
Abstract
HIV genetic recombination and high mutation rate increase diversity allowing it to escape from host immune response or antiretroviral drugs. This diversity has enabled specific viral subtypes to be predominant in specific regions. To determine HIV-1 subtypes among seropositive antenatal clinic attendees in Kenya's North Rift Valley, a cross-sectional study was carried out on 116 HIV-1-positive blood samples. Proviral DNA was extracted from peripheral blood mononuclear cells by DNAzol lysis and ethanol precipitation. Polymerase chain reactions using specific primers for HIV-1 gag and population sequencing on resulting amplicons were carried out. Phylogenetic analysis revealed that 81 (70%) were subtype A1, 13 (11%) subtype D, 8 (7%) subtype C, 3 (3%) subtype A2, 1 (1%) subtype G, and 10 showed possible recombinants: 5 (4%) subtype A1D, 4 (3%) subtype A1C, and 1 (1%) subtype A2C. These data support the need to establish circulating subtypes for better evaluation of effective HIV diagnostic and treatment options in Kenya.
G
Recent advances in automated sequencing have led to the rapid determination of HIV subtypes. This diversity arises from high mutation rates combined with extensive recombination leading to the production of new quasispecies and unclassified sequences on a daily basis. 7,8 The most robust way of assigning a subtype to an unknown sequence is through phylogenetic analysis. The aim of this study was to determine HIV-1 subtypes among antenatal clinic attendees in three hospitals of Kenya's North Rift Valley based on HIV-1 gag sequences.
Patients in this study comprised antiretroviral treatment-naive antenatal clinic attendees from three district hospitals in Kenya's North Rift Valley who were offered single dose nevirapine (sdNVP) for prevention of mother-to-child transmission of HIV. The study participants have been previously described. 9,10 Informed consent was obtained from all the women enrolled in the study. Blood was collected in 5-ml EDTA tubes and separated into plasma and lymphocytes using Ficoll-Paque Plus (Amersham Biosciences, NJ). DNA was extracted from lymphocytes using DNAzol (GIBCO-BRL, Grand Island, NY) according to the manufacturer's protocol. 11
The HIV-1 portion corresponding to the region from amino acid 132 of p24 to amino acid 40 of p7 in the HXB2 was amplified by nested polymerase chain reaction (PCR) using primers H1G777, 5′-TCACCTAGAACTTTGAATGCATGGG-3′ (outer forward), and H1P202, 5′-CTAATACTGTATCATCTGCTCCTGT-3′ (outer reverse) in the first round and H1Gag1584, 5′-AAAGATGGATAATCCTGGG-3′ (inner forward) and g17, 5′-TCCACATTTCCAACAGCCCTTTTT-3′ (inner reverse) in the second round. PCR conditions used were 94°C for 2 min, 35 cycles consisting of 94°C for 30 s, 50°C for 30 s, and 72°C for 1 min 30 s, with a final extension at 72°C for 7 min in the first round; and 94°C for 2 min, 35 cycles consisting of 94°C for 30 s, 50°C for 30 s, and 72°C for 1 min, with a final extension at 72°C for 7 min in the second round.
Population sequencing of the 460-bp gag gene fragment was done using Big Dye technology on ABI 310 (Applied Biosystems, Foster City, CA). Sequences were aligned with subtype reference sequences from the Los Alamos database (
One hundred and twenty-eight samples from pregnant women were collected. Amplification was successful in 116 samples (90.6%). Phylogenetic analysis of the 116 sequences revealed that 81 (70%) were subtype A1, 13 (11%) subtype D, 8 (7%) subtype C, 3 (3%) subtype A2, 1 (1%) subtype G, 5 (4%) subtype A1D, 4 (3%) subtype A1C, and 1 (1%) subtype A2C. Figure 1 shows the results of phylogenetic trees based on partial gag gene sequences from three districts in North Rift Valley, Kenya (Kapsabet, South Nandi Hills, and Kitale).
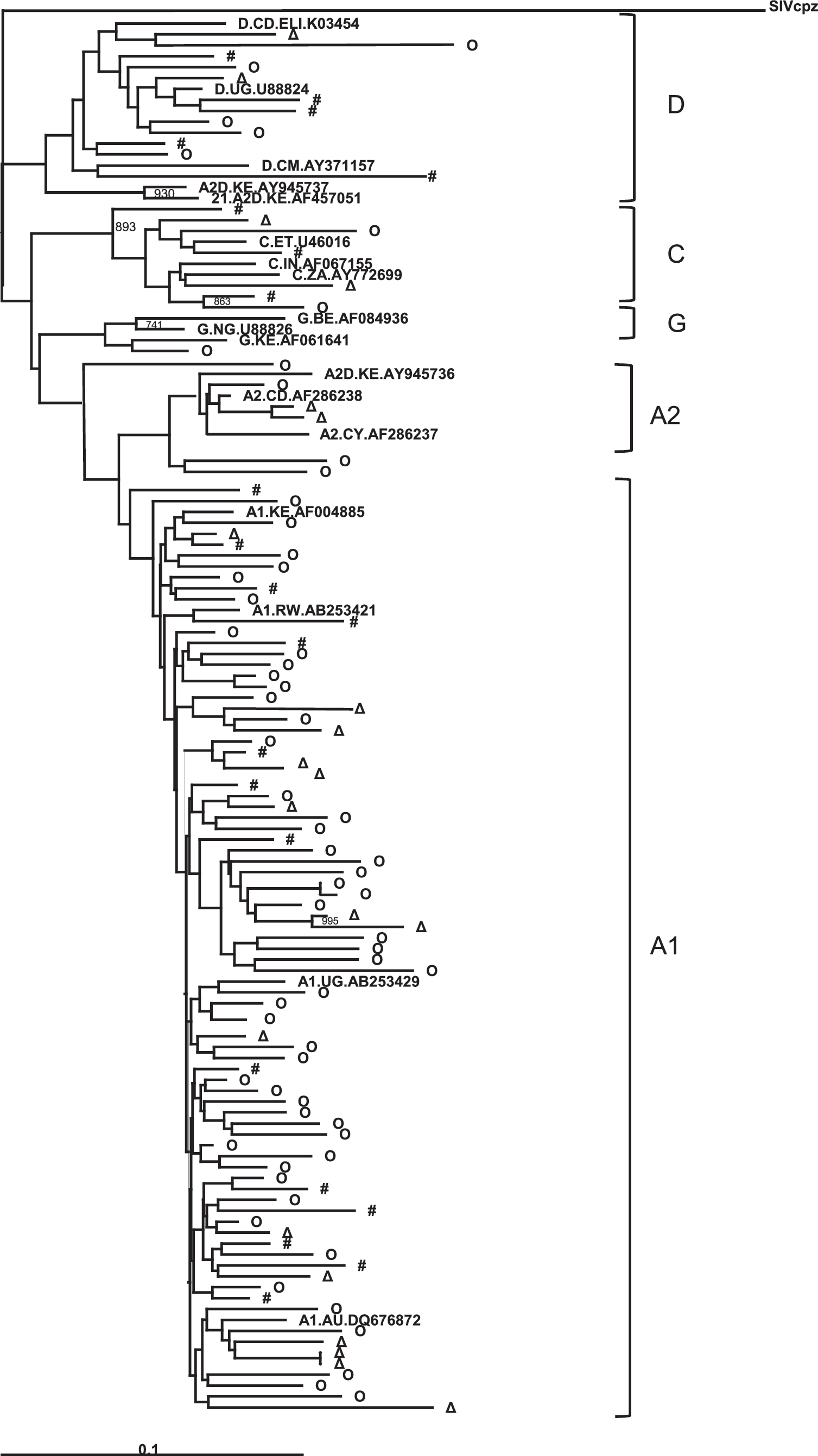
A phylogenetic tree showing diversity of HIV-1 gag sequences from North Rift Valley, Kenya. (
In this cross-sectional study, we established HIV-1 subtypes among antenatal clinic attendees in North Rift Valley based on gag sequencing. From our observation, most women were infected with HIV-1 subtype A1 followed by D, C, and possible recombinants. Previous studies have shown that HIV-1 subtype A1 is the most dominant virus in circulation in Kenya 13,14 and this study was consistent with that (Fig. 1). However, as seen from clustering in the phylogenetic trees, there was high diversity even within subtypes as demonstrated by low bootstrap values. This would indicate possible viral mixing and/or dual infections. This is being considered for further analysis.
As in other cross-sectional studies, this study had limitations. One, only positive samples were analyzed to determine subtypes in circulation; therefore we could not determine the site prevalence of HIV in the studied population. Two, only one region of HIV-1 was directly sequenced. We could not ascertain the exact prevalence of recombinants in our study population. As a result, it will be necessary to sequence larger portions of the virus to determine the scope of prevalent subtypes since what was done may have missed some mixed subtypes or recombinants. Furthermore, the sample size may have been too small to be generally accepted as the prevailing status of subtypes in the populous North Rift Valley region of Kenya. Nonetheless, this may be representative of prevalent subtypes in this region. Since HIV-1 treatment success partly depends on prevalent subtypes, this study adds to the existing knowledge of HIV-1 diversity, forms the basis upon which government intervention strategies should focus during the current upscaling of antiretroviral therapy, and provides information on circulating viral subtypes so that effective drugs can be administered to those who are infected.
Sequence Data
The nucleotide sequences reported in this study were deposited at the GenBank under accession numbers EU163589 - EU163704.
Footnotes
Acknowledgments
We give special thanks to Kitale, Kapsabet and South Nandi district hospital staff that helped in sample collection. We appreciate volunteers who generously donated samples for this work. We thank the director KEMRI for giving permission to publish this work.
Author Disclosure Statement
No competing financial interests exist.