
Abstract
The rate of virological failure was assessed in 386 adult patients attending the Centre National Hospitalier Universitaire of Bangui, the capital city of the Central African Republic (CAR), receiving their first-line antiretroviral (ARV) drug regimen for 24 months, according to the World Health Organization (WHO) recommendations. In addition, genotypic resistance testing was carried out in 45 of 145 randomly selected patients whose plasma HIV-1 RNA load was detectable. Overall, 28.5% of ARV-treated patients were in virological failure (e.g., HIV-1 RNA >3.7 log10 copies/ml). Twenty-four percent of patients in virological failure showed wild-type viruses, likely indicating poor adherence. Even after excluding the M184V mutation, all 76% of patients in virological failure displayed viruses harboring at least one major drug resistance mutation to nucleoside reverse transcriptase inhibitors (NRTI), non-NRTI, or protease inhibitors. Whereas the second-line regimen proposed by the 2010 WHO recommendations, including zidovudine, tenofovir, lopinavir, and atazanavir, could be effective in more than 90% of patients in virological failure with resistant viruses, the remaining patients showed genotypic profiles highly predictive of resistance to the usual WHO second-line regimen, including complex genotypic profiles diagnosed only by genotypic resistance tests in some patients. In conclusion, our observations highlight the high frequency of therapeutic failure in ARV-treated adults in this study, as well as the urgent and absolute need for improving viral load assessment in the CAR to prevent and/or, from now on, to monitor therapeutic failure.
Introduction
T
The high genetic diversity in HIV subtypes, comprising a high proportion of natural polymorphisms, among which certain positions are associated with resistance, increased the complexity in ARV therapy management in sub-Saharan Africa. 2,3 Recent data about the prevalence of resistance in Africa in HIV-infected adults described high rates of resistance: 83% in South Africa, 4 80% in Chad, 5 85% in Burkina Faso, 6 50% in Mali, 7 and 36% in Cameroon. 8 All studies related to ARV drug resistance in Africa pointed out the necessity in improving treatment adherence and biological monitoring, including an increase in access to viral load assessment with the aim of optimizing strategies for the use of ARV-containing regimens.
To our knowledge, ARV drug resistance in HIV-infected adult patients in the CAR has been reported in only very limited series. 9 In addition, a high level of HIV genetic diversity was described in the country. 9 –11 The aim of the present study was to assess the rate of virological failure and the selection of HIV-1 variants resistant to ARV drugs in adult patients followed up in Bangui, the capital city of the CAR.
Materials and Methods
Study patients and sampling processing
The so-called “Hôpital de Jour” was created on behalf of the French network GIP-ESTHER (“Groupement d'Intérêt Public-Ensemble pour une Solidarité Thérapeutique en Réseau”) in a partnership between the Centre National Hospitalier Universitaire of Bangui and the Centre Hospitalier Général of Brives-la-Gaillarde, France. The “Hôpital de Jour” constitutes an open health care center for ambulatory adults infected by HIV. The active file included in 2009 around 2500 patients, of which 850 were treated by ARV therapy according to the World Health Organization (WHO) 2006 revised recommendations for resource-poor settings. 12
All patients followed at the “Hôpital de Jour” were prospectively included between July 2009 and October 2009 on the basis of the following criteria: age more than 18 years old, signed informed consent, and ARV treatment for more than 6 months. For all patients, 1 EDTA blood sample was obtained for the measurement of HIV-1 plasma viral load and of CD4 T cell counts at the Pasteur Institute of Bangui, and one plasma aliquot was frozen at −30°C to be further transported in dry ice to the virology laboratory of the Hôpital Européen Georges Pompidou for possible genotypic resistance testing.
The study has been formally approved by the Scientific Committee of the Faculté des Sciences de la Santé (“FACSS”) of Bangui (so-called “Comité Scientifique Chargé de la Validation des Protocoles d'Etudes et des Résultats”/”CSCVPER”) (agreement UB/FACSS/CSCVPER/09), which constitutes the National Ethical Committee.
HIV-1 viral load and CD4 T cell count measurements
HIV-1 RNA viral load was performed by generic HIV-1 viral load (BioCentric, Bandol, France) using the Applied Biosystems 7500 real-time PCR system, as previously described. 13 The threshold of detection of the BioCentric assay is 300 copies/ml. 13 The CD4 T cell count was measured by flow cytometry using FACSCalibur (Becton Dickinson, San Jose, CA) and expressed in absolute count.
Genotypic resistance testing
A genotypic resistance test was carried out for a subgroup of HIV-treated patients whose HIV-1 RNA load was above 300 copies/ml. Genotypic analysis of reverse transcriptase (RT) and protease (PR) HIV genes was performed at the virology laboratory of Georges Pompidou European Hospital, Paris, France, with the commercial assay ViroSeq (Celera Diagnostics, CA) used on plasma samples. ARV drug resistance mutations were identified and interpreted according to the Agence Nationale de Recherches sur le SIDA et les hépatites virales (ANRS) algorithm, updated July 2009 (
Results
HIV-1 RNA viral load and CD4 T cell count in the study population
During the 4-month study inclusion, 386 patients (median age, 38 years; 309 females and 77 males) on first-line ARV treatment for a median duration of 24 months (range, 6–60 months) were included. Antiretroviral regimens were prescribed according to the 2006 revised WHO recommended ARV drugs, 12 including zidovudine (AZT), stavudine (d4T), lamivudine (3TC), and the nonnucleoside reverse transcriptase inhibitors (NNRTI) nevirapine (NVP) and efavirenz (EFV), or a protease inhibitor (PI)-containing regimen, with indinavir (IDV) boosted with ritonavir (IDVr).
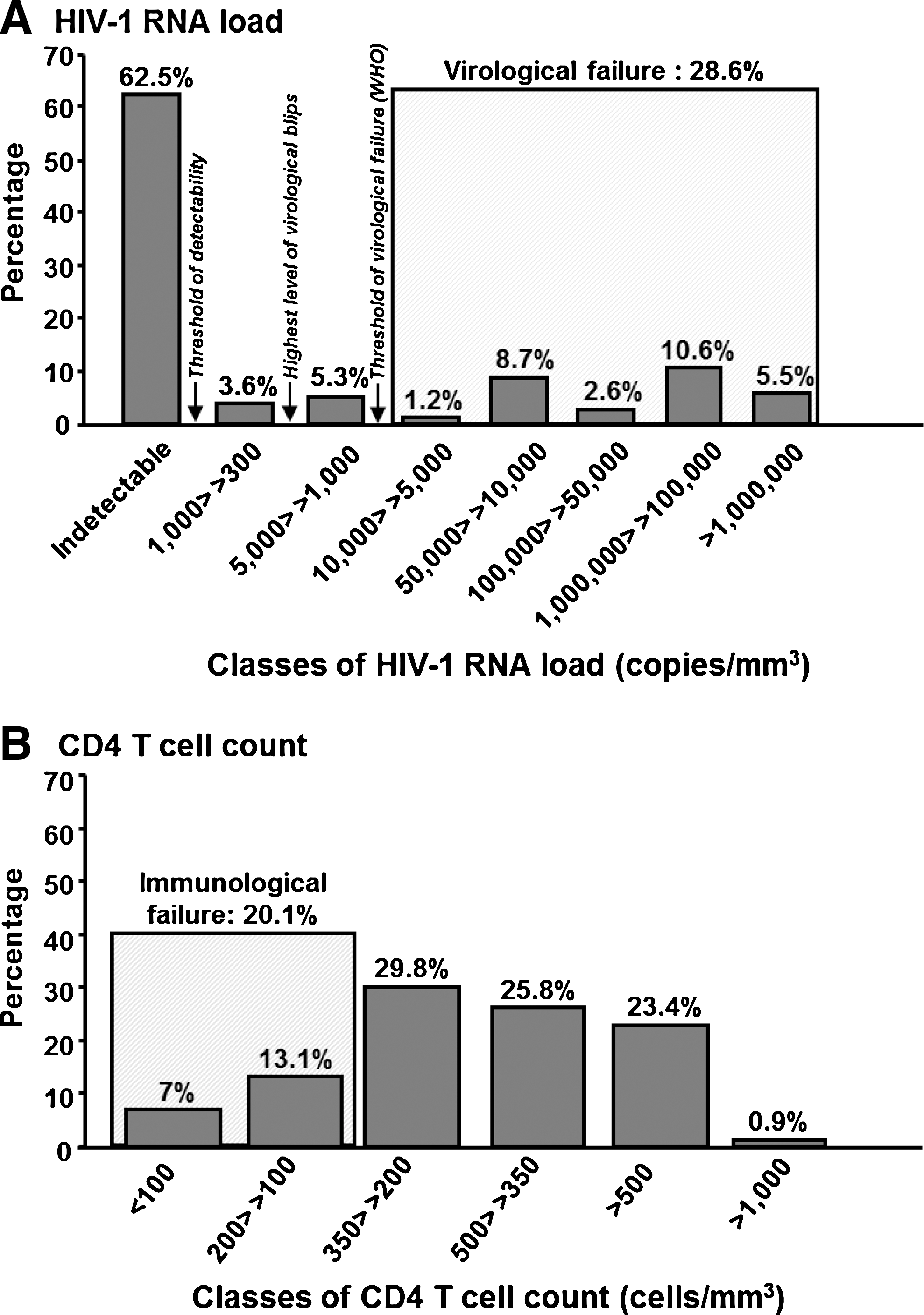
The distribution of plasma viral load levels in study patients is depicted in Fig. 1A. A total of 241 (62.5%) patients showed undetectable HIV-1 RNA viral load (<300 copies/ml), exhibiting virological success; 3.6% of patients showed low-level viremia, below 3.0 log10 copies/ml, likely due to possible transient viral blips; 5.3% of patients displayed moderately elevated HIV-1 RNA viral load, between 3.0 and 3.7 log10 copies/ml; unfortunately, a second determination of HIV-1 viral load was not carried out in these latter patients. Finally, 28.6% of patients had a plasma HIV-1 RNA viral load above 3.7 log10 copies/ml (5000 copies/ml), the threshold of virological failure, as recently recommended by the 2010 revised WHO criteria. 15
Distribution of HIV-1 RNA viral load
The distribution of CD4 T cell counts is depicted in Fig. 1B. A total of 24.3% of patients displayed CD4 T cell counts above 500 cells/mm3, and 25.8% of patients displayed CD4 T cell counts between 350 and 500 cells/mm3, 29.8% between 200 and 350 cells/mm3, 13.1% between 100 and 200 cells/mm3, and 7.0% of ARV-treated patients displayed severe immunodeficiency with a CD4 T cell count below 100 cells/mm3. Thus, 20.1% of patients had CD4 T cell counts remaining under the threshold of ARV treatment initiation according to the 2006 or 2010 revised WHO criteria for adults and adolescents (200 cells/mm3). 12,15 The percentage of treated patients with CD4 T cell counts under 350 cells/mm3, the new CD4 T cell threshold for treatment initiation, 15 reached 49.9%.
Genotypic resistance tests results
A genotypic resistance test was carried out in 45 of 145 (31%) patients with detectable plasma HIV-1 RNA load, by random selection of one out of three patients. The median age of these patients was 37 years. Thirty-four patients (76%) were female. At the time of genotypic resistance testing, the median HIV-1 RNA viral load and CD4 T cell count were 4.4 log10 copies/ml (range, 2.5–7.1) and 277 cells/mm3 (range, 36–658), respectively. The major ARV-based therapy prescribed was the generic combination of d4T/3TC/NVP in 36% (16/45) of patients. Other associations were AZT/3TC/IDVr in 18% (8/45) of patients, AZT/3TC/EFV in 16% (7/45), 3TC/d4T/EFV in 12% (5/45), 3TC/d4T/IDVr in 14% (6/45), and the ARV combinations AZT/3TC/NVP and 3TC/d4T/EFV/NVP in 2% (1/45) each.
The predominant subtype was CRF11_cpx (35%), followed by undetermined subtypes (15%), A1 (12%), CRF01_AE (12%), G (12%), D (5%), H (3%), CRF02_AG (3%), and CRF13_cpx (3%).
From 45 genotypic resistance tests, sequence results were successfully obtained in 34 samples (76%) for the RT gene and in 32 (71%) for the PR gene. A total of 8 (24%) of 34 patients in virological failure showed wild-type viruses susceptible to their ongoing ARV treatment, whereas 26 (76%) displayed plasma-resistant viruses to at least one ARV drug of their treatment (Fig. 2).
Percentage of patients whose viruses showed resistance-associated mutations to nucleoside reverse transcriptase inhibitors (NRTI)
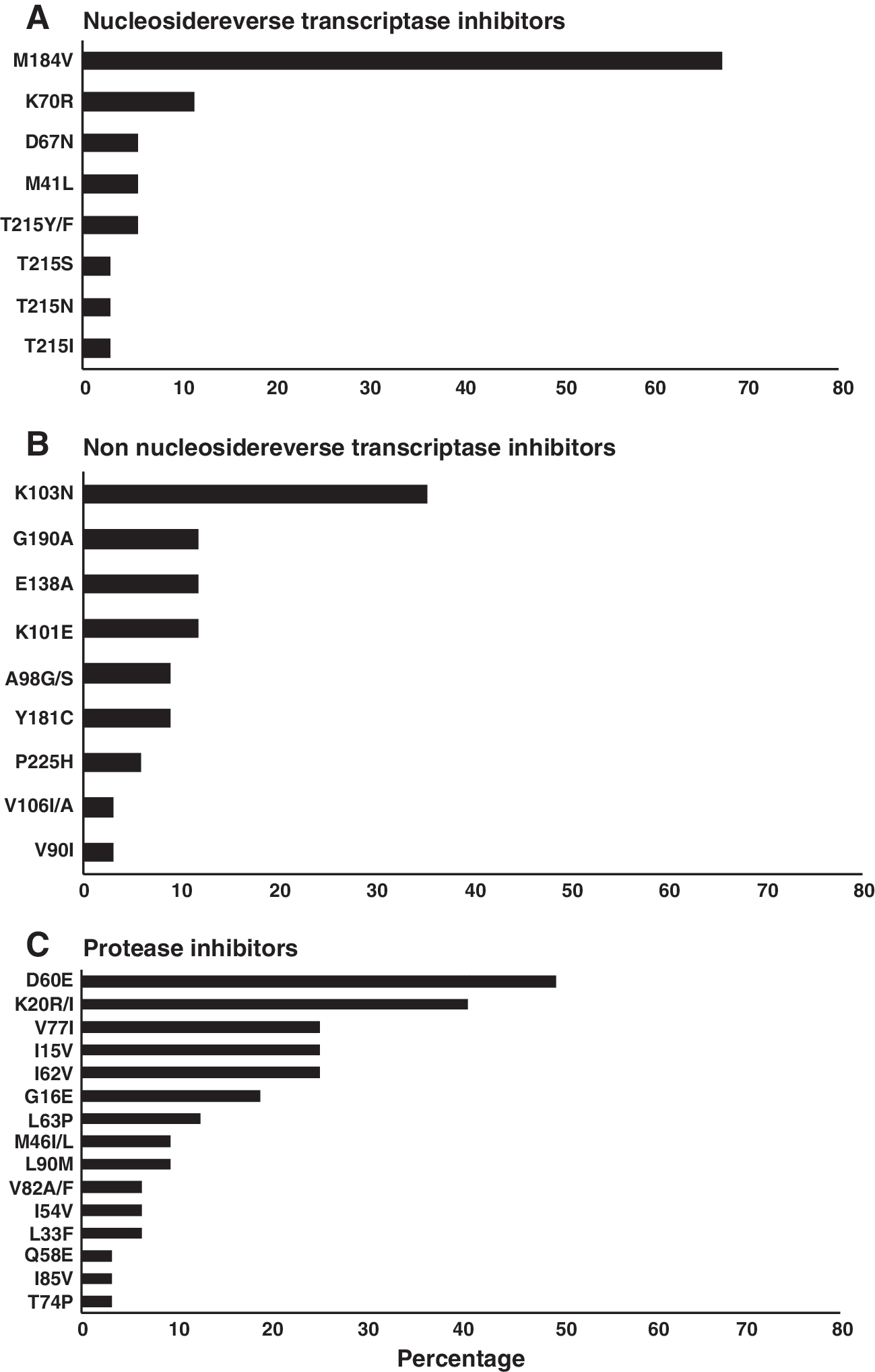
Regarding NRTI, 23 of 34 (67%) patients displayed virus harboring at least one mutation associated with NRTI resistance (Fig. 2A). In median, the virus exhibited one mutation associated with resistance to NRTI (range, 0–3). The most prevalent resistance mutations included M184V (n=23; 67%) followed by thymidine analog mutations (TAM) in 8 of 34 (24%) viruses (M41L: 2; D67N: 2; K70R: 4; and T215Y/F: 2). No viruses harbored the Q151M mutation or the insertion at codon 69 of the RT gene.
Assessing the prevalence of resistance to NNRTI, 23 of 34 (67%) patients displayed viruses harboring at least one NNRTI resistance mutation (Fig. 2B). In median, the viruses exhibited one mutation associated with resistance to NNRTI (range, 0–4). The most prevalent resistance mutations included K103H/N/S (n=12; 35%), followed by G190A (n=4; 12%), E138A (n=4; 12%), K101E (n=4; 12%), A98G/S (n=3; 9%), Y181I/C (n=3; 9%), P225H (n=2; 6%), V106I/M (n=1; 3%), and V90I (n=1; 3%).
Major resistance mutation to at least one PI was found in viruses from 6 of 32 patients (19%): M46I/L (n=3; 9%), L90M (n=3; 9%), and V82A/F (n=2; 6%) (Fig. 2C). The resistance mutations I54V and L33F (n=2 each; 6%) were also observed. In addition, as expected with HIV-1 non-B subtype protease sequences, a high frequency of natural polymorphisms was observed: the D60E mutation in 16 of 32 patients (50%) followed by K20R/I in 13 of 32 patients (41%), V77I, I15V, and I62V found in eight patients each (25%), followed by L63P (n=4;13%), and finally, I85V, Q58E, and T74V found in one patient for each (3%).
Overall, 26 of 34 (76%) patients displayed viruses harboring at least one major drug resistance mutation to NRTI, NNRTI, or PI molecules they were taking. Thus, 7 of 34 (21%) study patients harbored resistant viruses to one drug of their ongoing ARV-based therapy, 16 (47%) to two drugs, and 3 (9%) to all three drugs of their ARV-based therapy. If the M184V mutation is excluded, 26 of 34 (76%) patients displayed viruses harboring at least one drug resistance mutation to NRTI, NNRTI, or PI.
Figure 3 depicts the prevalence of sensitivity or resistance to the major ARV drugs used in the 2006 revised WHO recommendations, in the 34 patients whose genotypic resistance test was available. Thus, all study patients taking AZT displayed viruses yet remained sensitive to AZT, and the majority (85%) of patients under d4T showed viruses sensitive to d4T, with cross-resistance to AZT because of the presence of the T215Y/F/I mutation. In contrast, the majority (73% to 78%) of patients under NVP or EFV showed viruses resistant to NVP or EFV; cross-resistance to both NVP and EFV was noticed in 74% (n=17) of the 23 patients taking EFV or NVP whose viruses showed major NNRTI resistance mutations. Finally, half of the patients taking IDV had viruses resistant to this drug, but all remained sensitive to other PI drugs.

Percentage of patients whose viruses showed resistant (black) or sensitive (white) genotypes to their current antiretroviral treatment. The patients were followed up at “Hôpital de Jour” from July 2009 to October 2009, demonstrated detectable plasma HIV-1 RNA load, and had the benefit of a genotypic resistance test. AZT, zidovudine; d4T, stavudine; 3TC, lamivudine; EFV, efavirenz; NVP, nevirapine; IDV, indinavir; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors; PI, protease inhibitors.
The genotypic resistance profile could not be associated with viral diversity (not shown).
By considering the rate of detectable HIV-1 RNA load (37.5%) and the rate of major ARV drug resistance in the case of detectable viral load (76%), it is possible to estimate that 28.5% of the 386 study patients were in therapeutic failure.
Genotypic resistance tests interpretation and possible future therapeutic options
We further estimated possible ARV therapeutic options remaining in patients under virological failure, according to their resistance genotypes. Overall, the viruses of these latter patients remained susceptible to a median of five molecules of the six major available NRTIs [AZT, d4T, 3TC/FTC, ddI, abacavir (ABC), tenofovir (TDF)], a median of one molecule of the three major NNRTIs [EFV, NVP, etravirine (ETR)], and a median of seven molecules of the seven major PIs [IDV, saquinavir (SQV), nelfinavir (NFV), fosamprenavir (FPV), lopinavir (LPV), atazanavir (ATV), darunavir (DRV)].
Considering the NRTI class, plasma viruses of the 34 patients in virological failure with interpretable RT gene sequences were found to be susceptible to AZT and d4T in 91% (n=31), 3TC/emtricitabine (FTC) in 32% (n=11), ABC in 100% (n=34), and TDF in 100% (n=34). Thus, AZT and TDF, the two main ARV drugs included in the second-line regimen in Africa, 15 remained largely sensitive in patients with resistant viruses.
Considering the NNRTI class, plasma viruses of the 34 patients in virological failure were found to be susceptible to EFV in only 44% (n=15) and to NVP in only 41% (n=14). In contrast, the majority of patients displayed viruses remaining susceptible to the second-generation NNRTI ETR. Only one (3%) had virus harboring predicted resistance and four (12%) had possible resistance to this drug, due to the presence of the E138A mutation.
Considering the PI class, plasma viruses of 32 patients in virological failure with interpretable PR gene sequences were found to be susceptible to IDV in 87% (n=28), SQV in 91% (n=29), NFV in 87% (n=28), FPV in 91% (n=29), LPV in 97% (n=1), ATV in 91% (n=29), and DRV in 100%. Interestingly, more than 90% of patients in virological failure showed a remaining susceptibility to LPV and ATV, which constitute the major PIs of the second-line regimen in Africa, and DRV, which is recommended in the third-line regimen. 15
Interestingly, a panel of 10 patients (29%) showed viruses presenting a resistance genotypic profile whose interpretation by the ANRS algorithm predicted resistance to ARV drugs that they never received (Table 1). Thus, five patients had genotypic test results predictive of ETR resistance, possible (n=4; #4, #5, #7, #8; due to the presence of the E138A mutation) or full (#24; due to the accumulation of NNRTI resistance mutations under NVP). Two patients (#17 and #25) showed viruses with predicted resistance to EFV and NVP, whereas they had been treated only by PI-based regimen, likely because of interindividual transmitted drug resistance. Regarding the PI drug class, three patients (#4, #17, and #22) had viruses resistant to ATV and one (#22) to LPV, the two major PI molecules recommended in second-line ARV treatment. Furthermore, five patients (#4, #17, #22, #25, and #29) harbored viruses accumulating PI resistance mutations conferring cross-resistance to FPV, NFV, or SQV. Finally, one protease sequence issued from a PI-naive patient (#20) displayed possible resistance to SQV, related to the presence of natural polymorphisms at codons 10, 20, and 62 of the PR gene according to the ANRS algorithm.
In bold: major resistance mutations to protease inhibitors.
In italic: presence of resistance mutations to antiretroviral drugs never received.
Therapeutic history, current antiretroviral treatment, HIV-1 subtype, profiles of resistance-associated mutations to nucleoside reverse transcriptase inhibitors (NRTI), nonnucleoside reverse transcriptase inhibitors (NNRTI), or protease inhibitors (PI); interpretation of genotypic resistance profiles according to the ANRS algorithm in 10 patients showing viruses presenting a resistance genotypic profile compatible with resistance to ARV drugs that they never received.
ABC, abacavir; AZT, zidovudine; d4T, stavudine; ddI, didanosine; 3TC, lamivudine; TDF, tenofovir; EFV, efavirenz; NVP, nevirapine; ETR, etravirine; FPV, fosamprenavir; ATV, atazanavir; DRV, darunavir; IDV, indinavir; LPV, lopinavir; NFV, nelfinavir; SQV, saquinavir; IDV/r, indinavir boosted with ritonavir. S, sensitive; pR, possible resistant; R, resistant; nd, not determined.
The major final study results and conclusions have been reported to the Ministry of Health and to the National Council for AIDS (“Conseil National de Lutte contre le SIDA” or “CNLS”), Bangui, CAR.
Discussion
In the present study, the efficiency of ARV treatment was evaluated in 386 HIV-infected patients followed up in a health care center in the public sector in Bangui, and taking a first-line ARV regimen prescribed according to the WHO guidelines for a median duration of 24 months. Overall, 28.5% of ARV-treated patients were in virological failure, as assessed by a plasma viral load above 3.7 log10 copies/ml, and had been under treatment for more than 6 months. In addition, 20% of patients showed a CD4 T cell count under 200 cells/mm3 and 30% under 350 cells/mm3, indicating either ongoing immune restoration or immunological failure under treatment. Twenty-four percent of patients in virological failure showed wild-type viruses susceptible to all ARV drugs. However, 76% of them displayed plasma virus resistant to at least to one ARV drug, most frequently an NRTI (67%) or NNRTI (67%), followed by the PI class (19%), thus reflecting the therapeutic usage of ARV drugs in the CAR as recommended by the WHO. Further therapeutic options in patients in virological failure with resistant viruses included a median of five molecules of the NRTI drug class, one molecule of the NNRTI drug class, and all major PIs. Although in the majority (90%) of these latter patients, the second-line regimen proposed by the 2010 revised recommendations, including AZT, TDV, LPV, and ATV, could be effective, a minority showed a complex resistance genotypic profile highly predictive of resistance to the usual WHO second-line regimen. Thus, the analysis of genotypic resistance mutations appeared markedly relevant, even necessary, in some patients in virological failure. However, the therapeutic options resulting of the determination of resistance mutations frequently included ARV drugs hardly available in the CAR. Taken together, these observations indicate that virological failure may be frequently encountered in patients cared for in the public sector of Bangui, which emphasizes the need to perform plasma viral load measurement and the need for genotypic analysis of ARV resistance in a minority of patients in therapeutic failure not responding to a second-line ARV regimen as proposed by WHO guidelines.
Virological failure associated with ARV drug resistance has been frequently observed in treated patients in Central Africa settings, at variable rates according to duration of treatment, health care services, and urban or remote areas, such as in Cameroon 8,16 –19 and Chad. 5 For example, our observations showed seemingly higher rates of both virological failure (around one-third of patients) and resistant viruses (around 80%) in cases of detectable viral load under treatment than previously reported in the private sector in Douala, Cameroon. 8 These features contrast with the relatively low prevalence of resistant viruses under ARV treatment, previously reported by Kouanfack and colleagues at the universitary Central Hospital of Yaoundé. 18 The differences between the rates of virological failure and resistant viruses observed in patients followed in Yaoundé and those in Douala or Bangui may be due in part to differences in the levels of health care services between settings. Numerous socioeconomic factors, the heterogeneousness of health care services, and the occasional difficulties of ARV drug distribution and of payment of routine biology tests for treatment monitoring may contribute to explaining the relative high prevalence of virological failure observed in the study patients. Furthermore, the lack of availability of plasma HIV-1 RNA load monitoring in the CAR likely increases the risk of virological failure associated with the selection of ARV-resistant viruses.
Interestingly, wild-type viruses were detected in 24% of adults under first-line ARV treatment in virological failure (plasma viral load >3.7 log10 copies/ml). This finding is to similar to the rate of 20% of adult patients in virological failure with sensitive viruses previously reported in Douala. 8 Virological failure with sensitive viruses is likely due to poor adherence, which must be urgently corrected. Virological monitoring appears particularly of interest in ARV-treated patients, who may have difficulties in displaying good adherence, in order to diagnose virological failure early and to reduce the duration of viral replication under ARV drug pressure, preventing the selection and further accumulation of resistance mutations.
Seventy-six percent of patients in virological failure displayed plasma viruses resistant to at least to one ARV drug. Such a high level of virological failure has been similarly reported in a series of ARV-treated adult patients living in sub-Saharan Africa, 3 –6, 8 and reflects the wide use of ARV drugs characterized by a low genetic barrier to resistance, such as 3TC or NNRTI. As expected, drug resistance prevalence was correlated with the differential use of ARV drug classes: 67% NRTI, 67% NNRTI, and 19% PI, thus corresponding to the therapeutic usage of ARV drugs in the CAR as recommended by the WHO.
Only 9% of patients exhibited plasma viruses resistant to all three drugs of their ongoing ARV-based therapy, a rate similar to previous data reporting less than 10% of triple-drug-resistant virus in ARV-treated patients displaying virological failure. 4,5 In addition, nearly half the patients (47%) displayed major resistance mutations to two ARV molecules of their current treatment. These observations emphasize the fact that ARV resistance to first-line therapy in the present series mostly impacts two to three therapeutic classes. This outcome is likely to be related to a long period of detectable HIV-1 viral load under ARV-based therapy, 17 which may occur in Africa due to the lack of viral load control and to a delay in the diagnosis of virological failure with the risk of the accumulation of drug resistance mutations and of reduced future therapeutic options. 20 Even after excluding the M184V mutation, the majority of patients (76%) in virological failure continued to display viruses harboring at least one major drug resistance mutation to NRTI, NNRTI, or PI. This finding may be explained by the very high prevalence of the K103N NNRTI resistance mutation. Since the presence of the M184V resistance mutation to 3TC/FTC does not exclude further systematic use of 3TC/FTC in second-line treatment, it can be hypothesized that a significant proportion of patients taking second-line ARV treatment as recommended by the WHO will in fact receive two fully active ARV drugs in the context of viruses harboring the M184V mutation, which is thought to decrease viral fitness. 21,22 However, the in vivo impact of the M184V mutation in viruses of patients under second-line treatment should be investigated in African cohorts.
In the present series, the antiviral activity of ARV drugs in the second-line regimen proposed by the 2010 revised WHO recommendations in case of virological failure was not greatly impacted, with a predictive activity of the four major second-line drugs, AZT, TDF, LPV, and ATV, in more than 90% of cases. The relatively low proportion (24%) of TAM selection in the present series of patients in virological failure may be associated with the high frequency of the M184V mutation, conferring increased sensitivity to AZT and d4T, thus contributing to the lower frequency of TAM. 23,24 Furthermore, the low rate of TAM makes it possible to retain sensitivity to TDF, whose resistance needs an accumulation of at least three TAMs according to the ANRS interpretation algorithm. IDV-based treatment in the first-line regimen was associated with IDV resistance in 50% of patients taking this drug. However, the observed IDV resistance had no significant impact on further use of LPV or ATV, likely because the genetic barrier to resistance of LPV is known to be high, and the resistance profile of ATV is different from that of IDV. Finally, the sensitivity to DRV, which is recommended in a third-line regimen, 15 was 100%.
A minority of study patients in virological failure showed genotype resistance profiles compatible to resistance to the major molecules recommended in second-line treatment: 3% of them to LPV and 9% to AZT or ATV. In the CAR where genotyping resistance testing is not routinely available, these observations emphasize the need to carefully monitor the plasma HIV-1 RNA load in patients switching from first-line to second-line regimens. Only virological monitoring carried out 1 to 3 months after therapeutic change could likely allow early diagnosis of the failure of second-line treatment due to preexisting resistant viruses.
Interestingly, nearly one-third of patients in therapeutic failure had resistant viruses harboring complex resistance profiles, when interpreted using current a algorithm, such as the ANRS. Thus, the activity of ETR, a new second-generation NNRTI, appeared compromised in around 15% of circulating HIV-1 strains, despite the fact that the drug has been never introduced in the CAR. Such a high prevalence of predicted ETR resistance, which has been similarly observed in Cameroon, 8 appears much higher than rates (2.4% and 3.8%) previously reported in Western countries. 25,26 In the present series, primary resistance to ETR may reflect possible genetic specificity of HIV-1 “non-B” subtypes, 27 or may be associated with the long duration of viral replication under first-generation NNRTI drug pressure. Furthermore, interpretation of resistance genotype profiles makes it possible to detect interindividual transmitted drug resistance to NNRTI, cross-resistance within the PI drug class, and the possible impact on ARV treatment of natural polymorphisms in RT and PR genes of HIV-1 “non-B” subtypes. Finally, a minority of patients in virological failure showed complex resistance genotypic profiles, which may be resolved only with genotypic resistance tests.
In conclusion, virological failure of a first-line ARV regimen, generally associated with major ARV drug resistance mutations, appears particularly frequent in HIV-1-infected adults living in the CAR and treated according to the WHO recommendations. This has important public health implications. First, it emphasizes the need to improve the distribution of ARV drugs, to increase the adherence of treated patients, and to offer adequate HIV biological monitoring. Second, it should now be considered in all further programs for ARV drug access for HIV-infected adults living in this country, since around 30% of currently ARV-treated adults may be considered to be in therapeutic failure; these people now need original therapeutic options, likely more expensive and surely difficult to obtain in the context of resource-limited settings.
Footnotes
Acknowledgments
We thank Miss Sandra Perrot and Dr. Alexis Naissem, from GIP-ESTHER, for contributions and relevant discussions. Financial support is from Ensemble pour une Solidarité Thérapeutique en Réseau (GIP-ESTHER).
Author Disclosure Statement
No competing financial interests exist.