
Abstract
An unusual case of necrotizing gingivitis and neutropenic oral ulcers in an HIV-seropositive patient is presented. In spite of a very low CD4+ T cell count and severe neutropenia, the necrotizing gingivitis responded favorably to standard periodontal treatment, and the oral ulcers healed after administration of granulocyte colony-stimulating factor (G-CSF). Nonspecific oral ulcers in HIV-seropositive subjects with neutropenia should be regarded as neutropenic ulcers. The term nonspecific ulcers should be restricted to those ulcers with nonspecific histopathological features in patients without neutropenia or a nutritional deficiency such as iron, folic acid, and vitamin B.
Introduction
HIV-
Both necrotizing gingivitis/necrotizing periodontitis, collectively referred to as necrotizing periodontal diseases, and nonspecific oral ulcers are well known to be associated with HIV infection. 1 The clinical signs, course, and response to treatment of necrotizing periodontal diseases are similar in HIV-seropositive and in HIV-seronegative subjects. 4 –7
Neutropenia, defined as an absolute neutrophil count of less than 1.5×109 cells/liter, can have a variety of causes (Table 2). 8 HIV-associated neutropenia may result from myelosuppression indirectly mediated by HIV, 9 from HIV-mediated increased neutrophil apoptosis, 10 from side-effects of drugs, or from HIV-associated infections. Treatment with colony-stimulating factors, both granulocyte colony-stimulating factor (G-CSF) and granulocyte-macrophage colony-stimulating factor (GM-CSF), increases neutrophil counts in HIV-seropositive subjects with neutropenia regardless of the cause of the neutropenia. 11 –13
Although oral ulcers may vary in clinical appearance in neutropenic subjects, they may resemble recurrent major aphthous ulcers but without a history of recurrence. 14 Effective treatment of the neutropenia will bring about resolution of the neutropenic ulcers.
Nonspecific (not otherwise specified) oral ulcers are not uncommon in HIV infection. 15 According to the literature, a diagnosis of HIV-associated nonspecific ulcers should be reserved for those cases of nonrecurrent ulcers in which neither specific histopathological nor specific microbiological features can be found. 1 However, it is not unlikely that hematological investigation might have shown that some of the previously reported cases of nonspecific oral ulcers may have in fact been attributable to HIV-associated neutropenia.
Herein we present an illustrative case of HIV-associated neutropenic ulcers that, had blood tests not been performed, might have been misdiagnosed as HIV-associated nonspecific oral ulcers.
Case Report
A 46-year-old HIV-seropositive male was referred with multiple painful oral ulcers and painful gingival lesions. The patient stated that his lesions on the upper labial mucosa (Fig. 1) and on the tongue (Fig. 2) had developed about a month previously, and the gingival lesions (Figs. 3 and 4) about 5 days previously, and that the lesions were getting progressively larger and more painful. The patient reported, furthermore, that he had HIV infection for 8 years. Shortly after his HIV diagnosis, highly active antiretroviral therapy (HAART) was started, but 1 year before we saw him he had stopped HAART owing to financial constraints and had been in the position to resume the treatment only 3 weeks earlier. The cocktail of HAART comprised stavudine, lamivudine, and efavirenz.

Ulcer on the upper labial mucosa.

Ulcer on the dorsum of the tongue.
Inflamed necrotic palatal maxillary gingiva adjacent to the posterior teeth.

Inflamed necrotic marginal gingiva of the mandibular teeth.
The patient appeared to be in good health, did not smoke or use alcohol, was not taking any medication other than HAART, and his physical examination did not reveal any abnormalities.
On oral examination, the palatal masticatory mucosa adjacent to the maxillary left molars (Fig. 3) and the labial marginal gingiva in the mandibular incisor region (Fig. 4) were erythematous, necrotic, painful, and bleeding. The dentogingival microbial plaque control was poor. Necrotizing gingivitis was diagnosed.
There was an ulcer on the dorsum of the tongue (Fig. 2) and another on the upper labial mucosa (Fig. 1). The clinical differential diagnosis included HIV-associated nonspecific ulcers, neutropenic ulcers, syphilitic ulcers, tuberculous ulcers, and major aphthous ulcers. No other oral diseases were evident.
Microscopic examination of the biopsy specimen from the labial mucosal ulcer failed to reveal any specific histopathological features. A blood sample was taken and revealed that there was severe neutropenia (0.29×109 cells/liter; reference range 2.00–7.5), the CD4+ T cell count was 5 cells/mm3 (reference range 600–1550), and the CD4+ T cell percentage was 0.84% (reference range 30–60). Neither anemia nor thrombocytopenia was detected. The HIV viral load was 272,185 HIV-1 RNA copies/ml (5.435 log units). Serological tests were indicative of previous infections with CMV, HSV-1, and HSV-2.
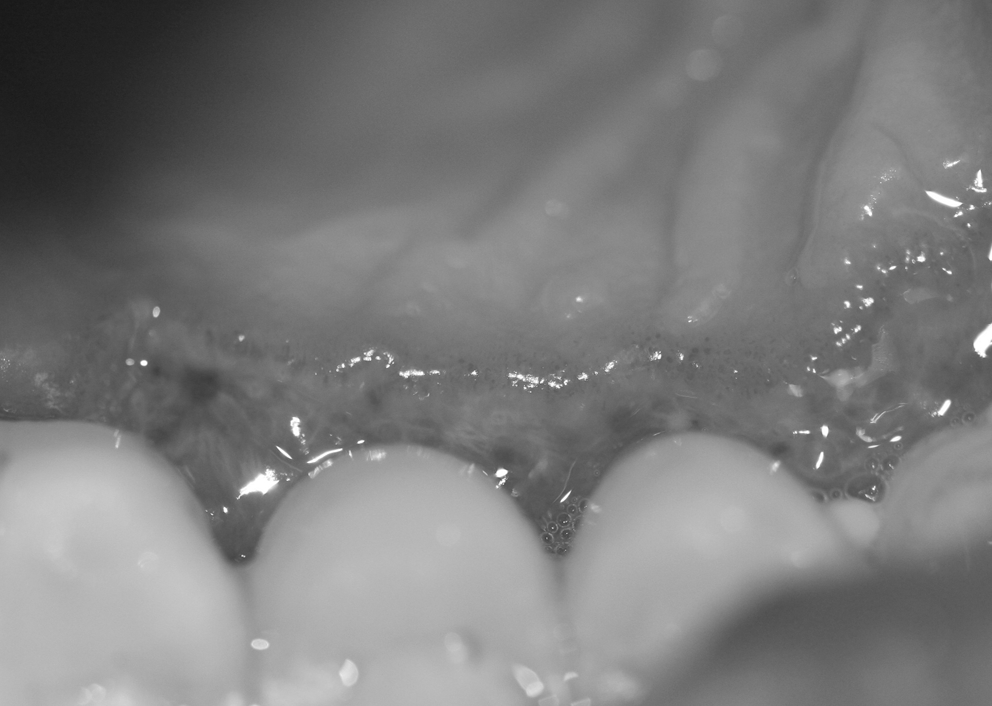
The patient received amoxicillin 500 mg and metronidazole 400 mg three times a day for 5 days and chlorhexidine 0.2% mouthwash twice a day for the treatment of his necrotizing gingivitis. After 2 weeks the gingival lesions were healing (Figs. 5 and 6), but the ulcers were not significantly better. The patient was given plaque-control instruction, and his teeth were scaled and polished to prevent recurrence of his necrotizing periodontal disease and to maintain his periodontal health.

Two weeks after treatment as described in the text, despite inadequate plaque control, the gingiva had greatly improved.

On the basis of the hematological investigations and the absence of specific histopathological features of the ulcers, a diagnosis of neutropenic ulcers was made. The patient was given filgrastim, a nonglycosylated recombinant methionyl human G-CSF, and 3 weeks later the labial ulcer had healed as had the ulcer on the tongue, though the latter had left a residual defect (Fig. 7). Although the patient had refused further neutrophil, CD4+ T cell, and HIV viral load investigation, after 18 months the patient was still well and had not had any recurrence of the oral lesions.

The residual defect on the tongue.
Discussion
There are many causes of persistent oral ulcers, several of which are uncommon. 16,17 To reach a definitive diagnosis, any nonhealing oral ulcer should be biopsied, and if the microscopic examination does not reveal specific diagnostic features, systemic factors should be excluded by appropriate investigations. 16 The microscopic appearance of the ulcers in our case was nonspecific, but blood tests revealed severe neutropenia.
Severe neutropenia alone is a risk factor for oral ulcers. 17,18 Ulcers without any characteristic histopathological features and without any discoverable cause are referred to as idiopathic nonspecific ulcers. 1,15 HIV-associated nonspecific oral ulcers, although similar in clinical appearance to major aphthous ulcers and neutropenic ulcers, have no history of recurrence, 1 and are not associated with neutropenia.
It has been suggested that the occurrence of nonspecific oral ulcers soon after the initiation of effective HAART might represent an immune reconstitution inflammatory syndrome (IRIS). 19 The link between IRIS and nonspecific oral ulcers may be an immunoinflammatory reaction to as yet unidentified antigens. Immunohistochemical and in situ hybridization studies have demonstrated that CD68+ macrophages and CD8+ T lymphocytes play an important role in the pathogenesis of HIV-associated nonspecific oral ulcers. 15 Therefore, it is reasonable to assume that dysregulated immune-mediated inflammatory responses to a preexisting subclinical pathogen or tissue antigen, after improvement in all HIV-related immunologic parameters early after the introduction of HAART, 20 may lead to the development of nonspecific oral ulcers in a subset of HIV-seropositive subjects. 19
Although nonspecific oral ulcers may occur as an IRIS phenomenon, the lack of any overt exuberant inflammatory response in this case was contrary to the concept of IRIS.
Since our patient exhibited severe neutropenia and had oral ulcers that were not recurrent and were microscopically nonspecific, we therefore diagnosed them as neutropenic ulcers. A shortcoming in the logical sequence culminating in this diagnosis is that a neutrophil count was not done after administration of G-CSF because the clinical condition had rapidly improved and the patient was not prepared to submit to any further hematological examination. It could be argued that resolution of the ulcers was a spontaneous time-related process, but the duration of the ulcers before the use of G-CSF and the fact that the ulcers healed when G-CSF was administered are strong evidence in support of the diagnosis.
The diagnosis of HIV-associated nonspecific oral ulcers should be reserved for nonrecurrent oral ulcers without specific microbiological and histopathological features, and in relation to which hematological abnormalities cannot be found. If there is neutropenia, the nonspecific ulcer should be diagnosed as a neutropenic ulcer.
This is not the conventional view expressed in the literature: without consideration of the neutrophil status HIV-associated oral ulcers are generally characterized as being nonspecific if microbiological studies and histopathological examinations are diagnostically negative. 1 In fact, some reported cases might well have been HIV-associated neutropenic ulcers.
The treatment of oral neutropenic ulcers and the treatment of nonspecific oral ulcers in HIV-seropositive subjects are different, so a correct diagnosis is important. Neutropenic ulcers will heal only after the causative agent of the neutropenia, such as myelosuppressive drugs, is eliminated, or if the neutrophil level is restored by administration of G-CSF, as in our case.
On the other hand, nonspecific oral ulcers are more difficult to treat. However, mild cases usually respond to high-potency topical corticosteroids, moderate cases to intralesional corticosteroid injections, and severe or persistent cases to systemic corticosteroids, or as a last resort to thalidomide. 16,21
It is possible, indeed probable, that treating ‘nonspecific oral ulcers’ in neutropenic HIV-seropositive subjects with steroids or thalidomide will not bring any resolution of the ulcers if the neutropenia has not been treated. This may explain the reported observations that HIV-associated nonspecific oral ulcers are refractory.
Neutropenia is common in HIV infection and may be brought about either by decreased production or by increased peripheral elimination of neutrophils, 10,12,22 –24 and is related to the CD4+ T cell count and to the HIV viral load. In HIV-seropositive subjects with neutropenia, decreased viral load and increased CD4+ T cell count brought about by HAART lead to resolution of neutropenia. However, inclusion of myelosuppressive agents such as zidovudine or lamivudine in the cocktail of HAART may hinder the resolution of the neutropenia or even increase it. 13,25
Neutropenia in HIV-seropositive subjects may be a consequence of an increase in constitutive neutrophil apoptosis, 24 neutrophil apoptosis owing to upregulation of cell death receptor pathways, 22 a low serum level of G-CSF, 13 or bone marrow dysfunction 10,23,26 individually or in concert.
HIV does not infect myeloid progenitor cells. The virus infects bone marrow stromal cells, particularly macrophages and microvascular endothelial cells, leading to changes in the bone marrow microenvironment, resulting in inhibition of myeloid hematopoiesis. Thus, HIV indirectly affects hematopoietic progenitor cell differentiation and clonal expansion. 10,23 Furthermore, infections concurrent with HIV, antiretroviral agents, and HIV-induced disturbance of cytokine profiles may all contribute to the myelosuppression in HIV infection. 27
Our patient had a high-level HIV viral load (5.435 log units), a very low CD4+ T cell count (5 cells/mm3), and his HAART included lamivudine, a drug associated with myelosuppression, 25 all factors that may explain his severe neutropenia.
Although the periodontopathic bacterial infection necrotizing periodontal disease is not uncommon in HIV-seropositive subjects, 4 –7 there are only isolated reports of necrotizing periodontal disease in HIV-seropositive subjects with severe neutropenia. 27 In a study investigating the relationship between HIV-associated oral lesions and hematological values, Patton reported that both nonspecific oral ulcers and necrotizing gingivitis/necrotizing periodontitis are about twice as likely to occur in neutropenic HIV-seropositive subjects as in HIV-seropositive subjects without neutropenia. 27 However, the prevalence of these oral lesions in the study population was too low for a significant relationship to be established, so the findings should be interpreted with caution.
In conclusion, nonspecific oral ulcers in neutropenic HIV-seropositive subjects should be regarded and treated as neutropenic ulcers. The term nonspecific oral ulcers (not otherwise specified) should be restricted to those ulcers with nonspecific histopathological features in which microbiological agents cannot be identified, and that are not associated with iron, folic acid, and vitamin B deficiencies or with neutropenia.
Comments
Posttreatment laboratory reports were not obtained because the patient could not be persuaded to have further tests done to determine either his neutrophil count after the administration of G-CSF, or his CD4+ T cell count, or his HIV viral load after HAART.
Therefore though it is highly probable that there was an improvement in the neutrophil count associated with resolution of the neutropenic ulcers, proof of this was lacking; likewise, because there was no evidence of immune reconstitution, discussion of nonspecific oral ulcers as an IRIS phenomenon is entirely academic.
It would have been desirable to have had the results of a PCR investigation for possible CMV or HSV DNA in the ulcers, to have obtained neutrophil counts at several stages during the progression of the case, to have had the services of a hematologist to investigate other possible causes of neutropenia, and to have had an endoscopic examination to exclude other gastrointestinal ulcers. However, in the semirural South African context in which the medical capacity for such extensive investigations to satisfy “ideals” of diagnostic thoroughness is very limited, and where the possibilities of such investigations are even further limited by the lack of cooperation of relatively unsophisticated patients, it is often necessary to make a diagnosis, to prescribe treatment, and to interpret the outcomes on whatever information is available.
Despite these limitations, we emphasize the need to investigate the possibility that neutropenia may be the cause of nonspecific oral ulcers in HIV-seropositive subjects. Therefore reports in the dental literature dealing with nonspecific oral ulcers in HIV-seropositive subjects in whom an investigation for neutropenia was not done must be interpreted with caution.
Footnotes
Author Disclosure Statement
No competing financial interests exist.