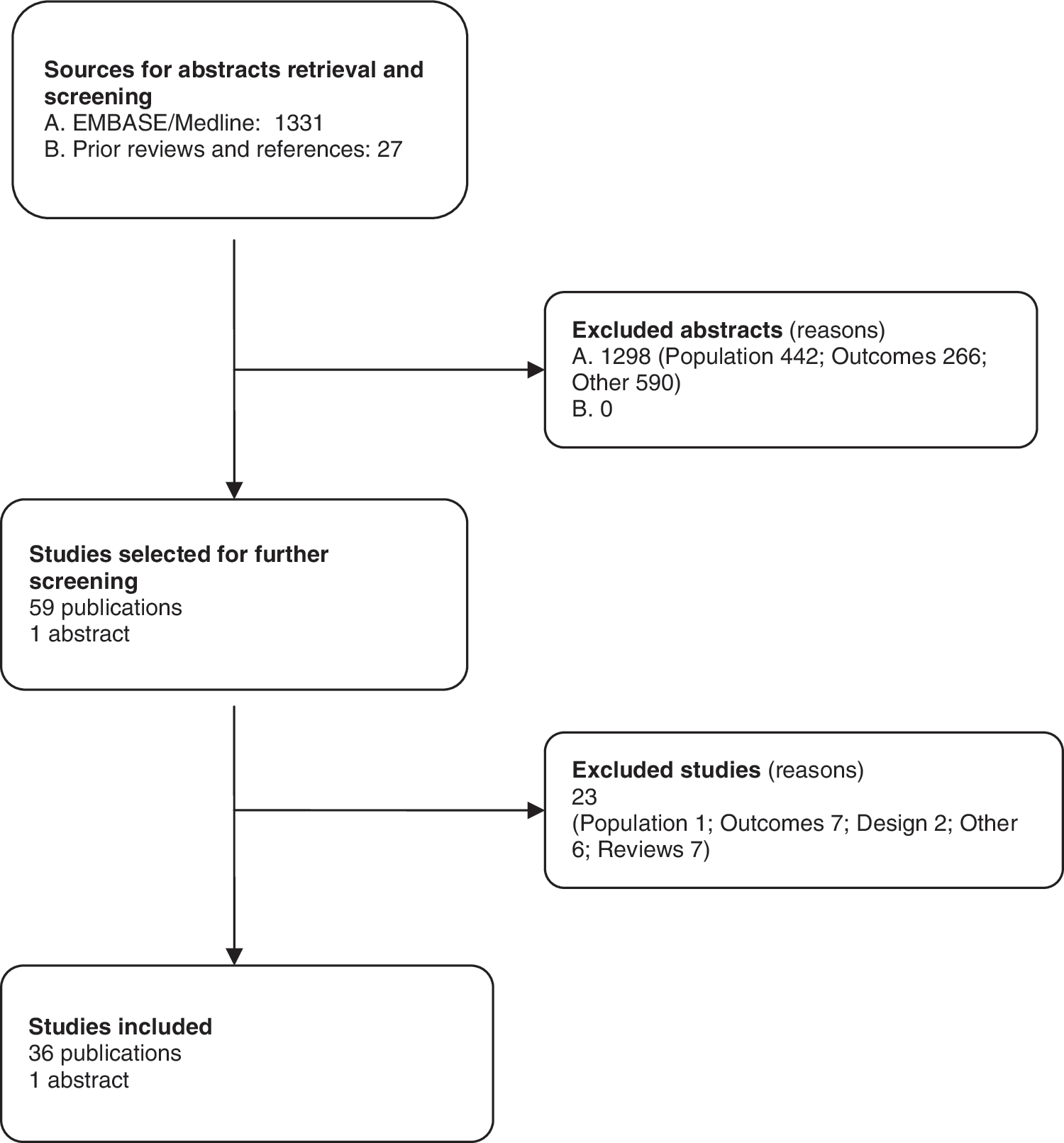
Flow diagram. The stages of study selection for systematic review.
Study characteristics
In Table S1 the principal characteristics of the selected studies are presented [for further information, see Supplementary Table S1 (Supplementary Data are available online at
Methods used to assess neuropathy included neurological examination in 18 studies, 6,18,21,22,24,26,27,29,30,32,34,35,38,46,48,50,51,54 a symptoms-based screening in seven studies, 39 –41,47,49,55,56 and the BPNS instrument in seven studies, 6,21,33,42,44,52,53 and in five studies medical records were used to identify neuropathy cases based on different case definition. 23,31,36,37,45 Beadles et al. 45 identified cases based on prescription of amitriptyline or zidovudine and reporting of pain/numbness in records; Lichtenstein et al. 37 used keywords “pain, tingling, or numbness in hand and/or feet” due to treatment, HIV, or for unknown reasons to identify relevant cases. Sheth et al. 23 used “painful sensory neuropathy,” “inflammatory demyelinating neuropathy,” “mononeuropathy multiplex,” “toxic neuropathy,” “diabetic neuropathy,” or “other HIV neuropathy” as key words. Buchacz et al. 31 selected cases based on reasons for hospitalization.
Patient characteristics
The characteristics of the patients included in the studies are summarized in Supplementary Table S2. The average age of patients among studies ranged from 28 to 47 years. The study populations were 2–49% female. Viral load varied between 1.7 and 5.2 log copies/ml (range of means across studies). CD4 count reported in the studies fell between 28 and 694 cells/mm3 (range of means across studies). The fraction of patients with AIDS ranged from 36% to 58%. The studies conducted in the post-HAART era had more than 50% of participants taking HAART. In the studies, treatment with NRTIs was reported as single use or in combination, either in the past or during the study, and ranged from 4% to 100% of the HIV patients. Smyth et al. explicitly determined that more than 50% were on PIs, who were on some kind of antiretroviral therapy at any time during their disease. 52 In a study in Thailand, Sithinamsuwan et al. reported that 97% of the HIV patients were on three drug combination ARV. 53
Prevalence of neuropathy among HIV-positive patients
Twenty-five studies provided estimates of the prevalence of neuropathy among HIV-positive patients, as summarized in Table 1. There was great variation across studies, with the lowest estimate being 1.2% and the highest estimate being 69.4%. Four studies reported estimates of less than 10%, six studies reported a prevalence of 10–30%, eight studies reported a prevalence of 31–50%, and seven studies reported prevalence estimates >50%. 21,23,24,27,29,30,32,37 –42,44 –55 Two studies, Morgello et al. and Pettersen et al., specifically reported antiretroviral toxicity-induced neuropathy (ATN) at 8.0% and 16.7%, respectively. 48,51
Numbers in parentheses are reference numbers.
The study by Barohn et al. (1993) was conducted on healthy U.S. Air Force personnel.
Gluck et al. did not report the number of AIDS patients nor the neuropathy cases among those patients.
The study by Matthews et al. (2000) used a questionnaire-based neuropathy screening.
BPNS, brief peripheral neuropathy screen; ANP, autonomic neuropathy; DSP, distal sensory neuropathy. U.S. Centers for Disease Control and Prevention (CDC) classification system of HIV-related conditions: CDC A, asymptomatic, acute HIV, or persistent generalized lymphadenopathy; CDC B, symptomatic conditions, not A or C; CDC C, AIDS-indicator conditions.
As illustrated in Fig. 2, when studies were stratified by geographic region, no clear pattern appeared, except that rates observed in Africa were greater than rates observed in Asia. The variation in prevalence among studies within a particular geographic region was greater than the variation in prevalence across regions. The prevalence in the U.S.-based studies varied from 1.5% and 62.0%, with four studies reporting estimates of less than 10%, five studies reporting a prevalence of 10–50%, and three studies reporting estimates greater than 50%. 23,27,29,37 –42,47,48,55 The prevalence of neuropathy among studies conducted in Europe ranged from 14.8% to 59.6%, and was less than 15% in two studies and greater than 50% in one study. 24,30,46 The studies conducted in Australia reported estimates of 34% and 63%. 32,52 The prevalence in Africa was reported to be 46.6% and 66.0%, 45,50 in Southeast Asia 10.0% and 34.4%, 44,53 and in Brazil 69.4%. 54
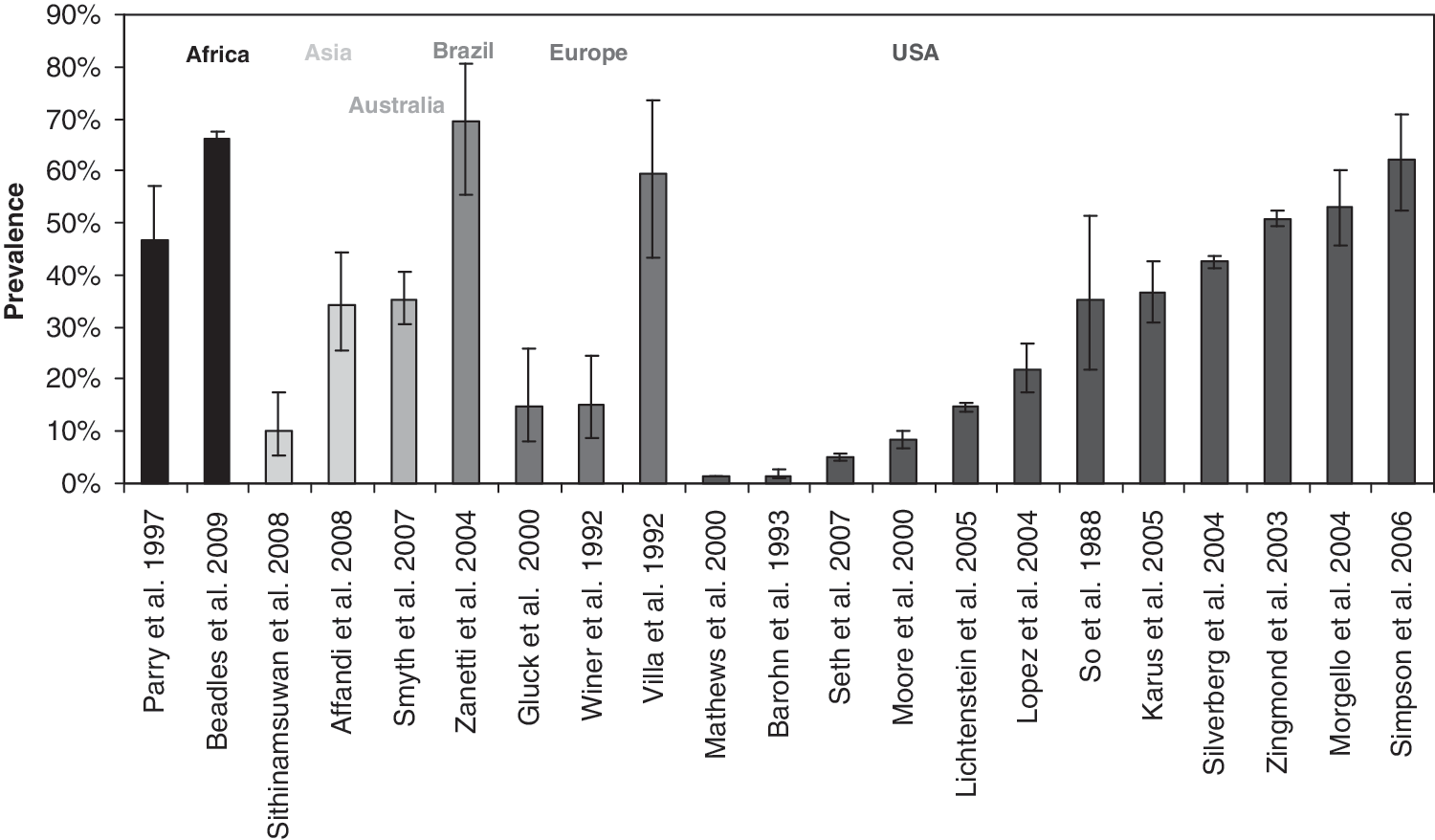
Neuropathy prevalence by region.
In Fig. 3 the prevalence estimates stratified by neuropathy assessment method are presented. It is obvious that there is variation in prevalence estimates as assessed by BPNS, symptoms, as well as neurological examination. Despite the variations within each assessment method, prevalence estimates obtained by neurological examination seem higher than those obtained with symptom-based assessments. Results for the BPNS seem to fall between these.

Neuropathy prevalence by methods of assessment.
The United States is the only country with studies that reported results for all of the above-mentioned methods of assessment (one study using BPNS, 42 four studies using neurological assessment, 27,29,38,48 five symptom-based studies, 39 –41,47,55 and two records 23,37 ). The BPNS-based study reported the highest prevalence estimates whereas the medical record-based study reported the lowest. Studies performed in Australia 21 and Asia 53 used the BPNS whereas studies performed in Europe relied on neurological assessment. 24,30,46 The studies performed in Africa used medical records 45 and neurological assessment, 50 with higher prevalence estimates reported by the former.
When studies were stratified by year of publication, the prevalence from studies conducted in the post-HAART era seemed comparable to prevalence estimated from studies in the pre-HAART era (see Fig. 4). Studies that allowed for the calculation of estimates among patients exposed to HAART as well as patients not exposed to HAART showed greater variation across studies than between exposed and nonexposed patients within studies. Among HAART-exposed patients, estimates ranged from 20.3% to 66.0%, and among nonexposed patients, prevalence estimates ranged from 5% to 52%. 23,26,38,41,48,52
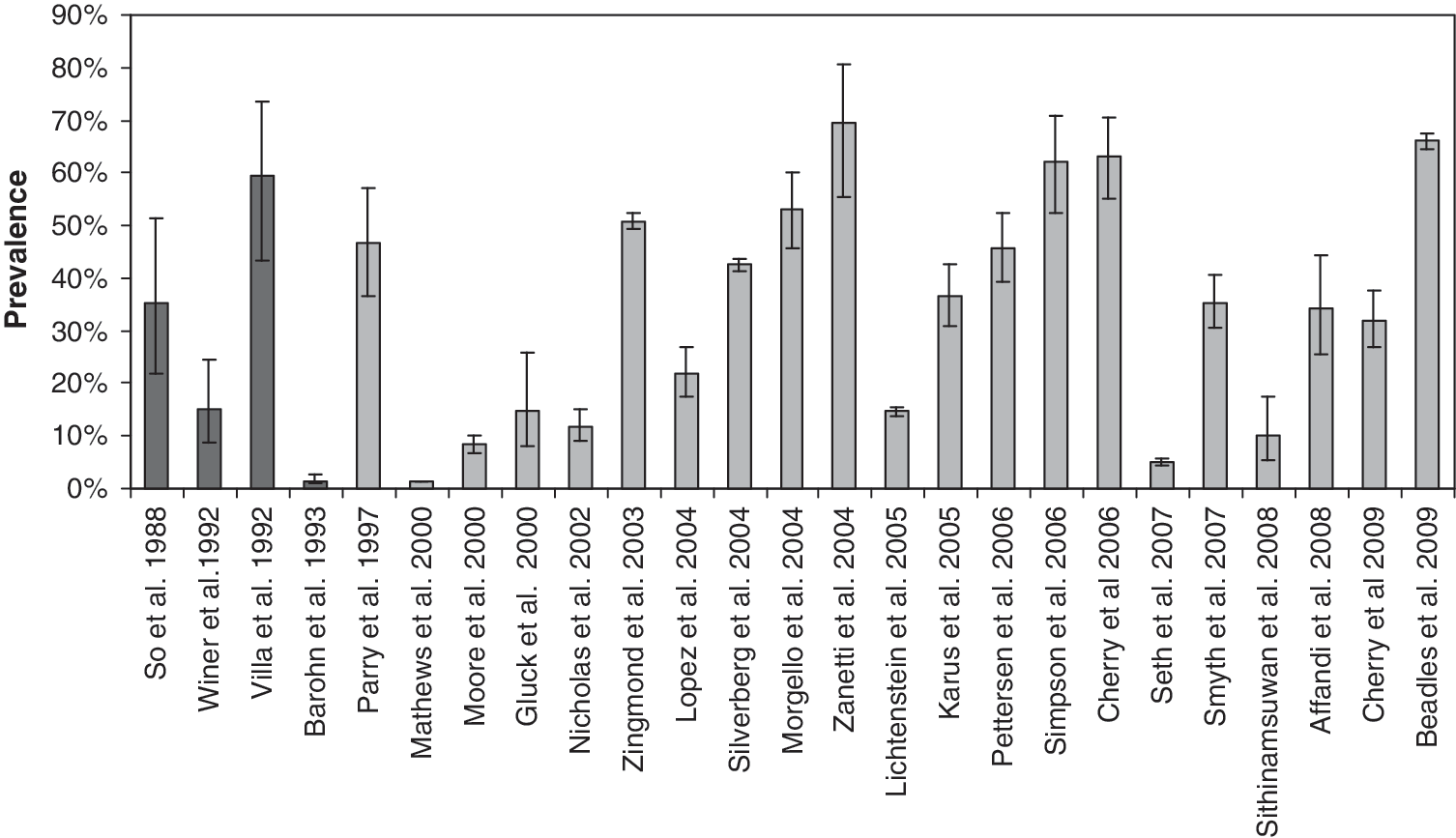
Neuropathy prevalence across studies conducted in the pre- and post-highly active antiretroviral therapy (HAART) era.
Overall, Barohn et al. 27 and Matthews et al. 39 reported the lowest prevalence estimates (1.5% and 1.25%, respectively). The population in Barohn et al. was composed of U.S. Air Force personnel who were screened for HIV infection while on active duty. This explains the low prevalence of neuropathy relative to other studies because patients with HIV were detected early in the course of disease. The retrospective study by Matthews et al. estimated the prevalence of symptoms based on a cost and service utilization questionnaire, which could have led to only severe neuropathy cases being detected, resulting in low estimates. The high prevalence estimates reported by Simpson et al. 42 and Zanetti et al. 54 (62.0% and 69.4%, respectively) might be partly explained by the fact that both studies not only evaluated for symptoms, but for subclinical nerve damage as well. However, from Fig. 3, it is obvious that this cannot totally explain the results. The high prevalence of 66.0% by Beadle et al. 45 could have been caused by their method of identifying neuropathy cases based on amitriptyline use and zidovudine use besides pain and/or numbness data. The high prevalence estimate of 63.2% reported in Cherry et al. 32 might be due to the high proportion (83%) of NRTI use and the fact that patients were recruited from hospitals. In Villa et al., 24 the occurrence of neuropathy was 59.4% with an odds ratio of 24.9 (95% CI 3–208), which can partly be explained by the fact that the study population was comprised of heroin users, among whom neuropathy-related symptoms can be common. The lowest odds ratio of 1.9 (95% CI 1.7–2.2) was reported by Silverberg et al. 41
Prevalence of neuropathy by subgroups
Severity of disease
Gluck et al. and Parry et al. 46,50 reported the prevalence of neuropathy by disease severity according to the U.S. Centers for Disease Control and Prevention (CDC) classification system of HIV-related conditions (CDC A: Asymptomatic, Acute HIV, or persistent generalized lymphadenopathy; CDC B: Symptomatic Conditions, not A or C; CDC C: AIDS-Indicator Conditions). 5 The two estimates of the prevalence of neuropathy among HIV patients classified as CDC A were 0.0% and 17.1%. For CDC B patients, the estimates were 17.6% and 60.8% (Table 1). For CDC C patients the estimates were 30.0% and 70.0%. According to Gluck et al., the prevalence odds ratios for neuropathy in CDC B and CDC C relative to CDC A were 3.1 (95% CI 0.3–36.9) and 9.7 (95% CI 1.1–90.7), respectively. 46 The corresponding odds ratios reported by Parry et al. were 7.5 (95% CI 2.2–25.3) and 11.3 (95% CI 3.4–36.5), respectively. 50 Despite this pattern of increasing prevalence of neuropathy among patients with more severe HIV disease status, the difference in results between the studies by Parry et al., performed in Africa, and Gluck et al., performed in Germany, is substantial. A possible explanation for the greater estimates reported by Parry and colleagues is that the more elaborate and arguably more sensitive neurological examination was used, which may have helped to detect asymptomatic neuropathy.
Four studies 21,38,46,52 reported a neuropathy prevalence of about 30% among patients with AIDS (Table 1). The study by Isezuo et al. reported a low prevalence of 2%, which might be due to the compromised quality of hospital records in Nigeria for case identification. 36 Smyth et al. reported the greatest prevalence with 45.2%. 52 Of the four studies that compared the prevalence of neuropathy among patients with and without AIDS symptoms, Lopez et al. and Gluck et al. reported a greater prevalence of neuropathy among those with AIDS, whereas Cherry et al. and Smyth et al. reported similar estimates. 21,38,46,52 It is interesting to note that the studies with similar results between patients with and without AIDS used the BPNS, whereas those with a difference used a neurological examination. The corresponding ORs varied between 0.8 (95% CI 0.5–1.3) 21 and 3.9 (95% CI 1.9–8.2). 38
Age
According to the study by Zingmond et al., which was conducted in the United States, older patients (>50 years) were more likely to experience neuropathy (58.8%) than younger patients (<50 years; 49.4%) 55 (Table 1). The corresponding OR was 1.5 (95% CI 1.2–1.7). The study by Cherry et al., a multinational study conducted in Jakarta, Kuala Lumpur, and Melbourne, compared >40 versus <40 years of age group and observed an OR of 2.8 (95% CI 1.2–6.4). 21 The differences between Cherry et al. and Zingmond et al. might be caused by study population characteristics and the diagnostic criteria used. The study by Cherry et al. included HIV patients from teaching hospitals using the BPNS, whereas the study by Zingmond et al. was conducted among U.S. veterans using reported symptoms to assess the prevalence of neuropathy, thereby probably underestimating the contrast.
Antiretroviral therapy
The studies that report prevalence estimates by exposure to PI and/or NRTI show great variation. In fact, the variation across studies is greater than the difference in neuropathy among exposed and nonexposed patients within studies. Prevalence estimates of neuropathy among populations exposed to any NRTI ranged from 20% to 49% 38,46,52,56 and from 5.0% to 40.5% among NRTI nonexposed patients. 38,46,52 The prevalence among PI-exposed patients ranged from 17.8% to 53.9%, whereas the prevalence among nonexposed patients was reported as 22.8% and 35.5%. 38,52
Incidence of neuropathy among HIV-positive patients
The incidence rate of neuropathy among HIV patients reported in 11 studies is summarized in Table 2. Results were not consistent across studies and the incidence rate varied between 0.7 and 39.7 per 100 person-years. 31,42 Seven studies reported an incidence rate of less than 5 per 100 person-years, and four studies reported an incidence rate greater than 20 per 100 person-years. 6,18,22,24,30,31,33,34,38,42,43 Only one study reported a relative risk of 2.9 (95% CI 0.1–219.5). 30 Childs et al. reported an ATN incidence of 0.2 per 100 person-years. 34
Numbers in parentheses are reference numbers.
Lichtenstein et al. (2005) reported the incidence rate only, without the number of neuropathy events that occurred during the follow-up period.
HAART+, exposure to HAART; HAART–, no exposure to HAART; ANP, autonomic neuropathy; DSP, distal sensory neuropathy; NRTI–, data are missing in the selected studies.
When studies were stratified by geographic region, no clear pattern appeared. The variation in incidence across studies within a particular geographic region was greater than the variation in incidence across regions (Fig. 5). The incidence rates reported in the U.S.-based studies varied between 0.7 and 39.7 cases per 100 person-years, with three studies having rates of less than 10 per 100 person-years, rates between 10 and 30 per 100 person-years in three other studies, and one study reporting a rate greater than 30 cases per 100 person-years. 6,18,22,31,34,38,42 The three studies conducted in Europe reported incidence rates ranging from 4.7 to 9.3 per 100 person-years. 24,30,43 The study conducted in Australia reported an incidence rate of 4.7 per 100 person-years. 33 Stratification of studies by pre- and post-HAART era seems to suggest a greater reported neuropathy incidence in the post-HAART era (Fig. 6).

Neuropathy risk by region.

Neuropathy risk across studies conducted in the pre- and post-HAART era.
Incidence of neuropathy by subgroups
Severity of disease
It is interesting to compare the risk of neuropathy by HIV severity stage given the fact that it is believed that DPS is immune-mediated. According to Lopez et al., the incidence rate of neuropathy among patients with AIDS was 24.8 per 100 person-years, as compared to 10.0 per 100 person-years among patients without AIDS. 38 In this study, the AIDS and non-AIDS subgroups were comparable in terms of demographics, but no information was provided on treatment history. However, it can be assumed that the AIDS subgroup had a longer history of treatment and arguably more exposure to different drugs because AIDS is the final stage of HIV. This illustrates the difficulty of disentangling the effect of HIV severity and HAART on the risk of neuropathy. The corresponding RR was 1.1 (95% CI 1.0–1.1). The HR as reported by Matthews et al. was 1.1 (95% CI 0.7–1.7) as well. 39
Age
The relative risks of neuropathy among HIV patients of older age (>40 years) versus younger (<40 years) were 1.1 (95% CI 1.1–1.2) and 1.3 (95% CI 0.9–1.9) according to Lopez et al. and Moore et al., respectively. 38,40 This comparable result was observed despite differences in the methods of assessment, which were neurological examination and symptom-based assessment, respectively.
Antiretroviral therapy
The incidence rate of neuropathy among HAART users across five studies ranged from 0.5 to 40.0 per 100 person-years, 18,26,31,37,43 whereas the incidence rate among non-HAART users reported in two studies were 1.7 and 25.0 per 100 person-years. 31,37 The incidence rate of neuropathy among NRTI users varied from 0.9 to 10.5 per 100 person-years across four studies. 33 –35,40,43 No data were identified that reported neuropathy risk explicitly for non-NRTI use (Table 1).
Lichtenstein et al. 37 used medical chart evaluation for neuropathy identification, which might have resulted in lower incidence estimates (5.0 per 100 person-years). For Buchacz et al. 31 the incidence estimation was low (0.5 per 100 person-years) because neurological disorder-related hospitalization rate was considered as a proxy for neuropathy development. The relatively high incidence of neuropathy among HAART users reported by Shiffito et al. 18 (40.0 per 100 person-years) might be explained by the fact that some of the patients developing neuropathy when on HAART might have already been experiencing subclinical neuropathy at baseline. It is interesting to note that this estimate is greater than the risk of neuropathy among AIDS patients as reported by Lopez et al. 24 (eight per 100 person-years), 38 which can be explained by the population at risk to develop neuropathy. Many patients with AIDS might already experience neuropathy symptoms, which excludes them from the at risk population for that particular study, thereby resulting in a lower incidence estimates.
In Zehender et al. 43 patients were considered neuropathy cases only if they reported persistent symptoms, which were confirmed by EMG, which led to a smaller estimate (1.9 per 100 person-years). Cherry et al. 33 (2.1 per 100 person-years) and Childs et al. 34 (0.9 per 100 person-years) probably reported a low incidence rate because many patients were already NRTI users, and the study populations might reflect a selection of subjects less prone to neuropathy development; NRTI patients experiencing neuropathy were not part of the at-risk population in these studies. It has been argued that neuropathy risk is in particular the greatest within the first few months of NRTI use; in fact, Lichtenstein et al. reported that neuropathy risk was the greatest during the first year of treatment, irrespective of HAART regimen. 37 Hence, this selection of subjects can explain the lower risk estimate by Cherry et al. 33 and Childs et al. 34
Discussion
A systematic literature review of studies providing information on the incidence and prevalence of neuropathy among HIV patients suggests there is a significant burden, but there is much variation across these studies. In addition to the estimation of the overall incidence and prevalence of DSP, the occurrence and risk of neuropathy were estimated for different age groups, HIV disease states, and antiviral treatment.
Although data regarding study and patient characteristics were collected from the included studies as much as possible, explaining differences in estimates and conflicting results across studies based on these characteristics fell short due to the studies' methodological problems and failure to take into account the etiology of HIV-related neuropathy.
In the included studies, neuropathy cases were identified by means of symptoms reporting, neurological examination, BPNS, or medical record review. The BPNS was developed to assess symptoms of DSP for HIV patients, specifically, pain, aching or burning, pins and needles sensations, and numbness in the feet and legs. The patient-completed screener asks patients to respond using a numeric rating scale (NRS), ranging from 0 to 10, with a recall period of “current.” The BPNS also includes a clinical examination to assess the patient's symptoms, perception of vibration, and deep tendon reflexes. It has been validated against objective measures, including both thermal threshold testing and epidermal nerve-fiber density. The BPNS has a relatively low sensitivity (34.9%) and high specificity (89.5%) for the diagnosis of DSP. 42 Hence, the BPNS cannot replace a careful clinical assessment of an HIV-infected patient presenting with neuropathic symptoms or signs. However, it can be considered a valid research tool that takes only minutes to administer and requires no specialized equipment. 15 Identification of cases based on symptoms reported in medical records should be considered the least reliable approach. As such, neuropathy estimates based on medical record review should be interpreted with caution. In addition to the identification of neuropathy cases based on signs and symptoms, the use of particular medication for neuropathy (e.g., amitriptyline), use of particular NRTIs (e.g., zidovudine), and neuropathy-related hospitalization were used to define cases.
To the extent it was possible to explain variation in the epidemiology estimates across studies, one of the primary reasons for variation seems to lie with the choice of assessment method used to identify and classify neuropathy cases. Since HIV-related neuropathy may be subclinical before it becomes symptomatic, diagnosis based on clinical aspects of the disease will fail to identify the cases with asymptomatic nerve damage, whereas diagnostic tests might detect subclinical nerve damage along with symptomatic neuropathies. This has an impact on both prevalence and incidence estimates. For prevalence studies, it is obvious that a method to detect subclinical neuropathy, such as neurological evaluation, will result in greater estimates than methods relying on reporting of symptoms alone. Accordingly, relying on a subclinical definition of neuropathy results in overestimation of the disease burden compared to a symptomatic approach. For incidence studies, the impact is less clear.
To estimate the incidence of neuropathy, the patient population should be free of neuropathy at baseline, or at inclusion in the study. When symptom assessment is used to identify cases, only HIV patients free of clinical neuropathy are included in the incidence study. Hence, the population at baseline can consist of both subclinical neuropathy cases and patients completely free of neuropathy. The subclinical neuropathy patients might develop clinical neuropathy faster than patients completely free of neuropathy at baseline. When a neurological examination is used to identify cases, only patients free of neuropathy will be included at baseline; however, at follow-up, both asymptomatic and symptomatic neuropathy will be identified, which might, in principle, result in more cases than a symptomatic definition, but given the less severe population at baseline, fewer patients might develop neuropathy along the duration of the study.
In light of this discussion, it is interesting to note that Schifitto et al. 18 reported that 42% of patients who were not symptomatic at baseline developed symptoms over a 1-year period. The corresponding symptomatic DSP incidence was 21%. In comparison, the incidence of DSP (asymptomatic and symptomatic) was 40%. Similarly, Simpson et al. 42 observed a transition from no neuropathy to both subclinical and symptomatic stages of 14% and 21%, respectively, among 28 patients. No transition was observed from subclinical to symptomatic stages.
When no distinction is made between neuropathy due to drug toxicity and virus-related neuropathy, the prevalence estimates of those studies might be greater than reported in studies that include only virus-related neuropathy. For incidence studies, this distinction does not necessarily increase the risk because it depends on the population at risk at baseline, whether these include patients free of clinical or subclinical neuropathy, either caused by HIV, ARV, or both. Of the included studies, only Childs et al., Morgello et al., and Pettersen et al. distinguished between HIV and drug-related neuropathy. 34,48,51 The lack of a standard definition of neuropathy has obviously limited the comparability and interpretation of the findings.
Other limitations in the identified studies are the lack of well-defined criteria for exclusion of patients who were at risk of neuropathy due to alcoholism, vitamin B12 deficiency, pyridoxine or thiamine, concomitant therapy with neurotoxic drugs (isoniazid, vincristine, dapsone), or with other systemic medical conditions (e.g., diabetes mellitus). Furthermore, the drop out rate, which ranged from 1.8% to 36.4%, can affect the validity of the estimates.
Despite the obvious limitations in the evidence, it is certain that HIV-positive patients might be at risk of neuropathy at some point. More specifically, the data seem to support the premise that older patients and those with advanced stages of HIV infection experience DSP. Current understanding of the etiology of neuropathies among HIV-positive patients is that some degree of (subclinical) neuropathy is universal among HIV-infected patients and neuropathy develops gradually with progression of HIV disease. 6 Clinical neuropathy is common among patients with AIDS due to lower CD4 counts. Patients with AIDS are less responsive to antiretroviral agents, thereby increasing the risk of virus-related neuropathy. Antiretroviral agents in turn are neurotoxic because of inhibition of mitochondrial DNA polymerase. 59,60 Patients with advanced stages of disease and older age typically have greater history and exposure to neurotoxic drugs, thereby increasing their risk of ATN. A few studies also looked into gender and neuropathy. Pettersen et al. 51 and Smyth et al. 52 did not find any significant differences in prevalence between men and women. In terms of incidence, Cherry et al. 33 and Hulgan et al. 56 indicated that men are at slightly greater risk than women. It is of interest to note the greater average neuropathy prevalence in African studies compared to Asian studies, which is in line with the recent findings by Cherry et al. who observed that black race is an independent risk factor for HIV-related neuropathy. 61
The identified studies did not suggest any difference in the prevalence of neuropathy before and after the introduction of HAART. On one hand, it can be argued that any real change in the true prevalence of neuropathy due to the availability of HAART cannot be observed and is overshadowed by the great heterogeneity across studies. On the other hand, it is possible to argue that the prevalence of neuropathy at a population level is not changed by the introduction of HAART because (virus-related) neuropathy (and other symptoms associated with severe stages of HIV and AIDS) is simply postponed in the post-HAART era. The primary benefit of HAART is increased longevity; however, at some point the treatment regimen will fail, and patients will progress to advanced HIV stages (including AIDS) and are at increased risk of virus-related neuropathy. A comparison of the incidence estimates of pre-HAART versus post-HAART studies suggested greater risk estimates in the post-HAART studies, but as discussed above, comparisons of results across incidence studies are difficult to make, given differences in case definition and identification methods, among others.
Although several studies allowed for the calculation of the prevalence or incidence of neuropathy among subgroups of patients exposed to any HAART, NRTI, or PI, comparisons of these calculated neuropathy estimates among exposed versus nonexposed populations can be affected by confounding bias due to other differences between the exposed and nonexposed populations within studies. Furthermore, different HAART regimens are associated with different neuropathy risks, 10,11,51,57,58 further complicating any interpretation of observed differences in neuropathy among subgroups with differences in exposure to PIs and NRTIs.
This review identified a significant “evidence gap” in the current literature, supporting our concern that the complexity of HIV-related neuropathy poses a challenge to researchers in robust epidemiological estimation of prevalence and incidence of the disease. Hence, calculation of the patient and economic burden at a population level based on current epidemiology data will have a considerable amount of uncertainty. With the methodological limitations in mind, a future study that intends to investigate the epidemiology of neuropathy requires a longitudinal design with a clear rationale for adopting an assessment method to identify asymptomatic, symptomatic, or both neuropathic states. Of course such a study needs a sufficient sample size and use of a validated instrument for epidemiologic research to measure neuropathy. A sufficient follow-up period with repeated measures regarding exposure to HAART (and which combinations of ARV), CD4 count over time, and neuropathy symptoms is required to capture the transitions between neuropathic states and to examine the relative impact of HAART exposure and HIV severity.
In conclusion, currently available studies providing information on the incidence and prevalence of neuropathy among HIV patients suggest a significant burden, but there is great variation in results across studies. Prevalence estimates of less than 10% were reported, but also estimates of more than 50% without a clear pattern across countries. The incidence rate of neuropathy varies between less than 5 per 100 person-years to rates that are greater than 20 per 100 person-years. There is no definitive explanation for the variation; however, it underscores the fact that complexity of the disease, along with absence of standardized diagnostic criteria, has considerably influenced the methodologies and outcomes of the studies. Furthermore, the variation in the estimates across studies suggests that patients might be misdiagnosed or undiagnosed because the diverse etiologies and the lack of standardized diagnostic criteria confound a clinician's ability to discern the clinical presentation and cause of the HIV-related neuropathy. This study therefore highlights the presence of a significant gap in evidence studying HIV-related neuropathy and also underscores the need for standardized tools and further research to capture the true burden of HIV-related neuropathy.
Footnotes
Acknowledgments
This research was funded by Pfizer Inc. Mapi Values received funding from Pfizer in connection with the development and execution of both this article and the research it describes.
Author Disclosure Statement
This study was financially supported by Pfizer. Dr. Jansen is an employee of Mapi Values. Mr. Ghosh was an employee of Mapi Values at the time this research was conducted. Ms. Chandran is an employee of Pfizer and owns stock in Pfizer.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.