
Abstract
The GRACE (Gender, Race and Clinical Experience) trial enrolled treatment-experienced, HIV-1–infected patients, mainly women, in North America, to assess outcomes with a darunavir/ritonavir-based regimen, which could include etravirine (ETR). We present outcomes at week 48 for men and women receiving ETR. Virologic response (HIV-1 RNA <50 copies/ml) and safety were assessed; descriptive statistics are reported. To evaluate the independent contribution of ETR treatment, a post hoc analysis including a multivariate model assessed factors predictive of virologic response for the entire GRACE population (429 patients). Of 207 patients who received ETR (women, 57.5%; black or Hispanic, 81.7%), 71.4% of women and 79.5% of men completed the study. Week 48 virologic response rates in women and men (intent-to-treat population) were 58.0% and 61.4%, respectively. After censoring patients who discontinued treatment for reasons other than virologic failure, response rates were 79.3% and 73.0%, respectively. Overall, ETR was well tolerated. Women experienced more nausea (24.4% vs. 11.4%) and rash-related events (21.0% vs. 15.9%), but less diarrhea (15.1% vs. 21.6%), compared with men. Grade 3–4 hypertriglyceridemia was more common in men (9.3%) than women (1.1%). In total, 11 (9.2%) women and 7 (8.0%) men discontinued ETR due to adverse events. In the multivariate model of the entire GRACE population, ETR use was independently associated with improved virologic response. ETR is effective and well tolerated in treatment-experienced patients with HIV-1, with similar outcomes among women and men.
Introduction
E
The GRACE (Gender, Race and Clinical Experience) study was designed to enroll a high proportion of women, with study sites chosen to reflect the geographic distribution of women with HIV in the United States. The GRACE study assessed the efficacy and safety of darunavir/ritonavir (DRV/r; PREZISTA) 600/100 mg bid, along with an investigator-selected optimized background regimen (OBR). The OBR could include ETR (200 mg bid), which was not commercially available at the time of trial enrollment. Given the cautions and limitations surrounding the use of first-generation NNRTIs in women, 5,6 the limited data on ETR use in women, and the high proportion of women who received ETR as a component of their OBR in GRACE, we assessed efficacy, safety, and tolerability outcomes by sex in the subgroup of GRACE patients who received ETR.
Materials and Methods
Study design
GRACE was a 48-week, multicenter, open-label, phase 3b study conducted in 65 study sites primarily located across the United States (58 sites), with a small number of sites in Canada (four sites) and Puerto Rico (three sites). The study was conducted from October 6, 2006 to December 19, 2008. The GRACE study was designed to compare by sex the efficacy and safety of DRV/r 600/100 mg bid plus an investigator-selected OBR. Selection of the OBR was based on resistance testing (vircoTYPE HIV-1) and could consist of commercially available nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs) and NNRTIs. Study-provided antiretrovirals (ARVs) for possible use in the OBR included tenofovir (TDF), emtricitabine (FTC), the fixed-dose combination of TDF/FTC, and zidovudine. Etravirine (200 mg bid) was made available for use in the OBR at the discretion of the investigator if, in his or her judgment, it was needed to construct an effective treatment regimen. Modifications to the OBR were allowed only in the event of toxicity related to an adverse event (AE) or serious adverse event (SAE). In these cases, either a single within-class ARV substitution or temporary interruption of all ARVs was allowed. Study visits were conducted as described elsewhere. 7 During enrollment, the vircoTYPE HIV-1 resistance test used to select the OBR did not include ETR. This resulted in some patients with reduced susceptibility to ETR receiving the drug. Subsequently, at the time of data analysis, baseline samples were reanalyzed using an updated version of the vircoTYPE HIV-1 resistance test interpretation, which included ETR; these results were not available to the study sites. The data referenced in this article are those obtained from the updated analysis.
Patients
The GRACE study enrolled treatment-experienced adults aged 18 years or older, with plasma HIV-1 RNA 1000 copies/ml or greater, regardless of CD4+ count. Patients were required to have previously received protease inhibitor (PI)-based or NNRTI-based therapy for at least 12 weeks. Patients with interruption of prior treatment for a minimum of 4 weeks were also eligible for the trial. The complete list of inclusion and exclusion criteria for GRACE has been reported elsewhere. 7 This analysis assessed patients from the GRACE trial who received ETR during the study period.
Efficacy
This preplanned analysis assessed virologic response (HIV-1 RNA <50 copies/ml) to DRV/r-based therapy in male and female patients who also received ETR. Additional end points included change in CD4+ count from baseline to week 48, the proportion of patients with virologic failure (VF), and the number developing new resistance mutations. Virologic failure was defined as a viral load greater than 50 copies/ml from week 24 onward, measured by two consecutive assessments at least 14 days apart; a viral load greater than 50 copies/ml prior to week 24 was not considered to be VF. Genotype analysis was conducted at VF only in patients with plasma HIV-1 RNA greater than 1000 copies/ml.
Safety
Safety and tolerability, serum chemistries, and clinical laboratory test abnormalities were determined, as described previously for the overall GRACE study. 7 In addition to those AEs assessed for the overall GRACE population, AEs of specific interest to the ETR subgroup, including skin-associated, neuropsychiatric-associated, cardiac-associated, and hepatobiliary-associated AEs, were assessed.
Statistical methods
Virologic response is reported using the time-to-loss of virologic response (TLOVR) algorithm for the intent-to-treat (ITT) population, which includes all patients who took at least one dose of study medication, and the non-VF censored population, which censors patients who discontinued for reasons other than VF. Immunologic changes were analyzed using an observed case analysis and a mixed effects model that was constructed to evaluate CD4+ cell count change over time, using all available CD4+ cell count measurements. The mixed effect model assumed normality and included sex, log10 HIV RNA at baseline, CD4+ count at baseline, and race (black vs. nonblack) as the independent covariates. Statistical Analysis Software (SAS version 9.1, SAS Institute Inc., Cary, NC) was used for the statistical analyses. The ETR subgroup was not powered for comparisons by sex and, therefore, descriptive statistics are reported.
A post hoc analysis of the overall GRACE population was conducted in order to investigate factors that were predictive of virologic response (ITT–TLOVR). For this analysis, 43 covariates were evaluated in univariate assessments. Potential covariates included variables in the following groups: patient and disease characteristics, treatment factors, baseline resistance, site characteristics, and comorbidities (see Supplementary Table S1 for covariates and their univariate associations with response; Supplementary Data are available online at
Results
Patient disposition and baseline characteristics
Of the 429 patients enrolled in GRACE, 207 [119 (57.5%) women and 88 (42.5%) men] received at least one dose of ETR and were included in this subgroup analysis (Fig. 1). Of these 207 patients, 203 received ETR as a component of their OBR, as reported on study day 7, and four patients began ETR treatment after study initiation (two patients on day 8 and two on day 32). The majority of patients in the ETR subgroup were black or Hispanic women (Table 1). At baseline, the median CD4+ count was 187 cells/mm3 and the mean HIV-1 RNA was 4.6 log10 copies/ml. Men had slightly more advanced disease than women at baseline with lower median CD4+ counts and a higher prevalence of previous history of Centers for Disease Control and Prevention (CDC) Class C disease. At baseline, median ETR fold change and the mean phenotypic susceptibility score of the OBR were comparable for women and men (Table 1). In addition to all patients receiving DRV/r, the majority of patients in the ETR subgroup were receiving two NRTIs in their OBR (70.5%); 15.9% of patients received at least three NRTIs, while 8.2% and 5.3% of patients received one or no NRTI in their OBR, respectively.

Etravirine subgroup: study disposition. a“Other” classification was selected by the investigator as a reason for discontinuation and included one patient who was removed from the trial due to old age, one patient who discontinued due to no virologic response by week 12, one patient who was too busy to attend appointments, one patient whose primary care physician discontinued the study medication and started a new regimen, and two patients who were ineligible to continue.
Virco TYPE HIV-1 resistance analysis.
Genotypic score. 9
Includes ETR but not DRV.
SE, standard error; SD, standard deviation; CDC, U.S. Centers for Disease Control and Prevention; ETR, etravirine; DRV, darunavir; IAS, International AIDS Society; NNRTI, nonnucleoside reverse transcriptase inhibitor; RAM, resistance-associated mutation; PSS, phenotypic susceptibility score; OBR, optimized background regimen.
The overall discontinuation rate in the ETR subgroup was 25.1%: 34 (28.6%) women and 18 (20.5%) men discontinued the study. The primary reasons for study discontinuation in women and men in the ETR subgroup were AEs (7.6% of women and 4.5% of men) and lost to follow-up (6.7% of women and 3.4% of men; Fig. 1). Apart from nausea (1.4%), no single AE leading to trial discontinuation was reported in more than 1.0% of subjects in the ETR subpopulation.
Efficacy
At week 48 (ITT–TLOVR), 123 of 207 [59.4%; 95% confidence interval (CI): 52.7%, 66.1%] patients in the ETR subgroup achieved virologic response: 58.0% (95% CI: 49.1%, 66.9%) in women and 61.4% (95% CI: 51.2%, 71.5%) in men (Fig. 2). The response rate was higher in the non-VF censored population, with 123 of 161 (76.4%; 95% CI: 69.8%, 83.0%) patients achieving virologic response: 69 of 87 (79.3%; 95% CI: 70.8%, 87.8%) women and 54 of 74 (73.0%; 95% CI: 62.9%, 83.1%) men (Fig. 2). In a post hoc analysis of the ITT–TLOVR population from GRACE, response rates were lower for patients who did not receive ETR (47.7%; 95% CI: 41.2%, 54.3%) compared with patients who received ETR (59.4%; 95% CI: 52.7%, 66.1%). Similarly, in the non-VF censored population from GRACE, a smaller proportion of patients who did not receive ETR achieved virologic response (69.7%; 95% CI: 62.4%, 77.0%) compared with patients who received ETR (76.4%; 95% CI: 69.8%, 83.0%).
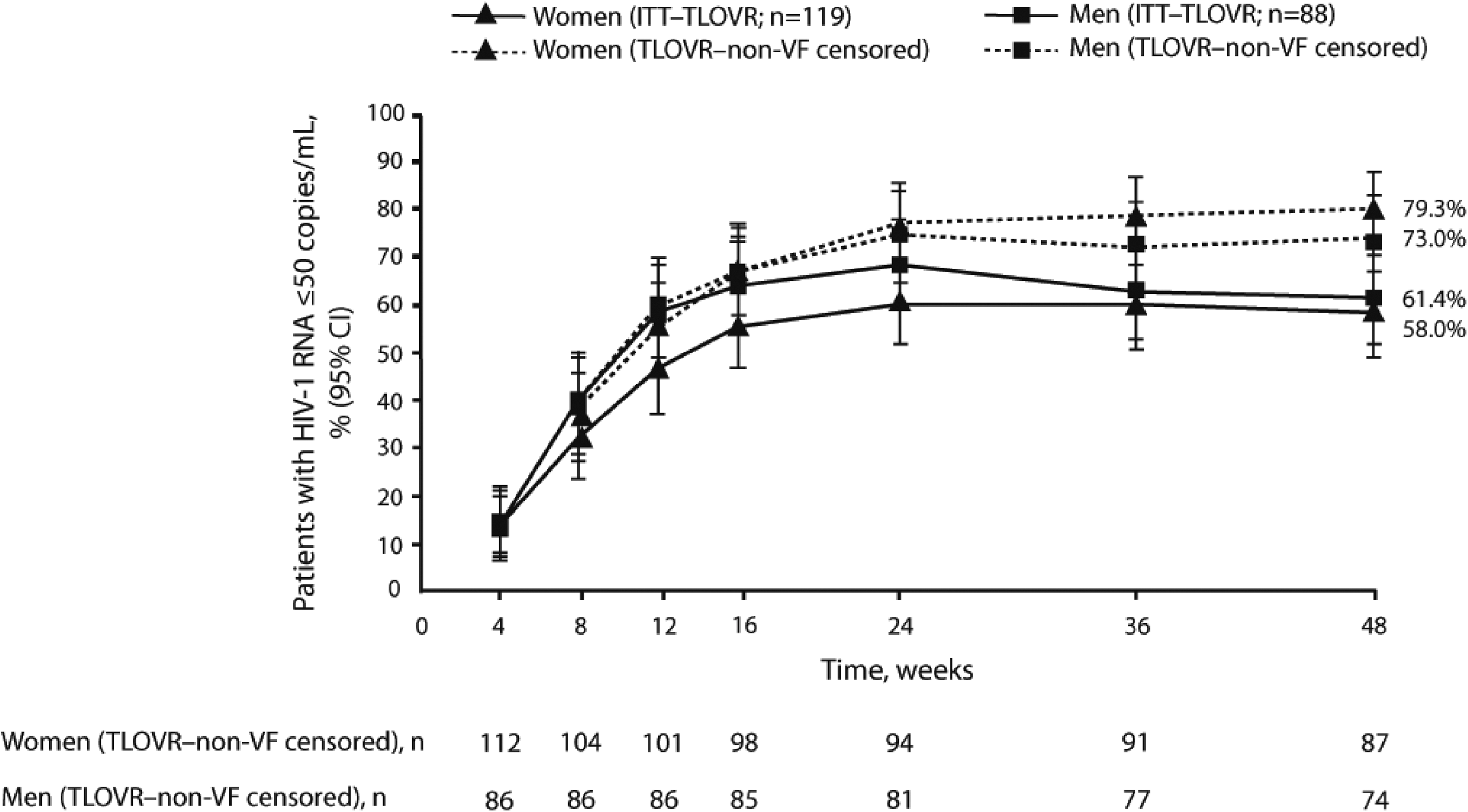
Etravirine subgroup: virologic response in the intent-to-treat and nonvirologic failure censored populations. ITT, intent-to-treat; TLOVR, time-to-loss of virologic response; VF, virologic failure; CI, confidence interval.
The mean [standard deviation (SD)] change in CD4+ count from baseline to week 48 in the observed analysis of the ETR population was +123 (134.0) cells/mm3; at week 48, the observed mean (SD) change in CD4+ count from baseline was +136 (141.6) cells/mm3 for women and +108 (123.7) cells/mm3 for men (Fig. 3). After adjusting for baseline log10 HIV RNA, baseline CD4+ count, and race, sex was not significantly associated with a change in CD4+ count from baseline. In a post hoc analysis, the observed mean (SD) change in CD4+ count from baseline to week 48 was slightly higher for patients who did not receive ETR [159.5 (153.3) cells/mm3] than for patients who did receive ETR [+123 (134.0) cells/mm3].

Etravirine subgroup: mean change from baseline over time in CD4+ count in the observed case analysis. CI, confidence interval.
In the post hoc multivariate analysis assessing correlation of virologic response (ITT–TLOVR) in the overall GRACE population (irrespective of ETR use, N=429) at week 48, ETR use in the OBR was significantly associated with an improved response rate in the final model (p=0.0424). 8 Other factors independently associated with improved virologic response in the final model were lower baseline viral load, nonblack race/ethnicity, older age, at least 95% adherence, lack of a gastrointestinal medical history, and participation at a trial site with limited clinical experience (Supplementary Table S2).
Resistance
Virologic response in the ETR subgroup decreased with increasing baseline ETR weighted genotypic score 9 ; higher virologic responses were observed in those patients with ETR scores of 0–2 (Table 2). Fifty-one (24.6%) patients [25 (21.0%) women and 26 (29.5%) men] experienced confirmed VF. Genotype analysis was conducted for 20 (39.2%) patients with plasma HIV-1 RNA greater than 1000 copies/ml at VF and an available baseline sample for comparison. Of these, six patients developed treatment-emergent ETR resistance-associated mutations [RAMs; V90I, L100I, K101P, V179F (n=2), Y181C (n=5), and Y181I], one patient developed a major International AIDS Society (IAS)-USA PI mutation (I50V), and one patient developed two DRV RAMs (I50V and L89V).
Genotypic score. 9
ETR, etravirine.
Safety
In the ETR subgroup, 186 (89.9%) patients [112 (94.1%) women and 74 (84.1%) men] reported at least one AE. The most frequently reported AEs of any grade were nausea, diarrhea, upper respiratory tract infection, cough, rash, and vomiting; nausea and vomiting were more commonly reported in women than men and diarrhea was more commonly reported in men than women (Table 3). In total, 11 (9.2%) women and 7 (8.0%) men prematurely discontinued ETR due to AEs.
Occurring in ≥10% of patients in either group.
Excludes laboratory abnormalities reported as AEs.
Occurring in ≥2% of patients in either group.
AE, adverse event; SAE, serious adverse event; ETR, etravirine; ALT, alanine transaminase; AST, aspartate aminotransferase.
Serious AEs were reported by 47 (22.7%) patients. The most common SAEs in the ETR subgroup were pneumonia (3.4%), which was more commonly reported in women than men, and Pneumocystis jiroveci pneumonia (2.4%), which was more commonly reported in men than women (Table 3); all other SAEs were reported in less than 2.0% of patients. Two deaths were reported in the ETR subgroup (pneumonia and lactic acidosis) and were considered not, or doubtfully, related to ETR.
Adverse events of any grade considered at least possibly related to ETR were experienced by 95 (45.9%) patients (Table 3). Grade 2–4 AEs considered at least possibly related to ETR were experienced by 29.5% of patients (n=61), with the most common being nausea (n=14; 6.8%), rash (n=8; 3.9%), and diarrhea (n=7; 3.4%) (Table 3). More women (n=41, 34.5%) experienced grade 2–4 AEs at least possibly related to ETR than men (n=20, 22.7%); nausea occurred much more commonly in women (n=12, 10.1%) than men (n=2, 2.3%).
Of the AEs of interest to the ETR subgroup, skin-associated events, which include rash, dermatitis, edema, and other similar events, were the most common and were reported by 50 (24.2%) patients; the overall incidence of rash-related events in the ETR subgroup (all grades/types), regardless of causality, was 21.0% (n=25) in women and 15.9% (n=14) in men, with a median onset of 16.0 days after first day of drug intake. Most rash-associated events were grade 1 or 2; grade 3 macular rash and grade 4 urticaria were reported in one patient each. Skin-associated events led to permanent discontinuation of ETR in five patients (women, n=3; men, n=2).
Neuropsychiatric-associated events occurred in 28 (23.5%) women and 17 (19.3%) men, with none leading to discontinuation of ETR. The most frequent neuropsychiatric-associated events were headache [8.7% overall (women, 9.2%; men, 8.0%)] and depression [5.3% overall (women, 5.0%; men, 5.7%)]. Hepatobiliary-associated events were less common in women (n=6, 5.0%) than men (n=11, 12.5%), with four leading to discontinuation of ETR. The most frequent hepatic events were increases in aspartate aminotransferase [4.3% overall (women, 2.5%; men, 6.8%)] and alanine aminotransferase [1.9% overall (women, 0.8%; men, 3.4%)]. Cardiac-associated events occurred in 11 (9.2%) women and six (6.8%) men, with one (myocardial infarction in a man; doubtfully related to the study drugs) leading to discontinuation of ETR. The most frequent cardiac-associated events, all doubtfully related to ETR, were angina pectoris [2.9% overall (women, 3.4%; men, 2.3%)] and cardiac murmur and myocardial infarction [both in 1.4% overall (women, 0.8%; men, 2.3%)].
Most laboratory abnormalities were mild to moderate in severity. No differences were observed in grade 3–4 laboratory abnormalities between sexes, with the exception of hypertriglyceridemia, which was more common in men (Table 3), despite more men (10.6%) being on lipid-lowering therapy than women (6.3%) at baseline. Only small changes over time were observed for mean lipid-associated laboratory parameters in the ETR subgroup, and the mean changes from baseline were similar between women and men.
Discussion
This preplanned subgroup analysis of GRACE assessed efficacy and safety outcomes in patients receiving ETR at the investigator's discretion, and has the largest population of ETR-treated women in any trial to date. A total of 119 women and 88 men constitute the study population for this analysis. Approximately twice the number of women received ETR in GRACE compared with the number of women who received ETR in the DUET trials, 1,2 providing an opportunity to expand the efficacy and safety data on ETR use in women. The ITT–TLOVR response rate in the ETR subgroup of GRACE (59.4%) was similar to that reported in treatment-experienced patients in the ETR treatment arms of the two phase 3 DUET studies at week 48 (pooled data, 61.0%). 10 Women in the ETR subgroup of GRACE had slightly lower response rates than men, most likely due to the higher number of women compared with men that discontinued the study for reasons other than VF. When patients discontinuing for reasons other than VF were censored, a slightly higher response rate was observed in women compared with men.
Patients in the ETR subgroup had slightly more advanced disease at baseline compared with the overall GRACE population: 42.0% of women and 50.0% of men had CDC Class C disease in the ETR subgroup compared with 35.5% and 47.2%, respectively, in the overall GRACE population. The mean CD4+ count was 208 cells/mm3 in the ETR subgroup compared with 219 cells/mm3 in the overall GRACE population. Additionally, a greater proportion of patients in the ETR subgroup had one or more baseline IAS-USA NRTI or NNRTI RAMs (65.2% and 69.1%) compared with the overall GRACE population (57.8% and 55.3%). 7 This may reflect selective use of ETR in the OBR for patients with increased resistance and more limited treatment options. Nonetheless, the virologic response rates for the ETR subgroup (ITT–TLOVR, 59.4%; TLOVR–non-VF censored, 76.4%) were slightly higher than those for the overall GRACE population (ITT–TLOVR, 53.4%; TLOVR–non-VF censored, 73.2%), 7 confirming that ETR is an effective therapeutic option for treatment-experienced patients. Additionally, when comparing patients from GRACE who received ETR with those who did not receive ETR, patients who received ETR had slightly higher response rates (ITT, 59.4% vs. 47.7%).
Indeed, the post hoc multivariate analysis revealed that inclusion of ETR in the OBR was significantly associated with improved virologic response in the overall GRACE population. Furthermore, the mean phenotypic susceptibility scores of the OBR, which include ETR, for women and men in the ETR subgroup [2.1 (0.07) and 2.0 (0.09), respectively] were comparable to those of the overall GRACE population [2.0 (0.04) and 2.0 (0.07), respectively]. 7 These data suggest that the higher response rates achieved in the ETR subgroup relative to the overall GRACE population may have been enhanced by the inclusion of ETR in the OBR and not due to the use of a greater number of active agents in the treatment regimen. The significant association of ETR use with improved virologic response suggests that ETR-containing regimens are highly effective in treatment-experienced patients.
In the observed values analysis, higher increases in CD4+ counts were seen in women compared with men in the ETR subgroup, as previously noted in the overall GRACE population and other studies of ARVs. 7,11 In the observed analysis, the mean change in CD4+ count for the ETR subgroup (+123 cells/mm3) was slightly lower than that of the overall GRACE population (+141 cells/mm3). Similarly, changes in CD4+ count were slightly lower for patients who received ETR compared with patients who did not receive ETR. Differences in baseline disease characteristics between the groups may have impacted immunologic responses, as patients in the ETR subgroup had slightly more advanced disease at baseline than the overall GRACE population. 7,12
Overall, ETR was well tolerated in both men and women. Minimal differences were observed between sexes with regard to the majority of AEs; however, nausea (regardless of severity or causality) was reported more commonly in women than men, while diarrhea and hypertriglyceridemia were reported more commonly in men than women. These findings were similar to the overall GRACE population and to results of other ARV trials. 7,13,14 In general, rates of AEs in the ETR subgroup were similar to those in the overall GRACE population, as well as those in the larger DUET studies, with the exception of rash. Within GRACE, rash of all grades/types, regardless of causality, was seen in more women in the ETR subgroup (21.0%) than women in the overall study population (15.3%), consistent with the findings in the DUET trials, which showed that women receiving ETR had a higher incidence of rash than those receiving placebo. 7 The incidence of rash among women in the GRACE ETR subgroup, however, was lower than that observed among ETR-treated women in the DUET pooled data at week 48 (30.0%). 15 The incidence of rash (all grades/types, regardless of causality) among men in the ETR subgroup, on the other hand, was similar to that observed among ETR-treated men in the DUET studies (15.9% vs. 18.0%, respectively). 15 While comparison of the DUET and GRACE studies is limited due to differences in patient demographics, particularly the proportion of women and the racial/ethnic breakdown, results from GRACE may help increase our understanding of rash as a side effect of ARV therapy. Specifically, with 119 women receiving ETR in GRACE relative to only 60 in DUET, results from GRACE may offer a more accurate estimation of the incidence of rash that can be expected with ETR use in women.
Overall, AEs were the most common cause of trial discontinuation, though no specific AE was identified as driving discontinuation. The discontinuation rate in the ETR subgroup (25.1%) was slightly lower than that seen in the overall GRACE population (29.6%), again suggesting that ETR treatment was well tolerated and not a specific cause of trial discontinuation. 7 Discontinuations in the ETR subgroup were slightly higher in women than men, mostly due to reasons such as AEs, lost to follow-up, and “other” investigator-defined reasons. Previous studies of ARVs have also noted a higher incidence of discontinuation due to AEs among women than men. 12,16
Patients receiving novel agents, such as T-20, are generally highly treatment-experienced “salvage” patients. Previous studies of “salvage” patients have shown that men in this population are much more treatment experienced, with more resistance, than women. 17 In this trial, the OBR was restricted to include only NRTIs and/or NNRTIs in an attempt to select more early treatment-experienced patients and avoid this imbalance. Despite this restriction, however, there were still slight gender-based imbalances in GRACE, which should be considered when interpreting the data: women were younger, had less treatment experience, and had fewer mutations at baseline than men.
General comparisons of the ETR population with the overall GRACE population and with the population of patients who did not receive ETR provide some context regarding the potential benefits of ETR use; however, interpretation is limited because use of ETR was not randomized. As noted, patients who received ETR had slightly more advanced disease than did the GRACE population as a whole. Nonetheless, the multivariate analysis reported here does account for some differences in baseline characteristics and, consequently, provides an appropriate representation of the impact of ETR use in combination with ritonavir-boosted DRV in GRACE.
The ETR subgroup in GRACE provides a representative sample of treatment-experienced women living with HIV in the United States, and also a higher proportion and total number of women than is typically seen in clinical trials of ARV agents. Results from this trial, therefore, expand on the limited data available on the use of ETR in women and simultaneously allow for sex-based comparisons. 10,18 Overall, this analysis of data from the GRACE study demonstrates that ETR is effective and well tolerated in treatment-experienced patients with HIV-1, with similar outcomes observed in women and men.
Footnotes
Acknowledgments
The authors would like to thank the study sites, the patients and their families, and the study investigators for their participation in the trial. The authors would like to acknowledge Gilead for supplying tenofovir, emtricitabine, and tenofovir/emtricitabine and thank the internal study support staff, as well as Cali Howitt, Ph.D., Medicus International New York, for her drafting and editorial assistance. David Anderson and Lori DeLaitsch of Tibotec Therapeutics Clinical Affairs reviewed and provided input on this manuscript. Funding for the GRACE study and editorial support was provided by Tibotec Therapeutics.
These data were previously presented at the 49th Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC), San Francisco, CA, September 12–15, 2009. Poster H-919.
Author Disclosure Statement
S.H. has acted as a consultant for and has received grant support from Janssen Global Services. D.J. has acted as a speaker for Johnson & Johnson, Gilead Pharmaceuticals, Merck, Boehringer Ingelheim Pharmaceuticals, Inc., Bristol-Myers Squibb, Virco, and GlaxoSmithKline; has received research support from Johnson & Johnson, Vertex Pharmaceuticals, and Pfizer; and has acted as a consultant for Johnson & Johnson, Bristol-Myers Squibb, Gilead Pharmaceuticals, Three Rivers Pharmaceuticals, and GlaxoSmithKline. J.M. and J.W. are full-time employees of Janssen Global Services. R.R. is a full-time employee of Janssen R&D.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.