
Abstract
Antiretroviral naive patients (n=49) were recruited in central western Brazil (Campo Grande City/Mato Grosso do Sul State, located across the Bolivia and Paraguay borders). HIV-1 protease (PR), reverse transcriptase (RT), and env gp41 HR1 fragments were sequenced. Genetic diversity was analyzed by REGA/phylogenetic analyses. Intersubtype recombinants were identified by SimPlot/phylogenetic trees. PR/RT resistance was analyzed by Calibrated Population Resistance/Stanford databases. T-20 resistance in gp41 was assessed by Stanford, Los Alamos, and other sources. Of HIV-1 subtypes 65.3% were BPRBRT, 10.2% were CPRCRT, and 8.2% were F1PRF1RT. Intersubtype recombinants were 16.3%: four B/F1 and four B/C (two were “CRF31_BC-like”). The Pol-RT V75M mutation was detected in two homosexual partners; one patient had the T215S revertant mutation. T-20/gp41 resistance mutations were L44M (n=2) and V38A (n=1). The high percentage of non-B isolates (∼35%) highlights the importance of molecular surveillance studies in settings distant from the origin of the epidemic. Our data help elaborate the molecular epidemiological map of HIV-1 in Brazil.
Different regional patterns have been observed in the AIDS epidemic in Brazil, the largest country in Latin America. The State of Mato Grosso do Sul, in central western Brazil, presents interesting epidemiological features for a study site about HIV-1 genetic diversity and transmitted drug resistance. Mato Grosso do Sul State borders Bolivia and Paraguay and represents an important route of entry of illegal drugs, which are then distributed to the rest of the country. The possible impact of injecting drug use in HIV-1 diversity and drug resistance in this setting has not been explored. Moreover migrants, especially from southern Brazil, are an important component of the population in this state.
HIV-1 subtypes B, F1, C, and D cocirculate in Brazil. 1 In recent years several recombinant viruses including circulating recombinant forms (CRFs) and unique recombinant forms (URFs), mainly with subtypes B/F1 and B/C, have been described. 2 –4 The identification of subtypes circulating in smaller urban centers distant from the origin of the epidemic will contribute to forming the actual molecular epidemiological map of HIV-1 in the country. 5 –7
First line antiretroviral (ARV) treatment options comprise different combinations of nucleoside and nonnucleoside reverse transcriptase inhibitors (NRTIs and NNRTIs) or protease inhibitors (PIs). 8 In Brazil ARV therapy has been offered free of cost by the public health system since 1996. The prevalence of transmitted drug resistance mutations among naive patients varies in developed and developing countries and correlates with the level of exposure of the population to ARV drugs. Most recent studies have shown mainly low (<5%) to moderate (5–15%) levels of transmitted drug resistance in Brazil. 1,9
The fusion inhibitor enfuvirtide (T-20), a synthetic 36-amino acid peptide, binds to the heptad repeat 1 (HR1) domain preventing its interaction with the heptad repeat 2 (HR2), which is required for entry of HIV-1 into host cells. 10 T-20 has been recommended for salvage therapy in highly ARV-experienced patients.
This study describes HIV-1 phylogenetic diversity and natural resistance mutations in the protease (PR), reverse transcriptase (RT), and env HR1 gp41 fragments among ARV-naive patients recruited in Mato Grosso do Sul State. Consecutive ARV-naive patients infected with HIV-1 were recruited in 2008 (July–December) and 2010 (August–November) at the Central Laboratory/LACEN and “Hospital Dia Professora Esterina Corsini” in Campo Grande City (766,461 inhabitants), capital of the state of Mato Grosso do Sul. Patients infected with HIV-1, from both sexes, above 18 years, who had never been exposed to any ARV therapy, were included. Local ethic committees approved this study (“Comitê de Ética em Pesquisa do Hospital Dia Professora Esterina Corsini/Mato Grosso do Sul” protocol #435/CEP-HUJM/07 and “Comitê de Ética em Pesquisa Médica Humana e Animal da Universidade Federal de Goiás” protocol #073/05). Signed informed consents were obtained from all participants. Standardized questionnaires were used to collect sociodemographic, clinical, and laboratory data. Exposure category of three patients, viral load of one patient, and CD4 cell counts of two patients were not available.
Plasma RNA was extracted and transcribed to obtain complementary DNA. The entire HIV-1 PR, approximately 750 bp of the RT fragment and 766 bp of the HIV-1 gp41 fragment (HR1 region), were amplified by nested polymerase chain reaction (nested PCR). The amplified products were directly sequenced in an automatic sequencer as previously described.
6,11
HIV-1 subtypes were identified using the REGA tool and by phylogenetic inference. Phylogenetic trees were performed by neighbor-joining under Kimura's two-parameter correction (1000 bootstrap) (MEGA4 software) as previously reported.
6,11
PR/RT intersubtype recombinations were analyzed by SimPlot 3.5.1 (200 bp window/20 bp increments) and by phylogenetic analyses of individual fragments.
6,11
HIV-1 recombinant breakpoints were mapped using the Recombinant HIV-1 Drawing Tool available at the Los Alamos HIV-1 site (
Transmitted drug resistance in PR/RT and natural resistance mutations in env gp41 was analyzed using the Calibrated Population Resistance tool (Stanford Surveillance Drug Resistance Database) as previously described.
6
HIV-1 env gp41 resistance mutations to T-20 were defined by the Stanford online HIV Drug Resistance Database (
Frequencies and medians of main variables were assessed using the Statistical Package for the Social Sciences (SPSS) software for Windows version 13.0 (Chicago, IL).
Naive patients recruited were 61.2% (30/49) males, with a median age of 36 years (range 19–64 years); 67.3% (33/49) were men referred for heterosexual unprotected sex and 26.6% (13/49) were men who have sex with men. The median of CD4 cell counts was 392 cells/μl (range 46–1246 cells/μl) and the median of the viral loads was 20,416 copies/ml (range 79–268,674 copies/ml).
A high percentage of non-B HIV-1 isolates was detected (∼35%): 10.2% (5/49) were subtype C, 8.2% (4/49) were subtype F1, and 16.3% (8/49) were intersubtype recombinants in the PR/RT fragments. HIV-1 subtype B represented 65.3% (32/49) (Fig. 1). No relevant difference was observed in HIV-1 subtypes circulating among heterosexual and homosexual patients. The following recombination profiles were observed within PR/RT fragments: F1PR/BRT (n=2), F1BPR/BF1BRT (n=1), BF1PR/F1BRT (n=1), BPR/BCRT (n=1), CPR/CBRT (n=2), and CPR/CBCRT (n=1) (Fig. 2). The two CPR/CBRT isolates identified in this study were classified as CRF31_BC-like by REGA analysis. 3 In terms of profiles and breakpoints none of the B/F1 recombinants reported resembled CRF28_BF, CRF29_BF, CRF39_BF, or CRF40_BF previously described in southeastern Brazil. 2,4 Taking into account the HIV-1 genetic diversity in the three fragments sequenced (PR/RT and env gp41) the percentage of potential recombinants increased from 16.3% to 24.8%. Full-length or near full-length genomes are necessary to elucidate whether these recombinants identified in Mato Grosso do Sul State are any of the already described CRFs, another CRF, or URFs.
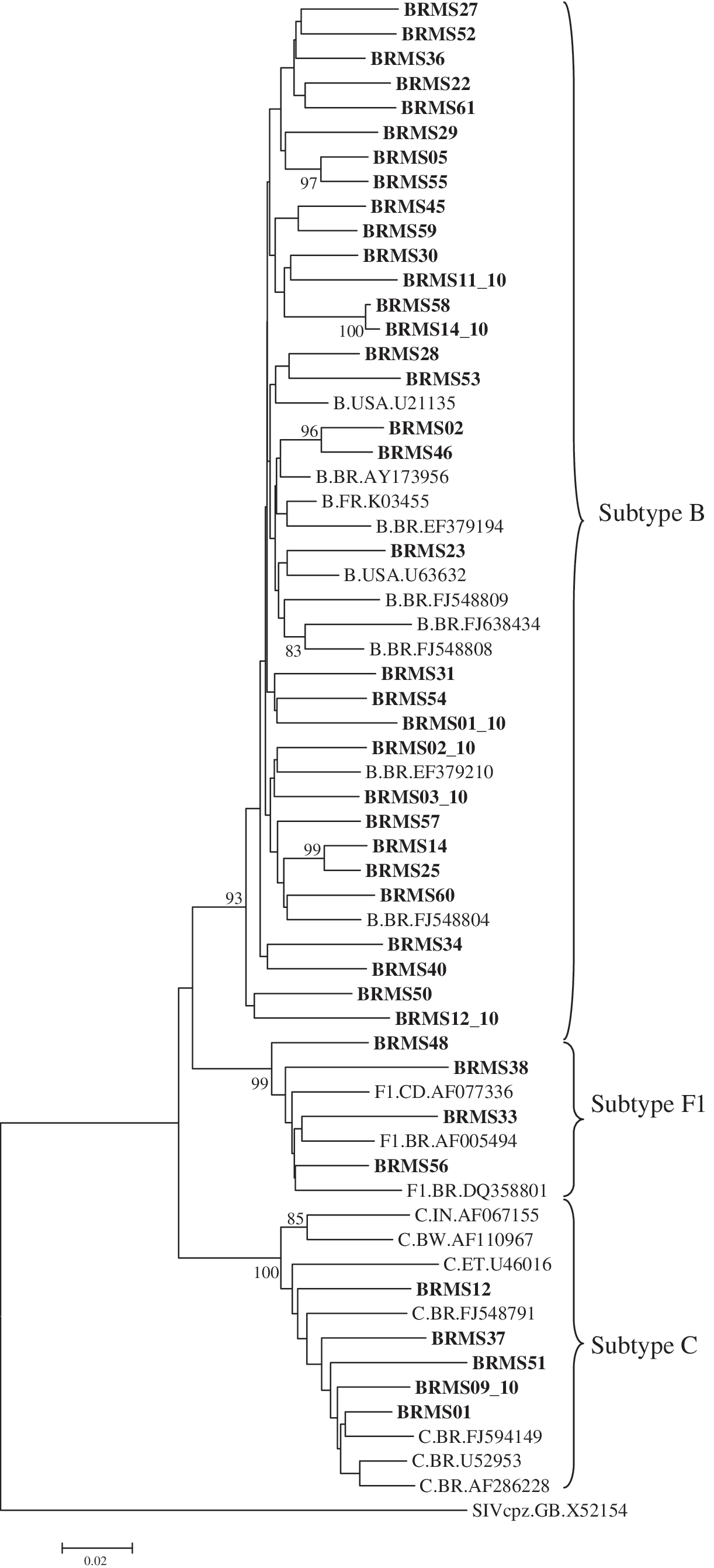
Phylogenetic of HIV-1 isolates in the PR and RT fragments among HIV-1 isolates from Mato Grosso do Sul State. Boostrap values above 70% were considered significant. The isolates characterized in this study are given in bold. GenBank accession numbers used in the comparative phylogenetic analyses are subtype B: U21135, AY173956, K03455, EF379194, U63632, FJ548809, FJ638434, FJ548808, EF379210 and FJ548804; subtype C: AF067155, AF110967, U46016, FJ548791, FJ594149, U52953 and AF286228; subtype F1: AF077336, AF005494 and DQ358801 and the simian immunodeficiency virus sequence from chimpanzee (SIVcpz): X52154.
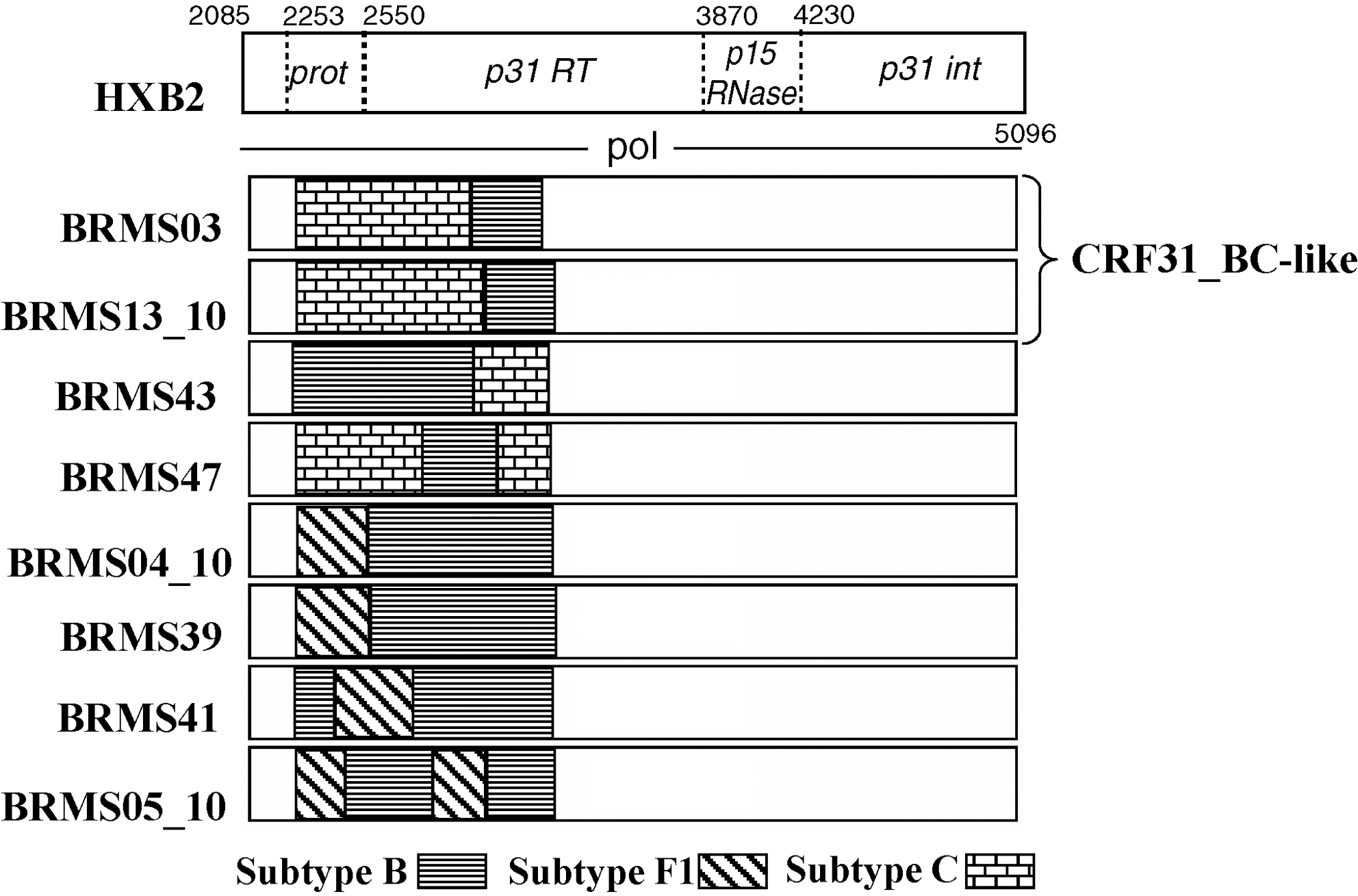
Map of recombinant breakpoints of HIV-1 isolates from Mato Grosso do Sul State.
A relatively high rate of HIV-1 subtype C was found (∼10%) in Mato Grosso do Sul State, where an important southern-western migration flow took place in the last decades due to larger areas for livestock breeding and agriculture. It is possible that subtype C in this state was introduced by these southern migrants since, as opposed to the rest of the country HIV-1 subtype C prevails among patients from southern Brazil. In fact, phylogenetic analyses confirmed the monophyletic clustering of subtype C circulating in Mato Grosso do Sul State and subtype C sequences from southern Brazil (Fig. 1). In the central western state of Goias, where this southern migration has not been as evident, subtype C still represents a minor genetic variant. 1,3,9 All HIV-1 isolates classified as subtype C in the pol region were assigned to another subtype in the gp41 region, representing possible recombinant viruses. These results indicate that HIV-1 subtype C may be also circulating as a recombinant among patients from Mato Grosso do Sul State.
We acknowledge that our sample size is not representative of the patients infected with HIV-1 from Mato Grosso do Sul State. Therefore we preferred to describe the individual mutations associated with resistance instead of calculating the estimated prevalence of transmitted resistance. Two homosexual partners had the transmitted pol-RT V75M mutation to NRTI, which causes intermediate resistance to stavudine (d4T) and low resistance to didanosine (ddI). Another patient presented the pol-RT revertant mutation T215S. Revertants T215S/C/D/E/I/V are considered transitions between wild-type and the Y and F mutations. Although they usually do not reduce NRTI susceptibility, their presence suggests that T215Y/F had either been present or may be present as minority populations.
In the neighboring state of Goias (central western) and in Tocantins State (northern) moderate rates of transmitted resistance (around 10%) have recently been reported. 6,7 Knowledge about HIV-1 transmitted resistance on a population level can be useful for improved prevention and treatment decisions.
Although resistance is uncommon in patients never treated with T-20, natural resistance mutations in treatment-naive patients have been described. 12,13 Three naive patients, harboring subtype B, presented resistance mutations to T-20: the L44M mutation (n=2) and the V38A mutation (n=1). T-20 mutations have been observed in multidrug-resistant patients, never treated with T-20, suggesting that highly active antiretroviral therapy could have selected these mutations. 14 In Goias State (central western Brazil) around 20% of isolates from multidrug-resistant patients presented G36E, N42T, and N43S mutations to T-20. 11
The pol and env sequences from this study are among the first HIV-1 sequences from this central western Brazilian State deposited in GenBank. In this sense, the molecular data about Mato Grosso do Sul State presented in this study, contribute to mapping HIV-1 diversity in a country with continental territorial dimensions, such as Brazil. These results highlight the importance of surveillance studies on HIV-1 diversity and drug resistance among patients from settings distant to the origin of the epidemic.
Sequence Data
The GenBank accession numbers of the sequences presented in this study are JF342273–JF342353.
Footnotes
Acknowledgments
This study was supported by UNESCO AIDS/STD National Program, Brazilian Ministry of Health (Grant 310-06). M.M.A. Stefani is a recipient of a fellowship from the National Counsel of Technological and Scientific Development/CNPq (Grant 304869/2008-2) and A.A. Silveira (Grant 141211/2008-3) and L.P.V. Cardoso (Grant 141820/2006-3) were supported by scholarships from CNPq.
Author Disclosure Statement
No competing financial interests exist.