
Abstract
Endothelial progenitor cells (EPC) and circulating endothelial cells (CEC) have recently been considered as biomarkers of cardiovascular risk (CVDR) in healthy subjects. The impact of HIV infection on these cells is not well known.
A case-control study was conducted in 15 antiretroviral-naive HIV+ patients and 15 HIV-negative controls. The quantitative profile of CEC and EPC differed significantly in HIV+ and HIV– subjects. HIV+ subjects had significantly more CEC and less EPC than HIV– controls. A quantitative impairment in the balance of the CEC and EPC might contribute to the increased subclinical CVDR in HIV+ patients.
C
In 1997 Asahara et al. identified a subset of cells in the peripheral blood named endothelial progenitor cells (EPC) involved in the renewal of the vascular endothelium. 3 Studies in HIV– persons have demonstrated an inverse association between the amount of EPC and CVDR. 4 In contrast, circulating endothelial cells (CEC) are mature endothelial cells discarded from the endothelium in response to endothelial damage. 5 Increased levels of CEC have been associated with increased endothelial dysfunction markers and with abnormal low-flow-mediated dilatation. 6 Thus, while EPC are associated with protection from CVD, CEC reflect endothelial damage and increased CVDR.
The impact of HIV infection on both EPC and CEC is not well known. Abnormal endothelial repair by EPC and/or an increased number of CEC accompanying endothelial injury might contribute to the accelerated course of CVD seen in HIV-infected patients.
To determine if HIV infection modifies the amount of EPC and CEC, we undertook a case-control, cross-sectional study in which 15 antiretroviral-naive HIV-infected individuals were compared to 15 HIV– persons matched for age, gender, and smoking status. Written informed consent for the examinations conducted in the study was obtained from all individuals, and the study protocol was evaluated and approved by the hospital Ethics Committee.
The 10-year CVDR was calculated using Framingham, SCORE, and REGICOR algorithms. 7 Individuals were classified as follows: (1) high CVDR, if >10% with Framingham and REGICOR or >5% with SCORE, (2) moderate CVDR, if 5– 9.9% with Framingham and REGICOR or 3–4.9% with SCORE, and (3) low CVDR, if <5% with Framingham and REGICOR or <3% with SCORE.
Levels of EPC and CEC were immediately measured by multiparametric flow cytometry in freshly isolated peripheral blood mononuclear cells (PBMCs) using Ficoll-Hypaque (Sigma Chemical Co., St. Louis, MO). The following monoclonal antibodies were used in the flow cytometry analysis using an FC 500 cytometer (Beckman Coulter): anti-CD45-ECD, anti-CD31-FITC (Beckman Coulter), anti-CD34-PECY7, anti-CD133-PE (eBioscience), and CD309-PerCP/Cy5.5 (BioLegend). 8 EPC were defined as %CD45dimCD34+CD31+CD133+CD309+ cells and CEC as %CD45–CD34+CD31+CD133– cells. Late EPC (%CD45dimCD34+CD31+CD133–) and immature CEC (%CD45–CD34+CD31+CD133+) were similarly measured. Figure 1 shows the gating strategy.
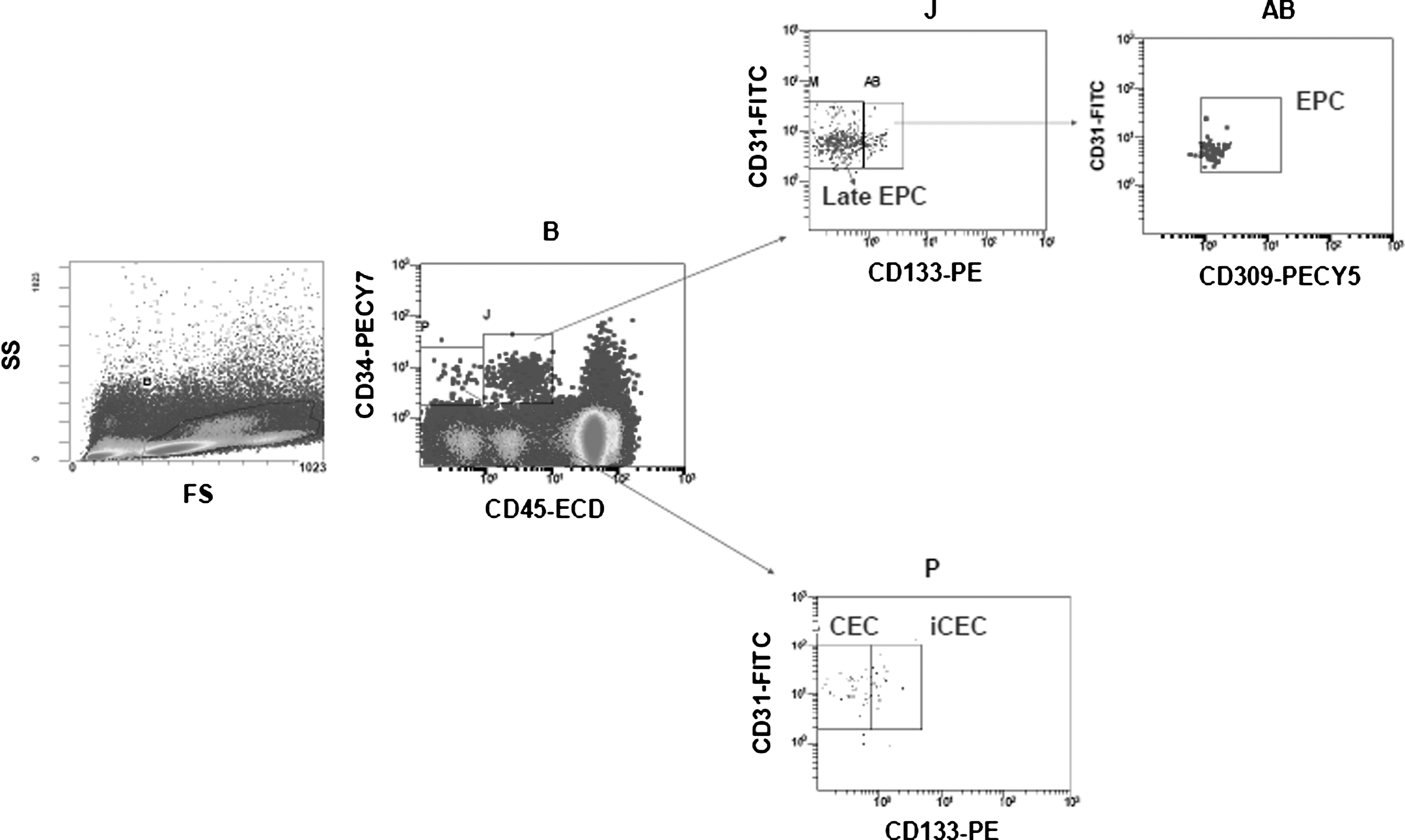
Detection of endothelial progenitor cells (EPC), late EPC, circulating endothelial cells (CEC), and immature CEC using multiparametric flow cytometry. Peripheral blood mononuclear cells (PBMCs) were stained with CD45-ECD, CD31-FITC, CD34-PECY7, CD133-PE, and CD309-PECY5. Forward and side scatter plot with gate for viable PBMCs (B). Viable cells assessed for CD45-ECD and CD34-PECY7 staining. CD45dimCD34+ cells (J) were then assessed for CD31-FITC and CD133-PE and CD45dimCD34+CD31+CD133– were defined as late EPC (M). CD45dimCD34+CD31+CD133+ cells (AB) were then assessed for CD309-PECY5 and CD45dimCD34+CD31+CD133+CD309+ were defined as EPC. CD45–CD34+ cells (P) were then assessed for CD31-FITC and CD133-PE and CD45–CD34+CD31+CD133– were defined as CEC and CD45–CD34+CD31+CD133+ as immature CEC (iCEC).
Differences between groups were assessed using nonparametric tests and associations with different variables were tested using Spearman correlations. All parameters were expressed as median (IQR) values.
The median age of HIV-infected individuals and controls was 29 (13) years and 27 (10) years. Overall, 93% were males and 16% were smokers. HIV-infected patients showed a length of infection of 10 (27) months, CD4 counts of 359 (145) cells/μl, and viral load of 4.38 (1.14) log HIV-RNA copies/ml. HIV-infected individuals had lower levels of HDL-cholesterol than controls [29 (14) vs. 41 (19) mg/dl; p=0.002] and a lower number of platelets [177,000 (58,000) vs. 252,000 (95,000) platelets/μl; p=0.008]. Although controls showed higher levels of total cholesterol compared to HIV-infected patients [171(48) vs. 155 (36) mg/dl; p=0.043), CVDR scores showed similar low risk values in both groups. No significant differences were observed in levels of LDL-cholesterol, VLDL-cholesterol, triglycerides, and glucose between both groups.
As shown in Fig. 2, CEC and EPC levels differed significantly according to HIV status. The CEC level was higher in HIV-infected patients than in controls [0.042% (0.027%) vs. 0.016% (0.011%); p=0.007]. However, HIV-infected individuals had lower EPC numbers than controls [0.002% (0.003%) vs. 0.009% (0.009%); p=0.002]. As expected, the vascular index defined as the CEC/EPC ratio was increased in HIV-infected patients [12 (15) vs. 2(3); p<0.0001]. Numbers of late EPC and immature CEC were similar in both groups. Moreover, no significant correlation was found between EPC and CEC in HIV-infected patients. Finally, no association was observed between EPC and/or CEC and CD4 counts, plasma HIV-RNA, and biochemical parameters.
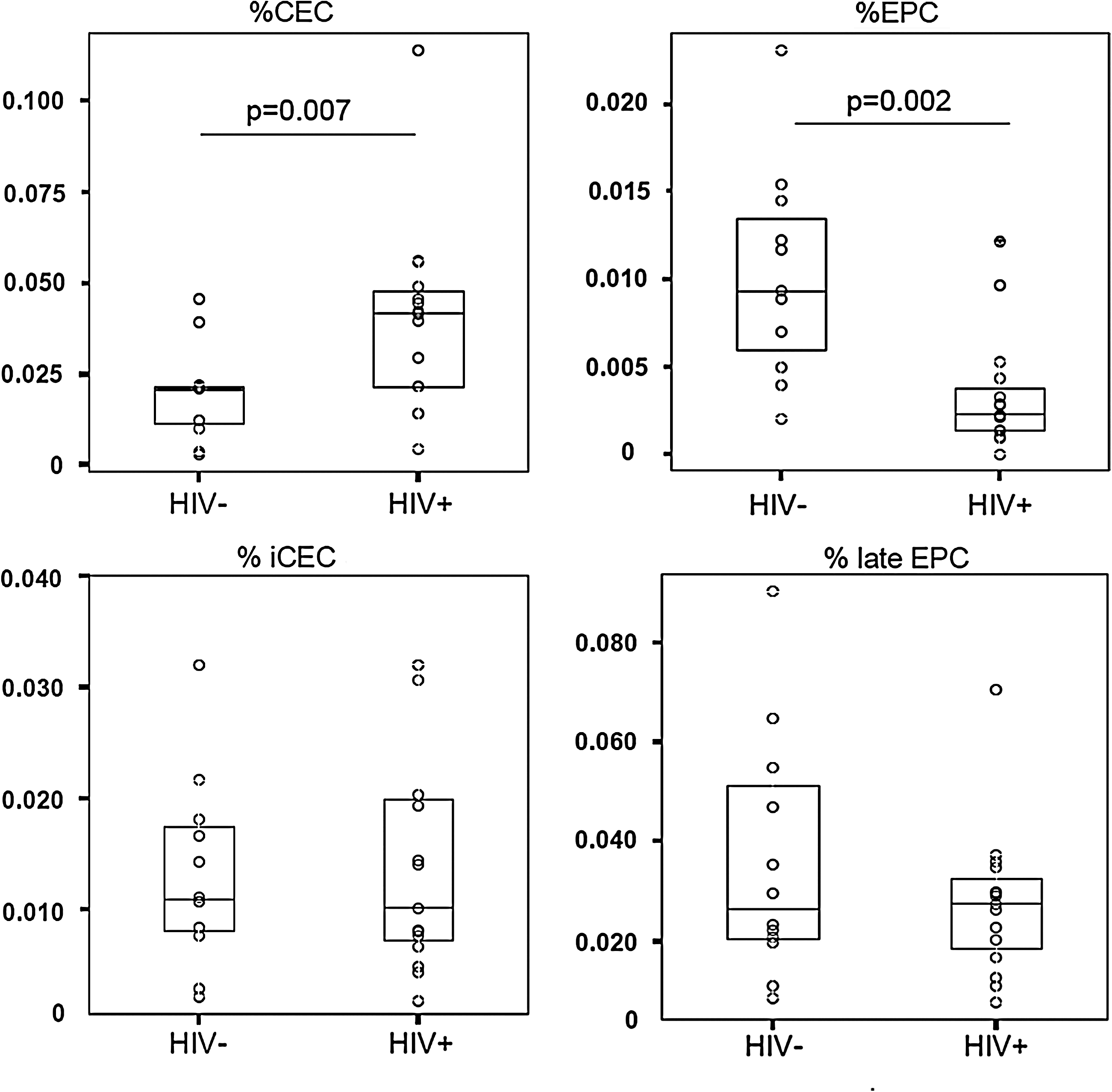
Levels of CEC, EPC, iCEC, and late EPC in HIV-infected patients and matched healthy controls.
HIV induces a prothrombotic state and proinflammatory phenomena in the vascular endothelium that may contribute to the increased CVDR seen in HIV-infected individuals. 7 High HIV viremia has been associated with endothelial dysfunction, which is a traditional CVDR for atherosclerosis. 9,10 In our study, HIV-infected patients showed lower HDL-cholesterol levels than controls, which might partially account for their increased CVDR. 11 In this setting, the presence of an unprotective mechanism involving high endothelial damage mediated by increased CEC levels might then potentiate the CVDR.
In normal conditions, EPC increases following any episode of endothelial injury in an attempt to repair the vascular endothelium. In our study, young HIV-infected patients with low CVDR had significantly lower EPC numbers than controls with similar age and CVDR factors. As a consequence, the endothelial dysfunction observed in HIV-infected individuals might result from more pronounced vascular damage due to the absence or limited activity of the restoration mechanisms. This link between EPC deficiency and CVDR has already been well documented in HIV– individuals with distinct degrees of atherosclerosis.
The amount of EPC inversely correlates with the number of CVDR factors in coronary artery disease (CAD). 4 In this regard, EPC constitute a surrogate marker of cumulative CVDR. As EPC are key determinants of endothelial dysfunction, 12 their number predicts vascular disease earlier and more accurately than traditional CVDR. Accordingly, a study assessed the prognostic value of EPC in patients with CAD followed for 1 year and showed that the cumulative event-free survival rate was directly associated with baseline EPC numbers. 13 Hypothetically, the protective mechanism driven by EPC that halts the development of atherosclerosis is probably limited or absent in HIV infection.
A recent study has shown that circulating-colony-forming unit endothelial cells (CFU-EC) may be infected by HIV. 14 Despite the lack of consensus regarding the phenotypic and functional profile of EPC, it might be that EPC are a subset of CFU-EC. Hence, direct infection of EPC by HIV might result in a lower number of these cells. In support of this, a recent study has reported a higher number of EPC in HIV-infected patients on highly active antiretroviral therapy (HAART) than in healthy subjects. 15 Future research must address the comparison of HIV-infected patients with and without HAART, and longitudinal studies examining the impact of HAART on the profile of EPC are warranted.
In summary, uncontrolled HIV infection is associated with a reduction of cells involved in the restoration of the vascular endothelium and an increase in cells associated with endothelial damage. A quantitative impairment in the CEC and EPC balance (damage/repair of the vascular endothelium) might contribute to the increased subclinical CVDR characteristically seen in HIV-infected patients.
Footnotes
Acknowledgments
This work was supported in part by grants from FIPSE, Foundation IES, FIS (ISCIII-RETIC RD06/006), and the European Union 6th Framework programme (NEAT, number: LSHP-CT-2006-037570). Some of the data was presented as Poster 259 at the 17th Conference on Retroviruses and Opportunistic Infections (CROI), 2011 February 27–March 2, Boston, MA.
Author Disclosure Statement
No competing financial interests exist.