
Abstract
Perinatal antiretroviral (ARV) exposure has been related to hyperlactatemia and lactic acidosis in infants born to HIV-infected mothers. Our objective was to determine the incidence of these conditions during the first year of life in uninfected infants born to HIV-infected mothers and compare the data with infants born to mothers with hepatitis C virus (HCV) infection. We investigated the relationships between hyperlactatemia and neurological and neurodevelopmental disorders by conducting a prospective, comparative cohort study (October 2004 to October 2007) consecutively including children of HIV- and HCV-infected mothers. Liver enzymes, pH, lactic acid, and plasma amino acids were determined at 1.5, 3, 6, and 12 months of life. Pathological hyperlactatemia was defined as lactate >2.1 mmol/liter together with alanine >475 μmol/liter. Seventy-nine patients (39 HIV-exposed patients and 40 unexposed patients) were included. Baseline maternal characteristics in the two groups were similar. Almost 90% of HIV-infected mothers received HAART during gestation, while 10.3% were given AZT monotherapy. Eight newborns received combined therapy and 31 received AZT-based monotherapy. Twelve patients (five exposed and seven nonexposed) had some neurological disorder, and four other patients (one vs. three) showed signs of neurodevelopmental delay, with no significant differences between the groups (p=0.34). Pathological hyperlactatemia was detected in 56.4% (95% CI 39.6–72.2) and 57.5% (95% CI 40.9–73.0) of patients, respectively (p=0.92), and this condition was more frequent in preterm children (p<0.05). ARV use during pregnancy and the neonatal period was not associated with pathological hyperlactatemia. The presence of hyperlactatemia was not associated with neurological or neurodevelopmental disorders. No association was established between the use of ARV agents and the development of hyperlactatemia or neurological disorders in HIV-exposed children during their first year of life.
Introduction
S
ARV administration to pregnant women and their newborns has generated doubts about the safety of these drugs. An association between ARV exposure and hyperlactatemia (sometimes symptomatic) and lactic acidosis has been extensively reported in these patients, 3,4 as well as cases of severe neurological involvement and death, 5 although this has not been confirmed by other groups. 6,7 Damage to mitochondrial DNA polymerase gamma resulting from antiretroviral treatment with nucleoside or nucleotide reverse transcriptase inhibitors (NRTI/NtRTI) is a proposed cause of the hyperlactatemia occurring in exposed infants. 8 –13 However, many of these studies are subject to methodological bias that could affect the results. The present study endeavors to obtain more realistic data on the incidence of hyperlactatemia in this population by controlling most of the confounding factors.
The objectives of this study are the following: (1) to establish the incidence of hyperlactatemia, lactic acidosis, and associated neurological symptoms during the first year of life in uninfected infants born to HIV-infected mothers and a comparison group of uninfected infants born to hepatitis C virus (HCV)-infected mothers, and (2) to determine factors associated with the presence of hyperlactatemia and neurological and neurodevelopmental disorders in these patients.
Materials and Methods
This is a prospective, comparative cohort study conducted at a pediatric referral hospital in Barcelona (Spain) that included an expected 40-patient sample in each group and 320 blood samples (160 per group). From October 2004 to October 2007, we consecutively included all HIV-uninfected children born to HIV-infected mothers in our center (exposed cohort). Vertical HIV transmission was excluded by complying with current international recommendations, and seroreversion was subsequently confirmed when infants were 18 to 24 months of age. Since children born to HCV-infected mothers in our center have similar demographic and clinical features, this patient group was used for comparison (nonexposed cohort), undergoing the same clinical protocol and analytical follow-up.
Laboratory testing to determine liver enzymes, pH, lactic acid, alanine, and the remaining plasma amino acids was performed at 1.5, 3, 6, and 12 months of life in all infants. The sample was immediately sent, at room temperature, to the metabolic diseases laboratory, where it was processed without further delay. Extracted blood was deproteinized in situ with 5% perchloric acid, intense agitation, and centrifugation at 4°C. The supernatant, once neutralized at pH 7.0 with phosphate buffer, was analyzed by enzymatic analysis in a semiautomatic analyzer Cobas Mira with a commercial kit (Roche, Basel, Switzerland). Hyperlactatemia was considered pathological when plasma lactate plus alanine values were greater than 2.1 mmol/liter and 475 μmol/liter, respectively, in any of the analyses. Clinical examination, anthropometric measurements, and neurological assessment were performed by experienced pediatricians as per daily clinical practice at the same time points.
Statistical comparison of the data between cohorts was performed with the Mann–Whitney U test or chi-square test, where appropriate. Statistical significance was set at p<0.05. All calculations were carried out with SPSS, version 15.0 (SPSS, Inc., Chicago, IL).
The study was approved by the local Ethics Committee and informed consent to participate was obtained from all parents or guardians.
Results
Seventy-nine patients comprised the final study group (39 patients in the HIV-exposed cohort and 40 in the nonexposed cohort). One exposed child was excluded because of a mitochondria-unrelated cause of death (congenital diaphragmatic hernia).
No significant demographic differences were observed between the mothers in the two groups (Table 1). Drug abuse during gestation was evidenced in up to 25% of mothers, although this datum was not systematically collected, and multiple drug abuse was common, with no significant differences between groups. Fifteen of the 39 HIV-infected mothers (38.5%) were coinfected with HCV, and one mother from the nonexposed cohort was infected with hepatitis B virus (HBV).
Median value (interquartile range).
HAART, highly active antiretroviral therapy; PI, protease inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; AZT, zidovudine; d4T, stavudine; HBV, hepatitis B virus; HCV, hepatitis C virus.
Almost 90% of the HIV-infected group had received HAART during pregnancy [in 40%, a zidovudine (AZT)/ lamivudine (3TC)/nevirapine (NVP) combination] whereas 10.3% received AZT-based monotherapy (Table 1). Among the mothers who were treated with NRTIs, more than 70% received thymidine analogues (AZT 60% and stavudine 11%). The length of maternal ARV therapy was not systematically recorded during pregnancy. Viral load (VL) nearest to labor was undetectable in only 54% of mothers, but most of the others had low-grade VL values that were not greater than 10,000 copies/ml: median VL in these patients was 1600 copies/ml (interquartile range, 925–37,500).
Most pregnancies in both groups were full term, with a median duration of 38 weeks (IQR 36.2–39.3), and a small but significant statistical difference (38.0 vs. 38.8 weeks, respectively, p<0.05) (Table 1).
The neonatal characteristics showed a slight predominance of girls, and birth weight greater than 2500 g, with no differences between the groups (2750 g exposed vs. 3020 g nonexposed; p=0.13) (Table 1). Thirty-one newborns from the exposed group received AZT monotherapy and eight received combined therapy based on AZT, 3TC, and NVP. Neonatal prophylaxis lasted for 6 weeks in all cases (3TC and NVP were stopped 2 weeks after birth). Although median body weight, body length, and head circumference of patients in both groups were slightly below those corresponding to our general population at an equivalent age, the values were within the normal range. Head circumference values at 6 and 12 months were normal in both the exposed and nonexposed groups.
Twelve patients (five exposed and seven nonexposed; p=0.49) showed some type of neurological disorder, mainly lower limb hypertonia that spontaneously resolved as they grew older (Table 2). Almost all patients presented other risk factors that could potentially explain neurological impairment (mainly prematurity and mother's drug abuse during pregnancy). Only four patients (one exposed and three nonexposed) presented persistent sequelae at the age of 12 months and, again, these could be attributed to the mother's drug abuse 3 and neonatal asphyxia. 1
Four patients (one exposed and three nonexposed) showed some neurodevelopmental delay, with no significant differences between the groups (p=0.34).
Of the 316 metabolic studies in prospect, complete results were obtained in 246 (77.8%). An increase in lactate greater than 2.1 mmol/liter in at least one analysis was found in 91% of patients (72/79). This figure dropped to 57% (45/79) when hyperlactatemia was accompanied by a rise in plasma alanine greater than 475 μmol/liter within the same determination. The incidence of direct signs of hepatic involvement (rise in liver enzymes greater than twice the upper limit of normal) and indirect signs (combined rise of methionine and tyrosine) was not significantly different between the groups, except in the first month when the incidence of elevated liver enzymes was higher in the exposed group (p<0.05). These findings were not associated with the presence of hyperlactatemia as a possible marker of hepatic involvement resulting from mitochondrial damage in either group.
Twenty-two exposed patients (56.4%, 95% CI 39.6–72.2) and 23 comparison patients (57.5%, 95% CI 40.9–73.0) had hyperlactatemia (p=0.92). Although both groups showed a trend toward spontaneous normalization, significant differences were seen in the temporal distribution of abnormal lactate results, which were more frequent in the exposed group at 1 month of life (p<0.05) and in the comparison group at 12 months (p<0.05) (Fig. 1). At the age of 12 months, 24% of patients still presented pathological hyperlactatemia. No significant differences were observed at 3 and 6 months (p=0.17 and p=0.42, respectively). No cases of lactic acidosis were detected.
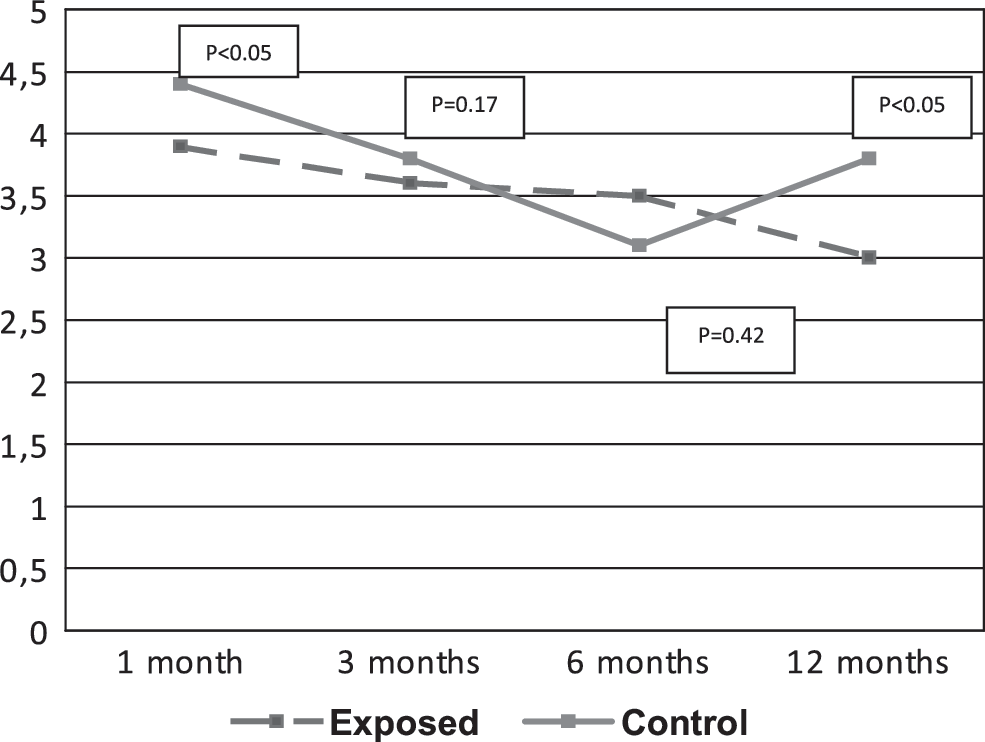
Evolution of median lactic acid values over time in patients with hyperlactatemia and hyperalaninemia in the HIV-exposed and nonexposed cohorts.
Among the variables studied, only prematurity was associated with hyperlactatemia (Table 3). HAART use during pregnancy, ARV class, AIDS diagnosis in pregnant mothers, prelabor CD4+ lymphocyte count and VL, and ARV administration in newborns during the first 6 weeks of life were not significant risk factors for the presence of hyperlactatemia (Table 4). To note, ARV use during pregnancy and after birth was significantly related to the presence of hyperlactatemia at 1 month of life (p<0.05) but not thereafter. There were no significant differences in the frequency of hyperlactatemia between infants born to HIV-infected mothers with an undetectable prelabor VL (12/21) and those born to mothers with detectable VL (10/15) (57.0% vs. 67.0%, respectively; p=0.55). A higher frequency of hyperlactatemia was found in patients with no neurological disorders (p<0.05). Furthermore, none of the patients with neurological manifestations or neurodevelopmental delay showed persistent hyperlactatemia. At preseny, the median age of the children included in this study is 4.7 years, and all are alive.
Median value (interquartile range).
HAART, highly active antiretroviral therapy; NRTI, nucleoside reverse transcriptase inhibitor; AZT, zidovudine; d4T, stavudine; 3TC, lamivudine; NVP, nevirapine.
Discussion
The results of this study show a significant incidence of asymptomatic hyperlactatemia over the first year of life in two cohorts of infants, one group born to HIV-infected mothers and another to HCV-infected mothers who had similar demographic and clinical characteristics with the exception of exposure to HIV and ARV therapy. Among the factors studied, a statistically significant relationship with hyperlactatemia was found only for premature birth; there were no significant associations with factors related to HIV and ARV therapy.
The epidemiological data of the mothers in the present study were similar to the characteristics of women included in larger cohorts in studies performed within our country and in other geographic areas. 3,4,14,15 Among the data obtained, those concerning drug abuse during pregnancy should be analyzed with caution, as the information on this factor was not obtained by systematic screening, but by questioning the mother, by detection of toxic substances in the mother's or newborn's urine when drug abuse is suspected, or by withdrawal syndrome in the newborn. Therefore, it is likely that drug abuse during pregnancy is underestimated in these at-risk populations, as has been reported, and the prevalence is higher than the rate in the general population of women of reproductive age. 16
The characteristics of HIV infection and ARV treatment in the mothers of exposed newborns were similar to those reported in previous studies in which most of the combined ARV regimens included NRTIs, mainly AZT in conjunction with 3TC, 3,4,15 as in the present study. The neonatal data are also comparable to those recently published in our country on the FIPSE cohort in Madrid, 15 and data reported by the European group in 2003. 17
There were no differences between the exposed and comparison group with regard to neurological manifestations. However, the percentage of newborns with some neurological symptom was high in both groups (12.5% in the exposed group and 17.5% in the nonexposed group). In a study performed in Brazil including 83 HIV-exposed newborns, Bruck et al. 18 reported minor neurological alterations in 55%. It may be that the stricter follow-up used in these children leads to detection of a higher number of transient disorders than in the general population. Furthermore, it should be borne in mind that in our study all but two cases presented risk factors unrelated to HIV or ARV, mainly drug abuse during pregnancy and preterm birth. Of note, in contrast to the study by Landreau-Mascaró et al., 19 in which seizures were cataloged as a possible sign of mitochondrial toxicity, none of our patients showed symptoms of epilepsy.
Although most of the neurological manifestations in our population were transient, four patients showed a significant psychomotor delay at 1 year of life, and three of them still present sequelae at present. In these cases, however, other risk factors unrelated to HIV or ARV were also present, including multiple drug abuse in three patients and neonatal asphyxia in one, which could potentially explain these manifestations. Because other factors that could explain psychomotor delay were present and there was no persistent hyperlactatemia, it is unlikely that mitochondrial damage played a part in the psychomotor delay seen in these patients.
In a recent large study in 1840 children of HIV-infected mothers in the United States, no significant neurodevelopmental disorders were associated with ARV treatment at 2 years of life, as evaluated with the Bayley scale for assessing infant neurodevelopment (BSID). 20 Smaller studies, such as one by Alimenti et al. 21 in 2006, have described poorer outcomes in exposed children, but the differences disappeared when results were corrected according to intrauterine exposure to toxic substances related to drug abuse.
Regarding the presence of hyperlactatemia and its possible correlation with risk factors, it is necessary to initially assess the study procedures. Plasma lactate determination is a validated technique for screening that shows a good correlation with mitochondrial DNA involvement, 22,23 and it is a routine test in our center. Alanine determination adds reliability to the diagnosis of persistent hyperlactatemia, and rules out false-positive results caused by extraction techniques, sample management, or the child crying, which are common in daily clinical practice, especially in younger children. 24 Thus, among the 91% of samples with elevated plasma lactate levels, 57% showed both hyperlactatemia and concomitant hyperalaninemia, with no differences between the groups. These data differ from those of Noguera et al., 3 in which hyperlactatemia without hyperalaninemia was rare, although many samples were excluded because of inadequate extraction/processing; nonetheless, we cannot explain the differences with respect to our results. Our data do coincide with the data of Noguera in the progressive drop in mean lactic acid values recorded over the first year of life in the exposed cohort.
Since the study by Blanche et al. in 1999, 5 several reports have described hyperlactatemia as a marker of mitochondrial damage in HIV-exposed children, whereas the data concerning its consequences are inconclusive. In more recent studies from the French cohort, 25,26 two groups of mitochondrial involvement are described: time-persistent asymptomatic self-limited hyperlactatemia without neurological consequences, occurring in around a third of ARV-exposed children born to HIV mothers, and symptomatic hyperlactatemia with associated neurological manifestations of varying severity with an incidence of 0.3–0.5%. Of course, the size of our HIV sample would be too small to manifest this very low incidence of symptomatic cases (assuming it is correct); thus we cannot offer any discussion on these findings. Other studies conducted in the United States, Europe, and Thailand 3,4,27 –34 have questioned this association, or shown a much weaker association with neurological manifestations than the French studies. Nevertheless, since diagnosing mitochondrial disorders is often difficult, these conclusions should be interpreted with caution. What seems evident is the capability of ARV drugs, especially thymidine analogs, to deplete mitochondrial DNA. 35 –38
In around half the patients in our study, at least one blood test showed hyperlactatemia with hyperalaninemia, with no differences between the two cohorts. The distribution of data regarding the emergence of hyperlactatemia varied over time, describing a descending curve in the course of months in the exposed cohort and a flat curve in the comparison cohort (Fig. 1). These results may have a temporal relationship with ARV exposure in the exposed cohort and are similar to those reported by Noguera et al. 3 and Giaquinto et al. 32 The results of Alimenti et al., 4 who provide information on newborns only up to 4 months of life, show a tendency similar to that seen in our series. However, Poirier et al. 39 reported persistent mitochondrial DNA depletion up to one year of life.
As to the risk factors related to hyperlactatemia, a statistically significant association was only established with prematurity, in contrast to the findings of other studies. 3,4 Even though it is frequently considered an excellent marker of tissue damage during the neonatal period, we did not find any reference to hyperlactatemia in premature infants who did not experience fetal suffering or sepsis in the literature, either in the HIV or seronegative population.
None of the factors related to HIV and ARV treatment was statistically associated with hyperlactatemia in the exposed cohort. These data are consistent with those reported by Alimenti et al., 4 but not with Noguera's results, 3 in which an association was established between emergence of hyperlactatemia and the use of NRTI during pregnancy, in particular didanosine (ddI). The virtual absence of pregnant patients treated with ddl in our cohort (1/39) obviates assessment of a potential relationship between the use of this treatment and emergence of hyperlactatemia. Nevertheless, the actual relationship with the use of ARV during pregnancy and after birth with the presence of hyperlactatemia at one month of life may be explained by a more recent exposure to antiretroviral therapy that no longer persists thereafter, as stated by Noguera et al. 3
As to the presence of hyperlactatemia and the development of neurological complications, there was an unexpected, higher incidence of hyperlactatemia in patients without neurological manifestations, in contrast to the data from the French group. 5,25,26 As was mentioned above, none of the patients exhibiting neurological signs or psychomotor delay had persistent hyperlactatemia. Furthermore, none of our patients presented lactic acidosis, although the low incidence of this complication and the small sample may limit the value of this finding.
There are several limitations in our study. The first is the small sample size, which did not allow detection of severe symptomatic hyperlactatemia cases, as those defined by the French cohort. Nonetheless, we consider that the absence of differences in the baseline data relative to larger cohorts supports the validity of the results. The second is the lack of data on the length of ARV therapy during pregnancy, above all considering the significant number of mothers who did not achieve undetectable VL before delivery. However, the fact that there were no differences in the incidence of hyperlactatemia between the group of children born to mothers with undetectable peripartum VL (which could suggest constant, continuous ARV exposure), and those born to mothers with a detectable viral load (possibly associated with shorter duration of ARV exposure or less rigorous adherence to ARV therapy), limits the bias posed by this lack of data when interpreting the results. Third, mitochondrial DNA was not studied in conjunction with lactate and alanine findings, although it might have provided additional information. This point remains inconclusive, however, because the utility of DNA determination to screen for mitochondrial disorder in this population is controversial. 40,41 A strong point of the study is the fact that a comparison group was included, in which mothers had similar epidemiological and obstetric features, neonatal characteristics were comparable, and the follow-up study was identical.
Conclusions
The data provided by this study question the reported association between intrauterine, intrapartum, and postnatal use of ARV agents and the emergence of persistent hyperlactatemia and related neurological symptoms in HIV-exposed children. Only prematurity was independently associated with a higher incidence of hyperlactatemia in our cohort and ARV use showed only a transient relationship with the presence of hyperlactatemia that could not be demonstrated after the first month of life. We consider that a control group with comparable features should be used when interpreting data concerning mitochondrial damage in HIV-exposed children.
Footnotes
Acknowledgments
The authors thank Ana Alvarez for performing the blood tests and for taking care of the children and their families, and Celine Cavallo for English language assistance. This study was funded in part by the Foundation for AIDS Research and Prevention in Spain (FIPSE, Fundación para la Investigación y la Prevención del SIDA en España; 36721/08).
P.S.P. and A.M.N. participated in conducting the study and in writing and reviewing the manuscript, S.M. contributed to conducting the study and reviewing the manuscript, E.R. and J.A.A. performed all the metabolic studies and contributed to reviewing the manuscript, M.E. and C.F. reviewed the manuscript, and X.M.G. performed the statistical analysis and contributed to reviewing the manuscript. All the authors have read and approved the text submitted.
Author Disclosure Statement
No competing financial interests exist.