
Abstract
Low bone mineral density (BMD) is common in HIV-infected patients. Bisphosphonates such as alendronate potently inhibit bone resorption and are effective against osteoporosis. The aim of the ANRS 120 Fosivir trial was to evaluate the effect of alendronate on low BMD in HIV-infected patients. HIV-1-infected adults with a t-score≤−2.5 at the lumbar spine and/or total hip, as assessed by dual x-ray absorptiometry, and no other known risk factors for low BMD, were randomized to receive either extended-release alendronate 70 mg weekly or placebo for 96 weeks, with stratification for gender. All the patients also received daily calcium carbonate (500 mg) and vitamin D (400 U). The primary endpoint for efficacy was the percentage change in BMD at the site with a t-score≤−2.5. Forty-four antiretroviral-treated patients (42 men, 2 women) were enrolled. The median age was 45 years, the median CD4 cell count was 422/mm3, and viral load was <400 copies/ml in 84% of patients. Baseline characteristics were well balanced between the alendronate (n=20) and placebo (n=24) groups. At baseline, 15 patients (75%) in the alendronate group and 17 patients (71%) in the placebo group had a t-score≤−2.5 at the lumbar spine. In the main analysis, BMD at the site with a t-score≤−2.5 increased by 7.1% and 1.0%, respectively, in the alendronate (n=14) and placebo (n=20) groups at week 96 [mean difference, 6.1% (95% CI 2.8 to 9.3); p=0.0003]. Alendronate 70 mg weekly for 96 weeks improves BMD in HIV-1-infected patients on antiretroviral therapy.
Introduction
Low bone mineral density (BMD, g/cm2) is a common metabolic complication of HIV infection. The reported prevalence rates of osteopenia and osteoporosis in HIV-infected men range from 23% to 65% and from 4% to 33%, respectively. 1 –5 A meta-analytic review 6 showed that, by comparison with uninfected controls, HIV-infected patients were 6.4 times more likely to have reduced BMD (95% CI 3.7, 11.3) and 3.7 times more likely to have osteoporosis (95% CI 2.3, 5.9). In HIV-infected women, low BMD seems to be a significant problem only after menopause. 7 The causes of low BMD in this setting probably include host factors, viral factors, and antiretroviral therapy. 8 Although an effect of antiretroviral drugs has been clearly shown in several trials, 9 most of the difference in BMD between HIV-infected and -uninfected subjects is explained by low body mass index (BMI) in the former population. 10
Loss of BMD is associated with an increased fracture risk in the general population 11 and several recent studies reported a significantly higher prevalence of fractures in HIV-infected patients relative to matched for age and sex non-HIV-infected individuals. 12 –15
Alendronate, a potent bisphosphonate that inhibits osteoclast-mediated bone resorption, 16 is approved for the treatment of osteoporosis in both men and women. 17 As the causes of low BMD in HIV-infected patients may differ from those in postmenopausal women, it is important to verify the effectiveness of this drug specifically in the HIV-infected population.
This placebo-controlled, double-blind trial was designed to examine the effect of alendronate on bone mineral density in HIV-infected patients with low BMD.
Materials and Methods
Study design
The randomized, multicenter, double-blind, placebo-controlled trial (ANRS 120-Fosivir; ClinicalTrials.gov identifier NCT00120757) was designed to assess the efficacy of alendronate given for 96 weeks to HIV-infected patients with a t-score≤−2.5. The primary endpoint was the percentage change in BMD at the site with a t-score≤−2.5, between baseline and week 96. Randomization was centralized and stratified by sex, with blocks of six, using the SAS PLAN procedure. The Pitié-Salpêtrière Hospital institutional review board approved the protocol and all the patients gave their written informed consent.
Intervention
The patients were randomly allocated to receive extended-release alendronate 70 mg weekly, or a matching placebo, for 96 weeks. A service company for pharmaceutical development of clinical trial supplies produced the GMP overencapsulated blinded capsules. Patients in both groups also received daily calcium carbonate 500 mg and vitamin D 400 IU, and ongoing antiretroviral therapy was continued unchanged when possible. These dosages were chosen because they correspond to those conventionally used in osteoporosis trials, and particularly in that of Orwoll. 18
Patients
Men and nonmenopausal women over 18 years of age were eligible for this study if they had tested positive for anti-HIV-1 antibodies, had been diagnosed with HIV infection at least 5 years previously or had a CD4 cell count nadir below 200/mm3, had a CD4 cell count above 50/mm3 at randomization, and had a t-score≤−2.5 at the lumbar spine or total hip, or a t-score≤−1 at the lumbar spine or total hip plus a history of osteoporotic vertebral fracture (vertebral height loss >20%).
Patients were not eligible if they had severe respiratory failure, chronic alcoholism, ongoing opportunistic infections, gastric ulcer or disorders interfering with esophageal motility in the previous 3 months, a history of malignancy in the previous 5 years (except for skin cancer or Kaposi's sarcoma), cytotoxic chemotherapy or cytokine therapy, liver cirrhosis, breast feeding, or pregnancy. Patients were also excluded if they had other known risk factors for low BMD, namely vitamin D deficiency (such patients could be randomized, without further screening, after receiving calcium and high-dose vitamin D for 1 month, that is at least 800 UI per day), renal failure, heart failure (NHYA class III or IV), glucocorticoid therapy at a dose of at least 0.5 mg/kg/day for 15 days or more during the previous 6 months; thyroid or other endocrine disorders if untreated for more than 6 months; hypercalciuria; and a body BMI of 18 kg/m2 or less. Patients with low testosterone levels warranting initiation of testosterone therapy, patients already on testosterone therapy, and patients previously treated for osteoporosis were also excluded.
Assessment of bone mineral density
BMD was assessed by means of DXA. All the scans were analyzed centrally, blindly to the study treatment. They were subjected to quality controls, and only scans that met the quality criteria were included. t-scores were calculated for each body site by using the appropriate reference curve for each device. The t-score is the difference between a patient's BMD and the mean BMD of peak bone mass for young adults, divided by the standard deviation (SD) in the appropriate gender group. The same DXA device was always used for a given patient. Quality controls were applied to each device to verify the absence of drift during the study period. As GE-Lunar (Madison, WI) and Hologic (Bedford, MA) DXA devices were used, standardized BMD values (sBMD, mg/cm2) were calculated with published formulas. 19
Monitoring
A two-step screening procedure was used. Patients who met the other inclusion criteria had a physical examination, CD4 cell count and plasma HIV-1 RNA assay, and their lumbar spine and total hip BMD values were determined by DXA less than 4 weeks before baseline. In patients with a t-score≤−2.5 either at lumbar spine and/or at hip, biochemistry, vitamin D, testosterone, parathyroid hormone (PTH), thyroid-stimulating hormone (TSH), urinary calcium, fasting serum crosslaps, and osteocalcin were determined locally less than 2 weeks before baseline.
After inclusion the patients had physical examinations at weeks 4, 12, 24, 36, 48, 72, and 96, and BMD was evaluated by DXA at weeks 48 and 96. Adverse events were recorded at each visit. CD4 cell counts and plasma HIV-1 RNA levels were determined at weeks 4, 12, 24, 36, 48, 72, and 96. Serum calcium, phosphorus, alkaline phosphatase, creatinine, aspartate transaminase (AST), and alanine transaminase (ALT) levels were determined at weeks 24, 48, 72, and 96. Fasting serum crosslaps and osteocalcin levels were determined at weeks 48 and 96.
Plasma HIV-1 RNA assay
Plasma HIV-1 RNA was measured with the Amplicor Monitor assay version 1.5 (Roche Diagnostics, Basel, Switzerland; detection limit 400 copies/ml), or with the bDNA assay version 3.0 (Bayer Healthcare Diagnostics Division, Puteaux, France; detection limit 50 copies/ml).
β-Crosslaps serum assay
Serum β-crosslaps or C-telopeptide of type I collagen (CTX) were determined with an Elecsys 2010 analyzer (Roche Diagnostics, Mannheim, Germany). Briefly, the serum sample (50 μl) and a biotinylated antibody specific for an epitope of an 8-amino-acid sequence of the C-terminal portion of the telopeptide EKAHD-β GGR were dispensed into a reaction cup and incubated at 37°C for 9 min. The ruthenium-labeled partner monoclonal antibody targeting the same epitope plus streptavidin-coated magnetic microparticles were added and incubated at 37°C for a further 9 min. The electrochemiluminescent signal generated by the ruthenium-labeled sandwich complex was then measured.
Statistical considerations
The sample size was calculated for men only (both men and women could be enrolled in the study) and randomization was stratified by sex. In the initial sample size calculations, we wanted to detect a smaller difference (3%) in the percentage change in BMD at the lumbar spine than that observed by Orwoll et al. (5%). 18 Forty-five patients per arm were required to detect a between-group absolute difference of 3%, assuming a standard deviation of 5% based on Orwoll's study, with a type I error of 0.05 and a power of 80% in a two-tailed test. However, after 16 months of screening, only 40 patients had been enrolled and the sample size was thus recalculated to detect a 5% difference, as in Orwoll's study at lumbar spine. The new sample size required 17 assessable patients per arm, and the scientific committee therefore decided to halt enrollments after inclusion of 25 patients per arm, to account for the dilution effect of nonassessable patients.
Variables were summarized by using proportions for categorical variables; the median and interquartile range (IQR) for age, time since diagnosis of HIV infection, the CD4 cell count, the CD4 cell count nadir, the number of previously received antiretroviral drugs, the time since initial antiretroviral therapy, the t-score, and biomarkers of bone turnover; and the mean and standard deviation (SD) for continuous variables used as endpoints, as in Orwoll's study. 18 The primary endpoint was the mean percentage change in BMD at the site with a t-score≤−2.5 on DXA at week 96 versus week 0. Secondary endpoints were the mean percentage change in BMD at the lumbar spine on DXA at week 96 versus week 0, and the mean percentage change in total hip BMD on DXA at week 96 versus week 0, analyzed with an intent-to-treat (ITT) approach on available data, called analysis on available data in the rest of the paper. To deal with missing data for the primary endpoint, sensitivity analyses were applied, using the last-observation-carried-forward method (LOCF), or imputation of the first quartile (Q1) or the third quartile (Q3), according to data safety and monitoring board (DSMB) recommendations, to enable full ITT analysis.
In addition, sensitivity analyses were performed using mixed linear models on all available measures obtained over the 2-year study period for BMD at the site with a t-score≤−2.5, as well as at the lumbar spine and hip. Mean changes in alkaline phosphatase, osteocalcin, and serum crosslaps levels at week 96 versus week 0 were compared, using the analysis on available data. In addition, all these endpoints were also evaluated at week 48 versus week 0. Changes from baseline were compared between the groups by using the nonparametric Mann–Whitney test. Finally, at week 96, we compared the proportions of patients in each group who had a change in BMD at lumbar spine and total hip exceeding the smallest detectable difference (SDD), taking into account the variability of the technique (0.034 g/cm2 and 0.027 g/cm2, respectively). 20 Fisher's exact test was used for these comparisons and also to compare both the proportions of patients who had fractures during the study period and the proportions of patients who experienced serious adverse events. SAS software version 9.1 (SAS Institute, Inc., Cary, NC) was used for all analyses.
Results
Patient disposition
Between January 2004 and October 2006, 1079 patients (237 women) were screened in 27 French centers and 49 patients were enrolled. Following presentation of the ACTG 5163 results, 21 the DSMB, created before the beginning of the trial, examined the results at week 48 in the two arms (arms A and B), and recommended to continue the trial. As no formal test was being performed at this stage, no adjustment for multiple analyses was accounted for in the final analysis. As shown in Fig. 1, 44 patients received at least one dose of study treatment and were included in the analyses. Before week 48, seven patients stopped treatment and follow-up and were therefore not evaluated by DXA at week 48: two patients in the alendronate arm and three in the placebo arm decided to stop follow-up, one patient in the alendronate arm died, and one patient in the placebo arm stopped treatment for side effects (allergy). Another three patients were not evaluated by DXA at week 48 (one in the alendronate arm and two in the placebo arm). Three of these 10 patients, all in the placebo arm, were evaluated at week 96. Between week 48 and week 96, three patients stopped treatment and follow-up and were therefore not evaluated by DXA: two patients in the alendronate arm and one in the placebo arm were lost to follow-up. In addition, two patients in the placebo arm stopped treatment but were evaluated by DXA at week 96. Imputation of missing data was used to include patients without DXA evaluation in the ITT analyses of all enrolled patients, while these patients were excluded from the analysis on available data.
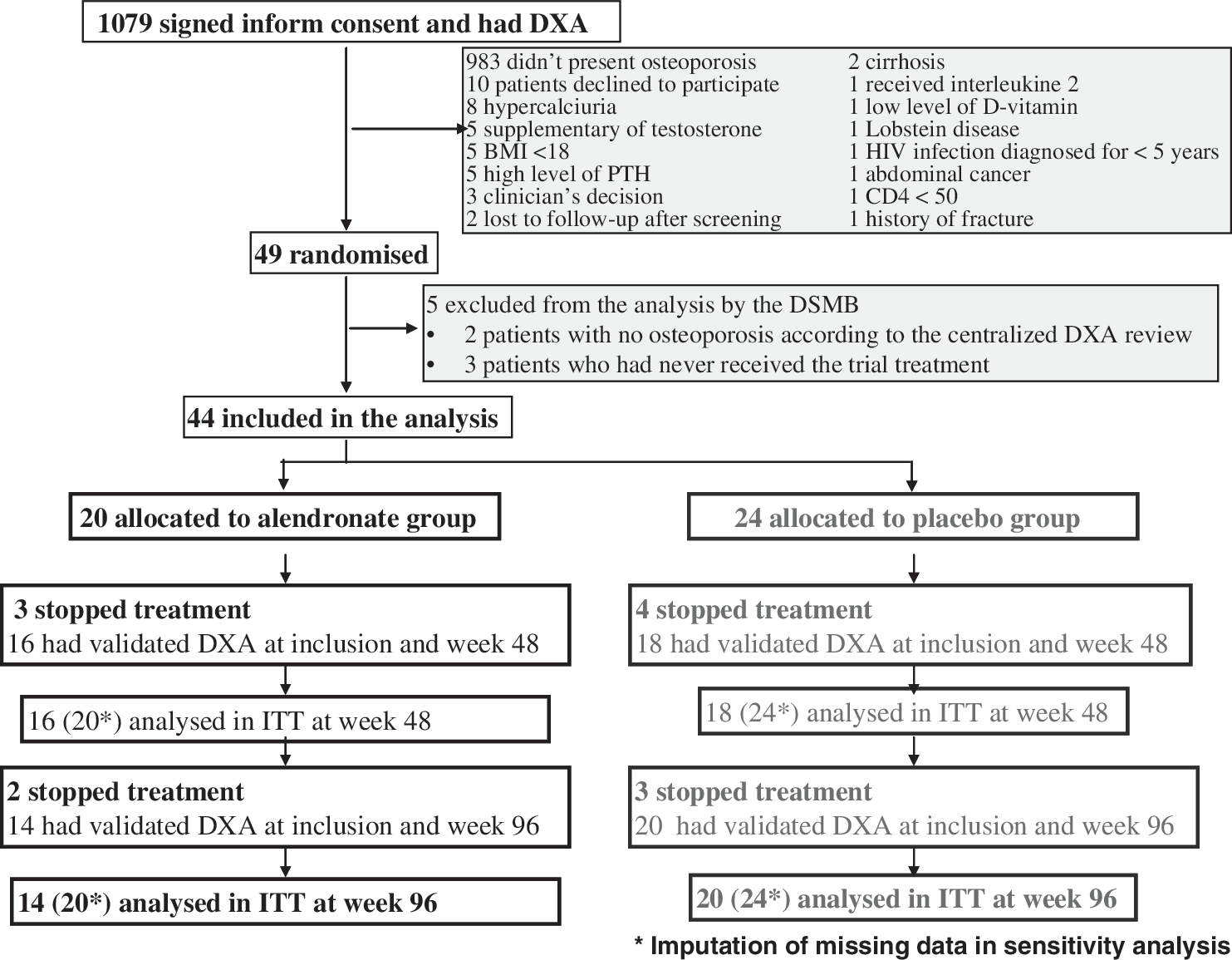
Trial flow chart.
Characteristics of the patients
The patients' baseline characteristics were well balanced between the two arms (Table 1). Most of the patients were men (95%). The median age was 45 years [interquartile range (IQR) 41–53, range 27–75] and 36% of the patients were over 50 years old. The baseline median CD4 cell count was 422/mm3 (IQR 314–678), and the plasma HIV-1 RNA level exceeded 400 copies/ml in seven patients (16%) (89,500, 81,900, 12,800, 6702, 749, 659, and 406 copies/ml).
Baseline Characteristics of the Patients
Values are N (%) unless otherwise indicated.
Numbers are medians (Q1–Q3).
Numbers are means (standard deviation).
ARV, antiretroviral; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor; IU, international unit.
At the screening visit the t-score was ≤−2.5 at the lumbar spine in 17 patients in the alendronate arm and in 18 patients in the placebo arm. Respectively, 6 patients and 1 patient also had a t-score ≤−2.5 at the hip.
All the patients had received antiretroviral therapy, starting a median of 9 years previously (IQR=6–11). All the patients were receiving antiretroviral therapy at baseline, and 14 patients (32%) were receiving tenofovir. No protease inhibitors were introduced or withdrawn during follow-up. Tenofovir was introduced in one patient in each arm and was interrupted in one patient in the placebo arm.
Changes in BMD
In the analysis of available data at 96 weeks, the percentage change in BMD at the site with a t-score ≤−2.5 was significantly larger in the alendronate arm (7.1±4.2%) than in the placebo arm (1.0±4.8%, p=0.0003, Table 2). The difference between the groups remained significant in full ITT analyses taking missing data into account (LOCF approach or imputation of Q1 or Q3 for missing DXA values at week 96: p=0.0128, 0.0104, and 0.0014, respectively). In addition, after 48 weeks the percentage change in BMD at the site with a t-score≤2.5 was already significantly larger in the alendronate arm (5.5±4.7%) than in the placebo arm (0.0±3.9%, p=0.0004). Compared to the placebo group, patients who received alendronate had a larger percentage change in BMD at the lumbar spine (7.0±4.1% versus 0.7±5.0%, p=0.0003) but not at the total hip (4.4±6.4% versus 2.3±3.0%, p=0.529). Figure 2 shows the percentage changes in BMD in the analysis of patients with available data at the three visits (screening, week 48, and week 96: 14 patients in the alendronate group and 16 in the placebo group). The between-group difference in the percentage change was 7.4% [95% CI=(4.4; 10.5)] at the site with a t-score≤2.5 (Fig. 2A), 7.7% [95% CI=(4.4; 10.5)] at the lumbar spine (Fig. 2B), and 2.6% [95% CI=(−1.3; 6.6)] at the total hip (Fig. 2C). Mixed linear models based on available data (112 BMD measurements for the site with a t-score≤2.5, 113 for the lumbar spine and 109 for the hip) confirmed these results: relative to the placebo group, alendronate therapy increased BMD significantly at the site with a t-score≤2.5 (p=0.0016) and at the lumbar spine (p=0.0016) but not at the total hip (p=0.3240).
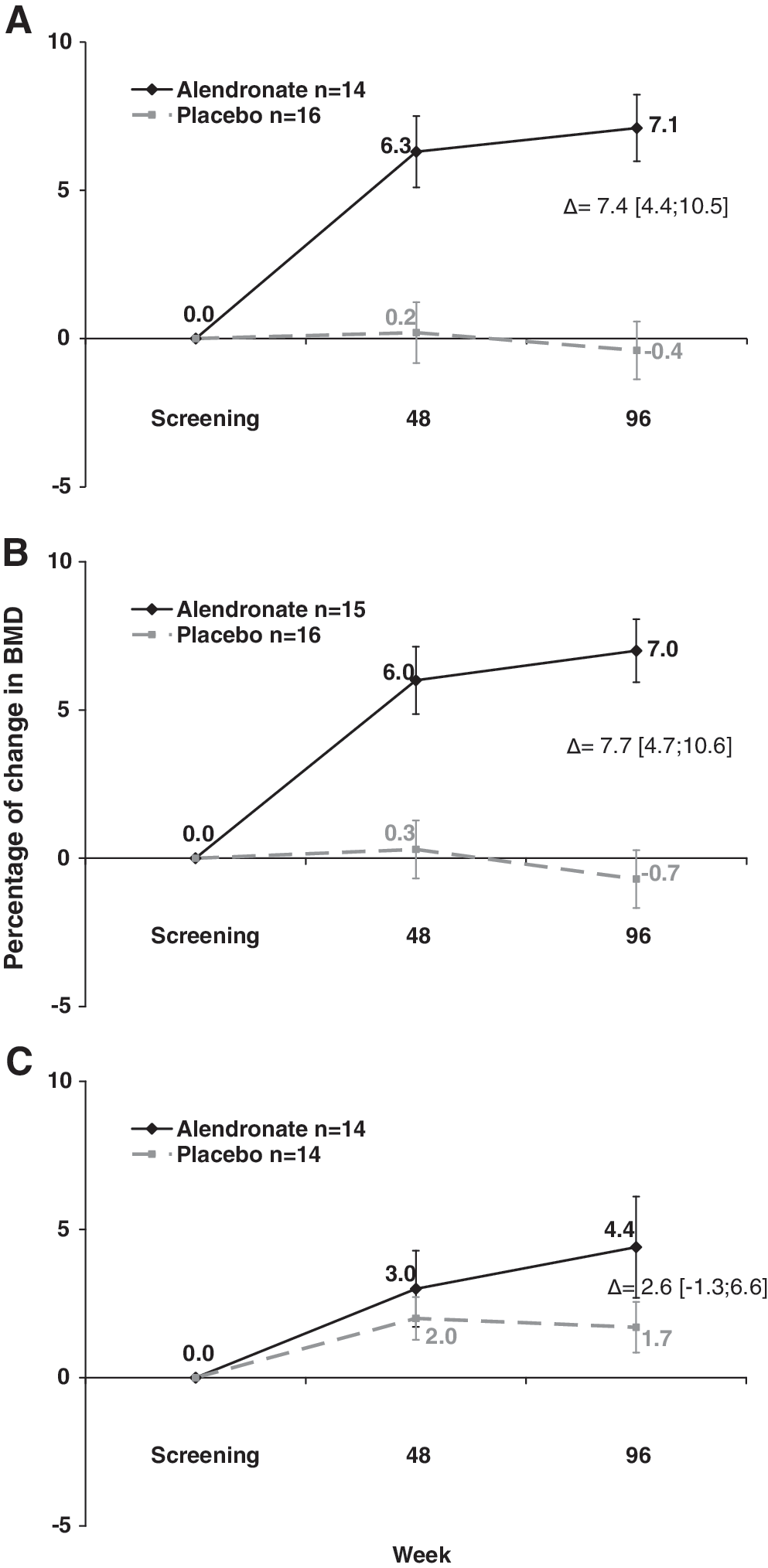
Mean percentage change (±standard error of the mean, SEM) from baseline in bone mineral density (BMD) at the site with t-score ≤−2.5
Changes in Bone Mineral Density Between Week 0 and Week 96
Mann–Whitney test.
ITT, intent-to-treat; LOCF, last observation carried forward; Q1, first quartile; Q3, third quartile; BMD, bone mineral density.
At week 96, the change in BMD at the lumbar spine exceeded the SDD in 80% of patients in the alendronate group and 20% of patients in the placebo group (p=0.0006), while the change in BMD at the total hip exceeded the SDD in, respectively, 43% and 37% of patients (p=1.00).
Biomarkers of bone turnover
After 96 weeks of alendronate therapy the alkaline phosphatase level had fallen more strongly in the alendronate arm (−21.4±29.0 IU/liter) than in the placebo arm (−5.0±20.3 IU/liter, p=0.06). Changes in other biomarkers of bone turnover (osteocalcin and serum crosslaps) did not differ between the two groups (Table 3). Alendronate therapy had no effect on the week 0 to 96 percentage change in alkaline phosphatase levels, available for 29 patients (p=0.11); or in osteocalcin levels, available for 20 patients (p=0.32); or in serum crosslap levels, available for 17 patients (p=0.44).
Changes in Biological Parameters
Mann–Whitney test.
Adverse events
Changes in serum creatinine, AST, ALT and serum phosphorus levels between screening and week 96 were not significantly different between the arms. During the study period, 19 serious adverse events occurred in 13 patients, comprising four patients in the alendronate arm (acute prostatitis and lithotripsy; adrenal insufficiency and left otitis externa; iron deficiency anemia; and death after diagnosis of epidermoid carcinoma) and nine patients in the placebo arm (three episodes of benzodiazepine withdrawal syndrome, Helicobacter pylori gastritis, and a depressive syndrome; inferior myocardial infarction; pneumopathy; viral gastroenteritis; vitrectomy; Mycoplasma pneumoniae pneumonia; lung superinfection; pneumonia; and an allergic reaction). The proportion of patients with serious adverse events did not differ between the groups (p=0.321). No fractures occurred in the alendronate arm, while one traumatic fracture of the coccyx and one traumatic fracture of the clavicle occurred in the placebo arm (p=0.49). No cases of jaw osteonecrosis occurred.
Discussion
In this placebo-controlled study of 44 osteoporotic HIV-infected patients, 42 of whom were men, alendronate 70 mg/week for 2 years was associated with a significant increase in BMD at the site of osteoporosis. The difference was significant at the lumbar spine but not at the total hip, possibly because of the small group sizes and the fact that only 19 patients had a total-hip t-score of ≤−2.5 at baseline.
The decision to use a t-score of ≤−2.5 to define low BMD may be questionable, as 64% of the patients included in this study were under 50 years old, while current guidelines recommend the use of z-scores for this population. However, it should be noted that 90% of the patients under 50 years old in our study fulfilled the z-score criterion for low BMD (≤–2.0). In addition, our study was planned in the mid-2000s, when available guidelines 22 recommended the use of a t-score below −2.5 even for patients under 50 years old. It is noteworthy that this criterion is more demanding than a t-score below −2, as used in Orwoll's study to assess alendronate in men aged from 31 to 87 years. 18 Other limitations of our study are the small sample size and the fact that 23% of patients could not be evaluated at week 96. However, our results are robust, when we used mixed linear models on available data or full ITT analyses using imputation techniques for missing data. For the primary endpoint, use of the analysis on evaluable data in this study is close to an on-treatment analysis, as most patients who stopped therapy did not undergo DXA scans. The large number of missing data, in particular at weeks 48 and 96, probably explains the absence of significant results for osteocalcin and serum β-crosslaps. Although total alkaline phosphatase is not bone specific, the decline is not surprising as bone remodeling is reduced by bisphosphonates, as can be shown by the trend of a decline in serum β-crosslaps in the group treated by alendronate.
The gender imbalance in this study is explained by several factors. For ethical reasons, we chose to enroll both men and women, but we excluded postmenopausal women in order to rule out an effect of osteoporosis risk factors than HIV infection and its treatment. Osteoporosis is also less frequent in women than men in the HIV-infected population. 3 We chose to keep the two women in the analysis, but the results would be similar in men only.
Our result for the lumbar spine is similar, with an absolute difference between groups of 7.7% [95% CI=(4.4–10.5)] and those obtained in Orwoll's study of 241 HIV-seronegative men with a mean age of 63 years that is 5.3% (4.3–6.3). 18 In his study, the difference was smaller at the hip, which is an absolute difference between groups of 2.6% (but still significant relative to the placebo group), possibly because alendronate is more effective on trabecular bone than on cortical bone. Given our small sample size, we were not able to detect this smaller effect at the hip while our effect was similar (an absolute difference between groups of 2.6% as well).
The main strengths of this study are that it involved osteoporotic patients, was double-blinded, and lasted 2 years. As the pathophysiology of HIV-associated osteoporosis is multifactorial, it was important to assess bisphosphonate efficacy only in patients who may need this treatment.
Several authors have tested alendronate in HIV-infected patients, 23 –28 but our study is the only one in which all patients were osteoporotic and therefore the study included the largest number of such patients, all patients received vitamin D and calcium, and all patients were followed for 2 years.
Negredo et al. 26 studied 26 patients with t-scores ≤−2.5 SD in a 96-week open randomized trial, but no patient received vitamin D or calcium supplementation. Alendronate significantly reduced the proportion of patients with osteoporosis at 2 years (27% in the alendronate group versus 96% in the control group); surprisingly, however, no significant difference in the change in BMD was observed either at the spine or hip, probably due to the small sample size.
McComsey's double-blind, randomized, placebo-controlled 1-year study based on centrally analyzed DXA scans included 82 patients with t-scores ≤−1.5 SD, of whom only 30% had osteoporosis. 23 All the patients received calcium and vitamin D supplementation. Alendronate had a significant beneficial effect on spine and total hip BMD values at week 48 with absolute differences between groups of 2.3 and 2.6%, respectively, smaller than our observed effect at lumbar spine at 96 weeks and similar to our observed effect at total hip.
Mondy et al. conducted an open randomized study of 31 patients with t-scores <−1.0 SD at lumbar spine, 19% of whom had osteoporosis. All the patients received calcium and vitamin D. A significant increase in spine BMD was noted at 1 year, 24 the effect being 3.9%, approximately half of the effect observed in our study at week 96. The third study, an open randomized 52-week trial involving 41 patients with t-scores <−1.0 SD, all of whom received calcium and vitamin D, showed no significant effect of alendronate on BMD, 25 probably because the study was not blinded, included patients with BMD values higher than other studies, and lasted only 48 weeks. A significant benefit was noted 1 year after a single intravenous zoledronate infusion in a 12-month randomized double-blind placebo-controlled study involving 30 HIV-infected patients with t-scores ≤−1.5 SD 27 ; the effect was 3.0% and 1.4% at spine and hip, respectively, at 1 year, which is roughly 50% of our observed effect at 96 weeks. Osteoporosis was present at baseline in 20% and 7% of the patients in the zoledronate and placebo groups, respectively. All the patients received vitamin D and calcium.
Finally, Bolland et al. conducted a 2-year randomized double-blind placebo-controlled trial involving 43 HIV-infected men with t-scores ≤−0.5 SD. 28 All the patients received vitamin D and calcium. Zoledronate was found to be effective as preventive or corrective treatment for bone loss with effects at 2 years similar to those in our study (6.3% and 3.0% at the lumbar spine and hip, respectively). Together, these studies indicate that bisphosphonates are effective for HIV-associated osteoporosis.
Studies of postmenopausal women have also shown that alendronate can prevent fractures. 13 This preventive effect has not yet been demonstrated in HIV-infected patients, because such studies require very large numbers of patients. However, there is mounting evidence of an increased risk of fracture in osteoporotic HIV-infected patients. 12 –15,29
Long-term use of alendronate has been studied only in elderly women, for periods of only 10 or 15 years. Chronic alendronate therapy in HIV-infected patients, starting in middle age, might carry unknown risks. The indications of alendronate in this population must thus take into account not only BMD but also age, BMI, dietary factors, the personal and family history of fracture, smoking, steroid intake, and other risk factors for osteoporosis.
In conclusion, this study shows that alendronate 70 mg weekly for 96 weeks improves bone mineral density in antiretroviral-treated HIV-infected patients with t-scores ≤2.5, with effects similar to those observed in non-HIV-infected individuals.
Appendix: Other Members of the ANRS 120 FOSIVIR Study Team
Clinical Centers (in order of the number of patients screened): Hôpital Pitié-Salpêtrière, Paris–C. Katlama, M.A. Valantin, L. Schneider, and H. Schoen; Hôpital Avicenne, Bobigny–M. Bentata, P. Honoré, F. Rouges, and L. Tuna; Hôpital Pitié-Salpêtrière, Paris–A. Simon, M. Bonmarchand, and M. Irguetsira; Hôpital Cochin, Paris–D. Salmon-Céron, N. Benammar, F. Almasi, and V. Le Baut; Hôpital Bichat, Paris – P. Yeni, S. Matheron, N. El Alami Talbi, and G. Fraqueiro; Hôpital Necker, Paris–J.P. Viard, G. Obenga, and A. Maignan; Hôpital Tenon, Paris–G. Pialoux, L. Slama, C. Fontaine, and C. Chakvetadze; Hôpital Bellevue, Saint-Etienne–F. Lucht and A. Frésard; Hôpital Côte de Nacre, Caen–R. Verdon, J.J. Parienti, and C. Bazin; Hôpital Saint-André, Bordeaux–D. Malvy, P Mercié, and I. Louis; Hôpital Gustave Dron, Tourcoing–Y. Yasdanpanah, S. Pavel, V. Baclet, and F. Ajana; Hôpital Lariboisière, Paris–A. Rami, P. Sellier, and M. Parrinello; Hôpital Hôtel-Dieu, Nantes–F. Raffi, V. Reliquet, and C. Brunet-François; Hôpital Raymond Poincaré, Garches–J.C. Melchior, P. de Truchis, D. Mathez, and H. Berthé; Hôpital Saint Jacques, Besançon–C. Drobacheff-Thiébaut and A. Foltzer; Hôpital Paul Brousse, Villejuif–D. Vittecoq and E. Teicher; Hôpital Saint-Louis, Paris–D. Séréni; Centre Hospitalier Intercommunal, Créteil–V. Garrait, I. Delacroix, B. Elharrar, and M. Mouchet; Hôpital Gabriel Montpied, Clermont-Ferrand–C. Jacomet, F. Gourdon, and H. Laurichesse; Hôpital de Bicêtre, Le Kremlin-Bicêtre–C. Goujard, B. Brunet, M. De Lavaissière, and M.T. Rannou; Hôpital Tarnier, Paris–I. Gorin and J. Deleuze; Hôpital Saint-Joseph, Paris–J. Gilquin, A. Chassaing, and A. Cros; Hôpital Saint-Louis, Paris–L. Gérard and J. Delgado; Hôpital Sainte Marguerite, Marseille–I. Poizot-Martin, M. P. Drogoul, S. Brégigeon, and G. Fabre; Hôpital Albert Michallon, Grenoble–P. Leclercq; Hôpital Saint Jacques, Besançon–B. Hoen and L. Hustache-Mathieu; Hôpital Louis Mourier, Colombes–Pr Vinceneux.
DXA Centers: Hôpital Pitié-Salpêtrière, Paris–S. Rozenberg and R. Inaoui; Hôpital Avicenne, Bobigny–P. Weinmann; Hôpital Cochin, Paris–C. Roux, S. Kolta, and N Vautier; Hôpital Bichat, Paris–C. Clerici and M. Essig; Hôpital Tenon, Paris–Hôpital Rothschild, Paris–A. Sebag and M.C. Muller; Hôpital Bellevue, Saint-Etienne–T. Thomas and P. Collet; Hôpital Côte de Nacre, Caen–J.P. Sabatier; Hôpital Pellegrin, Bordeaux–N. Bathe; Hôpital Roger Salengro, Lille–J.M. Decamps, N. Duquesnoy, V. Abou Argoub, and J. Cano-Morales; Hôpital Lariboisière, Paris–M.C. De Vernejoul and H. Cucchi; Hôpital Hôtel-Dieu, Nantes–Y. Maugars and J. Glémarec; Hôpital Raymond Poincaré, Garches–R. Carlier, D. Mompoint, C. Le Breton, and D. Safa; Hôpital Jean Minjoz, Besançon–H. Boulhardour, C. Ungureanu, C. Caoduro, and G. Quémard; Hôpital St Louis, Paris–E. de Kerviller and C. Bergot; Hôpital Gabriel Montpied, Clermont-Ferrand–J.M. Ristori and S. Malochet; Hôpital La Timone, Marseille–P. Champsaur; Hôpital Albert Michallon, Grenoble–G. Ferretti and L. Pittet-Barbier.
Footnotes
Acknowledgments
The French National Agency for AIDS and Viral Hepatitis Research (ANRS) 120-Fosivir trial was sponsored by Agence Nationale de Recherche sur le SIDA et les hépatites virales (ANRS).
After approving the protocol, the sponsor had no role in the collection, analysis, or interpretation of the data, writing of the report, or the decision to submit the article for publication. This study was registered with clinicaltrials.gov under number NCT00120757. This trial was reported as an oral presentation at the 12th European AIDS Conference (EACS), November 11–14, 2009, Cologne, Germany.
Contributors: Provision of study materials or patient enrolment: M.B., J.-P.V., M.-A.V., P.M., I.D., C.R., and S.K. Statistical analysis: E.L. and D.C. Drafting of the article: S.R., E.L., S.K., and D.C. Study design, data interpretation, and critical revision of the article for important intellectual content and final approval of the article: all authors. Data and safety monitoring board: Geneviève Chêne, Jean-Michel Molina, Philippe Orcel, and Elisabeth Rouveix
Author Disclosure Statement
No competing financial interests exist.