
Abstract
The purpose of this study was to investigate the amino acid substitutions in the protease of HIV-1 B and non-B subtypes and evaluate whether the emergence of resistance-associated mutations (RAMs) could have a significant correlation with the increasing prevalence of CRF02_AG strains in Morocco. A total of 162 protease gene sequences were successfully amplified from drug-naive HIV-1-infected individuals. We identified eight (sub)subtypes and CRFs: B(66%), A1(3.7%), C(1.2%), F1(0.6%), F2(0.6%), G(1.2%), CRF02_AG(25.3%), and CRF01_AE(1.2%). Phylogenetic analysis of CRF02_AG strains showed that 9.8% of isolates had a closer connection with reference strains from Morocco and 15.4% clustered with reference strains from eight West African and three European countries. When compared to the B subtype, patients with the CRF02_AG strain had a significantly higher prevalence of mutations associated with resistance to some antiprotease drugs, mainly tipranavir (TPV): H69K (97% vs. 5%; p<0.0001), L89M (95% vs. 1%; p<0.0001), and M36I/L (93% vs. 44%; p<0.0001). Most of the CRF02_AG strains (97%) significantly showed at least two TPV-RAMs (p=0.002) compared to the B subtype (7%). Multivariate analysis revealed that CRF02_AG infection was the only factor highly associated with the occurrence of more than two TPV-RAMs (C=0.42; p<0.0001). These results support the importance of transmitted drug resistance mutations (M36I/L, H69K, and L89M) in the protease gene of HIV-1 CRF02_AG isolates. This HIV drug resistance transmission before protease inhibitor (PI) exposure raises concern about its influence on the susceptibility of CRF02_AG strains to some PIs, especially tipranavir, which will soon be introduced as part of the second line therapeutic regimens in Morocco.
Introduction
O
Morocco's HIV-1 prevalence remains at a relatively low level (less than 1%). About 25,000 persons were living with HIV-1 in Morocco in 2010 and a total of 3621 cases of AIDS were documented, of which 42% were women. The majority of HIV infections in Morocco are due to heterosexual transmission (81%) followed by perinatal transmission (6%), homosexual transmission (4%), and intravenous drug use (3%). The identified AIDS cases are distributed in different Moroccan regions, mainly Sous Massa Draa (25%), Marrakesh Tensift Al Haouz (18%), and Grand Casablanca (11%). 7
Over the past 12 years, Morocco has provided free access to HAART (highly active antiretroviral therapy) for all HIV-1-infected patients eligible for antiretroviral (ARV) treatment. The protease inhibitor (PI) regimens used in Morocco varied over time. Thus, indinavir was first used between 1999 and 2004, and then indinavir/ritonavir and lopinavir/ritonavir were introduced in ARV Moroccan regimens. PIs are an important class of ARV drugs, but resistance-associated mutations (RAMs) are commonly observed in the protease gene and can affect the effectiveness of ARV drugs. 8,9 Furthermore, HIV-1 genetic diversity may influence the pattern of RAMs that might eventually emerge upon drug exposure as well as the rate of emergence of resistance. 10,11 The variability at the HIV-1 protease gene may account for differences in drug resistance pathways and distinct susceptibility to some of the new antiretroviral drugs. Thus, the growing diversity of HIV-1 subtypes in Morocco highlights the need for closer epidemiological characterization of viral isolates prior to the introduction of new PIs in this country.
The purpose of this study was to investigate the amino acid substitutions in the protease gene of HIV-1 B and non-B subtypes among drug-naive HIV-1-infected patients and evaluate whether the emergence of RAMs could have a significant correlation with the increasing prevalence of CRF02_AG strains.
Materials and Methods
Patients and samples
Our population is composed of 197 newly diagnosed individuals enrolled between 2006 and 2010 and followed at the Infectious Disease Unit of the University Hospital Center (CHU Ibn Rochd), Casablanca, Morocco. Among these individuals, 47% are from Casablanca. The remaining 53% are from various parts of the country. The Infectious Disease Unit of Casablanca receives actually about 60% of HIV-infected patients from all regions of Morocco.
During the recruitment period, all subjects consulting in this hospital for HIV infection and newly diagnosed as HIV positive were included in our study. Inclusion criteria were newly diagnosed HIV-1 infection, no history of antiretroviral therapy, age over 15 years, and HIV-1 RNA load more than 1000 copies/ml. This research project has been approved by our local Institutional Review Board.
RNA extraction, RT-PCR, and DNA sequencing
One milliliter of HIV-1 plasma samples was firstl centrifuged at 21,500×g for 105 min at 4°C. Viral RNA was then extracted using the QIAamp viral RNA mini kit (QIAGEN, Germany) according to the manufacturer's protocol. The HIV-1 protease gene was amplified by one-step reverse transcription (RT)-coupled polymerase chain reaction (PCR) using the Superscript One-Step RT-PCR with Platinum Taq DNA polymerase (Invitrogen, USA), followed by nested PCR using Taq DNA polymerase (Invitrogen, USA). Amplification was done according to the HIV-1 PCR and Sequencing Procedures of the ANRS AC11 Resistance Study Group (
Protease genes were successfully amplified and sequenced for 162 of 197 samples. Among them, 12 samples were collected in 2006, 40 in 2007, 36 in 2008, 38 in 2009, and 36 in 2010. Sequences generated in this study have been submitted to GenBank under accession numbers JN222581 to JN222742.
Phylogenetic analysis
Protease sequences were aligned with reference sequences of all known HIV-1 subsubtypes and circulating recombinant forms (CRFs) from the Los Alamos HIV sequence database (
Genotypic drug resistance interpretation algorithms
The protease sequences were analyzed for potential drug resistance-associated mutations using the last International AIDS Society (IAS)-USA Drug resistance mutation list
15
and the last rules of the French ANRS AC11 Resistance group (
Statistical analysis
All samples were categorized into two groups according to their HIV-1 protease gene subtype: samples with HIV-1 CRF02_AG strains and samples with subtype B. Mean (±SD), median (interquartile range, IQR), and frequencies (as percentages) were used to indicate the populations' characteristics in each group. Student's t-test was used to compare the mean values of continuous variables with normal distribution between the two groups, and the Mann–Whitney U-test was used to compare the median values for continuous variables with nonnormal distribution. Chi-square test and Fisher's exact test were used to compare qualitative parameters. Univariate and multivariate analyses were performed to assess which factors were related to the presence of more than two TPV-RAMs. Spearman's rho was used to evaluate the correlation of RAMs to CRF02_AG strains. All analyses were performed using XLSTAT software (
Results
A total of 162 individuals were studied between 2006 and 2010. The main characteristics of this population were as follows: the mean age was 36 years old (range 15–64 years) and 45% of the patients were male, the median (IQR) CD4 cell count was 270.4 (78.6–574.8) cells/mm3, and the median (IQR) HIV-1 RNA load was 5.23 (4.36–5.9) log copies/ml. We identified 82.9% of heterosexuals, 3.4% of homosexuals, 2.2% of intravenous drug users, and for 11.4% of the patients the risk exposure was unknown. Patients had different clinical stages at the time of diagnosis: A (73.9%), B (5.7%), and C (20.4%). Among the protease gene fragments analyzed, eight subsubtypes and CRFs were identified, including subsubtypes B, A1, C, F1, F2, G, CRF02_AG, and CRF01_AE. Phylogenetic analysis showed that 107 (66%) sequences belonged to subtype B and 55 (34%) to non-B subtypes and recombinant forms: 6 (3.7%) A1, 2 (1.2%) C, 1 (0.6%) F1, 1 (0.6%) F2, 2 (1.2%) G, 41 (25.3%) CRF02_AG, and 2 (1.2%) CRF01_AE. Table 1 summarizes the baseline characteristics of patients with CRF02_AG strains and those with subtype B. There were no differences of baseline characteristics between the two groups.
The phylogenetic tree constructed using non-B sequences identified in our study population is shown in Fig. 1. The selected CRF02_AG reference strains (n=36) were identified from 12 countries worldwide. Phylogenetic analysis of CRF02_AG strains resulted in one major cluster (white circles in the phylogenetic tree), representing 9.8% (16/162) of isolates, and showed a closer connection with reference strains from Morocco. 6 The remaining 15.4% (25/162) of CRF02_AG isolates (gray circles of the tree) are clustered with reference strains from eight countries of West Africa (Cameroon, Mali, Gabon, Nigeria, Senegal, Ghana, Ivory Coast, Burkina Faso) and three of Europe (Spain, Portugal, France).
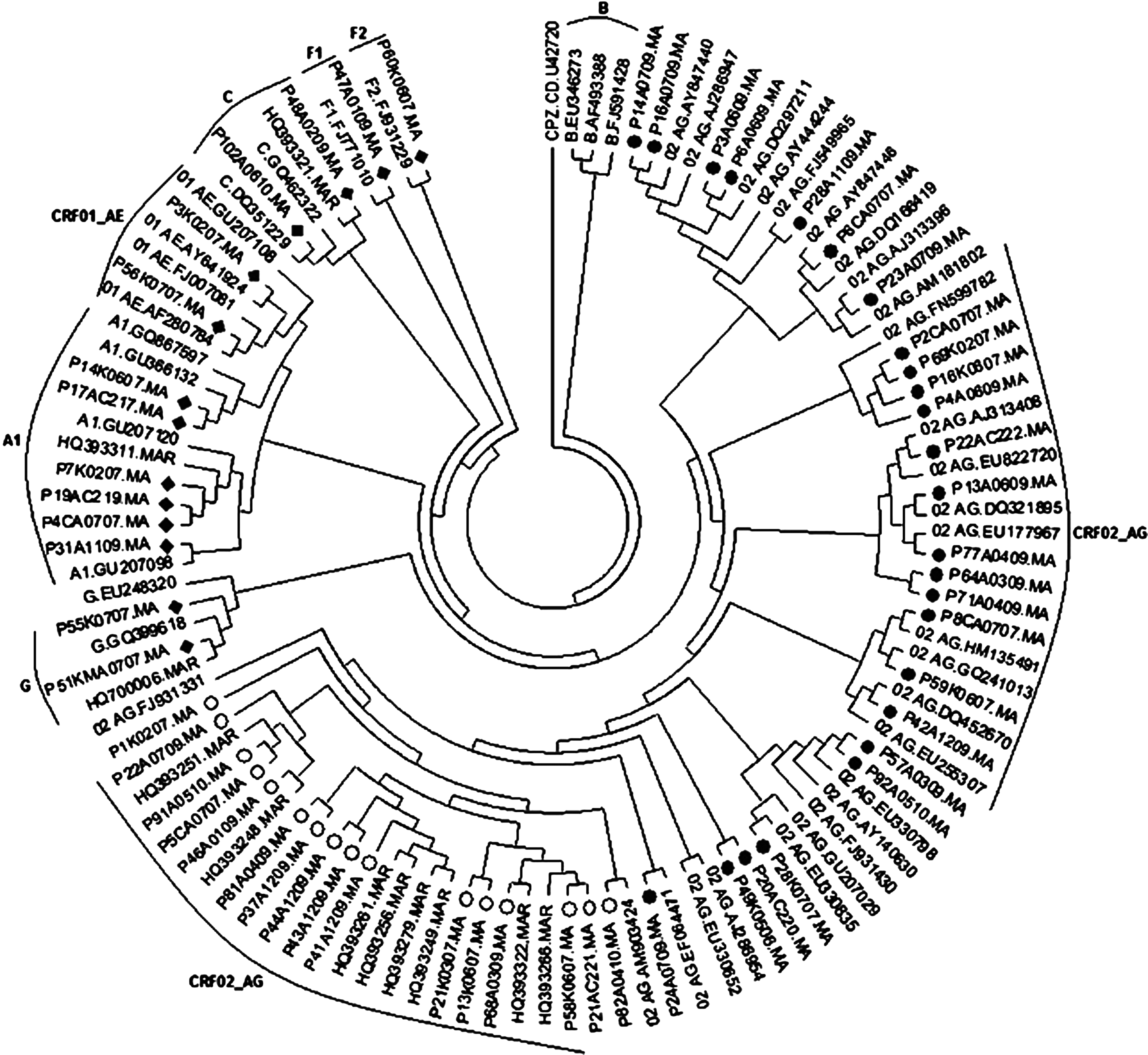
Phylogenetic tree of the protease region for HIV-1 non-B subtypes. Reference sequences included in the tree are obtained from the Los Alamos HIV Database with their original designations. Clinical samples characterized herein and belonging to CRF02_AG strains are marked with circles (●,○). Samples belonging to the remaining non-B subtypes are marked with diamonds (♦). HIV-1 sequence CPZ.CD U42720 was used as an outgroup.
To characterize RAMs, both major and minor resistance mutations in the PR gene were considered. None of the patient isolates contained major resistance mutations within the PR gene. However, 157 of the 162 isolates (97%) contained at least one minor mutation that is associated with resistance to PIs. Among the mutations identified, M36I/L (57.4%), K20I/M/R (35%), H69K (34%), and L89M (32.7%) were most frequently observed in CRF02_AG isolates than in B subtypes. Moreover, 48/162 (29.6%) of samples had simultaneously changes in their PR gene at the most frequently observed positions corresponding to M36, H69, and L89. These three protein changes were seen in 77% (37/48) of CRF02_AG strains. Additionally, for non-B subtypes, M36I/L was observed in 6/6 of A1 isolates, 2/2 of C, 2/2 of G, 1/1 of F1, 1/1 of F2, and 2/2 of CRF01_AE isolates; K20I/M/R was observed in 3/6 of A1, 2/2 of C, 2/2 of G, 1/1 of F2, and 1/2 of CRF01_AE isolates; H69K was observed in 4/6 of A1, 2/2 of C, 2/2 of G, and 2/2 of CRF01_AE isolates; and mutation L89M was observed in 5/6 of A1, 2/2 of C, 2/2 of G, 1/1 of F1, 1/1 of F2, and 2/2 of CRF01_AE isolates.
The other mutations were seen with lower frequencies in some samples: L63P (32%), I62V (20.3%), I64V (19.7%), G16E (16.6%), L10V (14.8%), V77I (14.8%), I93L (11.7%), and V82I (1.8%) (Table 2). Some of these more frequently selected mutations (L10V, M36I/L, H69K, L89M) were associated with exposure to tipranavir (TPV). 15,17 Frequencies of patients with 0, 1, 2, 3, and 4 TPV resistance-associated mutations (TPV-RAMs) were 29% (47/162), 28% (45/162), 13% (21/162), 24% (39/162), and 6% (10/162), respectively. The median number (IQR) of TPV-RAMs was 3 (0–3). Figure 2 shows the most common TPV-RAMs found in patients with the CRF02_AG strain and those with subtype B. Interestingly, the mean number of TPV-RAMs was higher in CRF02_AG strains when compared to subtype B isolates. Univariate analysis revealed that substitutions at positions H69K (97% vs. 5%; p<0.0001), L89M (95% vs. 1%; p<0.0001), and M36I/L (93% vs. 44%; p<0.0001) were more common in CRF02_AG than B viruses.
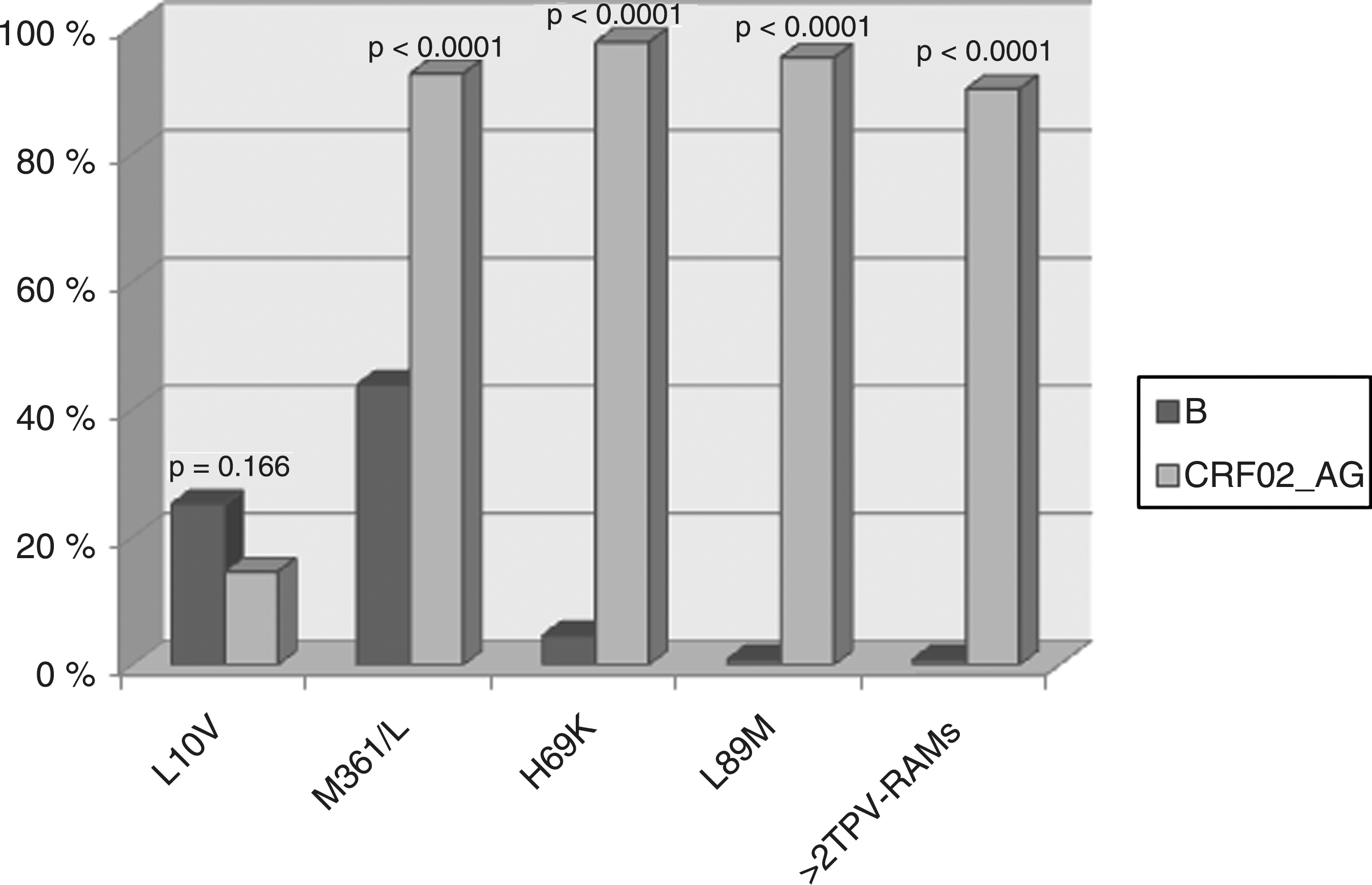
Prevalence of the most common tipranavir resistance-associated mutations (TPV-RAMs) according to HIV-1 CRF02_AG strain and B subtype.
TPV-RAMs, tipranavir resistance-associated mutations.
There were significant correlations between the occurrence of M36I, H69K, and L89M in these studied individuals. The correlation between the occurrence of H69K and L89M (r=0.84, p<0.0001) was stronger than the correlations between M36I/L and L89M (r=0.21, p<0.0001) and between M36I/L and H69K (r=0.17, p<0.0001). Furthermore, patients with CRF02_AG strains commonly had more than two TPV-RAMs when compared to patients with subtype B (90% vs. 1%; p<0.001). In multivariate analysis, only the CRF02_AG strain was significantly associated with the occurrence of more than two TPV-RAMs (C=0.42; p<0.0001). Gender, age, CD4 cell count, and HIV-1 RNA load were not associated with the occurrence of more than two TPV-RAMs (p>0.05).
Discussion
In this study, a total of 162 protease gene sequences were successfully amplified and sequenced from drug-naive HIV-1-infected individuals recently diagnosed between 2006 and 2010. Nevertheless, most of the individuals were diagnosed in Morocco at an advanced stage of infection and the exact lapse of time between infection and samples collection is unknown. Nearly 52% of diagnoses are made at stage C. Our results showed that 34% of individuals were infected with non-B strains, mainly CRF02_AG, which represents 25.3% of these naive patients. Detailed phylogenetic analysis of protease sequences showed that 15.4% of isolates had a closer relationship to reference strains from West African and European countries, which agreed with previous reports that suggest that Africa's migration passage to Europe is a potentially significant contributor to the spread of HIV-1 CRF02_AG infection in Morocco. 18,19 During the past 10 years, Morocco has become a destination country instead of transit zone of migrants from sub-Saharan countries, 20 mainly West African countries where the most predominant HIV-1 strain is CRF02_AG. 4,21 –24 This phenomenon could explain the introduction and the spread of CRF02_AG strains in several regions of Morocco. Nevertheless, 9.8% of CRF02_AG isolates showed a closer connection with reference strains from Morocco, indicating that the introduction of the CRF02_AG strain in this country is not recent.
By analyzing protease RAMs in subtype B and CRF02_AG, we found that their overall frequency was considerably higher in CRF02_AG than in B strains, confirming the results of previous reports. 25,26 Holguin et al. 27 indicated in their study the potential role of the observed substitutions K20I, M36I, L63P, and V82I in contributing to low susceptibilities to PR inhibitors. They found a 2.9-fold decrease in amprenavir (APV) susceptibility associated with the mutations K20I, M36I, and V82I and a 3.9-fold decrease in both nelfinavir (NFV) and ritonavir (RTV) susceptibility associated with amino acid substitutions K20I, M36I, L63P, and V82I. Two of the CRF02_AG-infected patients harboring these mutations were observed in our study population, but none of them was under ARV therapy. Furthermore, three substitutions, M36I, H69K, and L89M, are simultaneously found in the protease gene of 90% (37/41) of the CRF02_AG studied strains.
The 2010 IAS-USA Drug Resistance Mutations Group has added L89M to the list of TPV-RAMs 15 and previous studies revealed that the mutations in protease genes M36I/L/V, H69I/K/N/Q/R/Y, and L89I/M/R/T/V were found to be associated with reduced susceptibility and diminished virological response to TPV. 28,29 Reduced response to TPV is associated with the presence of more than two TPV-RAMs and loss of response occurs when there are eight TPV-RAMs. 29 Additionally, the results of multivariate analysis showed that CRF02_AG infection was the only factor highly associated with the occurrence of more than two TPV-RAMs. These results agree with previous reports that describe a significant high frequency of TPV-RAMs in non-B subtype viruses. 17,28,30,31
The widespread of drug resistance-associated mutations to tipranavir in Morocco is possibly due to the contamination by HIV-1-infected individuals receiving treatment from Non-Moroccan organizations to preserve their confidentiality, principally in Northern Morocco, close to the Spanish borders. This could also be explained by the contamination by infected subjects coming from countries where tipranavir is accessible (especially in Europe). Thus, our findings showing that HIV-1 CRF02_AG isolates were highly associated with the occurrence of RAMs in the protease gene and that these non-B strains are becoming increasingly prevalent must be taken into account by Moroccan public health officials. Our study, in agreement with others, 26,29 showed that CRF02_AG strains are less susceptible to PIs, mainly tipranavir, which will soon be introduced as a second line therapeutic regimen in the national AIDS control program.
In summary, these results support the importance of transmitted drug resistance mutations, principally M36I/L, H69K, and L89M, in the protease of HIV-1 CRF02_AG isolates. Our findings reinforce the need for analyzing the resistance genotype in drug-naive patients infected by non-B subtypes, mostly the CRF02_AG strain, to guide clinicians in their choice of therapeutic regimen and in the design of control strategies to limit the spread of circulating viruses and to enhance our understanding of viral diversity. 32,33
Sequence Data
All the 162 sequences generated from this study were deposited in GenBank under accession numbers JN222581 to JN222742.
Reference Sequences
Reference sequences used for building the phylogenetic tree were as follows: CPZ.CD.U42720, B.EU346273, B.FJ591428, B.AF493388, A1.GQ867597, A1.GU207098, A1.GU207120, A1.GU366132, 01_AE.GU207108, 01_AE.AY641924, 01_AE.AF280784, 01_AE.FJ007081, 02_AG.EU255307, 02_AG.AJ286947, 02_AG.EU822720, 02_AG.HM135491, 02_AG.FJ931331, 02_AG.EU330652, 02_AG.AY444244, 02_AG.AY847446, 02_AG.AJ313396, 02_AG.AY140630, 02_AG.AM181802, 02_AG.AJ286954, 02_AG.AJ313408, 02_AG.AM903424, 02_AG.AY847440, 02_AG.DQ166419, 02_AG.DQ297211, 02_AG.DQ321895, 02_AG.DQ452670, 02_AG.EF064471, 02_AG.EU177967, 02_AG.EU330798, 02_AG.EU330835, 02_AG.FJ549965, 02_AG.FJ931430, 02_AG.FN599782, 02_AG.GQ241013, 02_AG.GU207029, C.GQ462322, C.DQ351229, G.EU248320, G.GQ399618, F1.FJ771010, F2.FJ931229, HQ393248.MAR, HQ393249.MAR, HQ393251.MAR, HQ393256.MAR, HQ393261.MAR, HQ393266.MAR, HQ393279.MAR, HQ393311.MAR, HQ393321.MAR, HQ393322.MAR, HQ700006.MAR.
Footnotes
Acknowledgments
The authors wish to thank all the HIV-positive persons who participated in the study and all participating subjects and clinic staff at the Infectious Diseases Unit, Ibn Rochd University Hospital Center (Casablanca). This study was supported by the French Ministry of Foreign Affairs (Fond de Solidarité Prioritaire 2001/168 “Appui au Réseau de Surveillance des Résistances aux Antimicrobiens”) and by the Moroccan Association of the Fight Against Aids (ALCS). The authors are also grateful to Prof. Hakima Himmich, President of the ALCS and the Former Head of Infectious Diseases Unit, Ibn Rochd University Hospital Center.
Author Disclosure Statement
No competing financial interests exist.