
Abstract
Raltegravir is metabolized by glucuronidation via UDP-glucuronosyltransferase 1A1 (UGT1A1). We analyzed the genotypes of UGT1A1 (*6, *27, and *28) and their contribution to plasma raltegravir concentrations in 56 Japanese HIV-1-infected patients in the National Hospital Organization Nagoya Medical Center of Japan. Among the 56 patients, the UGT1A1 genotype in two patients was *6 homozygote. Heterozygous variants were found in 13 patients for *6 and in 11 patients for *28, while all of the patients were found to carry wild-type sequences at the position corresponding to the *27 allele. Plasma raltegravir concentration of a male patient with *6 homozygote (0.53 μg/ml) was modestly higher than that of patients with wild type (0.12 μg/ml) or *6 heterozygote (0.16 μg/ml). Another female patient with the *6 homozygote had a low plasma raltegravir concentration (0.03 μg/ml). Patients heterozygous for the *6 or *28 allele did not display significantly different plasma raltegravir concentrations compared to patients homozygous for the respective wild-type allele. Thus, in the present study, we showed that heterozygous reduced-function *6 and *28 alleles appear to have no significant effect on plasma raltegravir concentrations in Japanese HIV-1-infected patients. However, variability in raltegravir concentration and small patient population precluded a correlation between UGT1A1*6 homozygosity and plasma raltegravir concentration. To clarify the contribution of UGT1A1*6 or *28 polymorphisms to plasma raltegravir concentrations, further investigations on larger subject populations are required.
Introduction
R
Raltegravir is metabolized by glucuronidation via UDP-glucuronosyltransferase 1A1 (UGT1A1). The genetic polymorphism of UGT1A1 is known to be associated with UGT1A1 activity. To date, at least 113 variants of the UGT1A1 gene have been reported. 6 Among these variants, the *6, *27, *28, and *37 alleles are associated with reduced levels of UGT1A1. In particular, the *28 [(TA)7TAA] allele accounts for most of the UGT1A1 polymorphisms seen in the literature, and the level of UGT1A1 activity has been the focus of most studies. 7,8 On the other hand, among Asians, the *6 [211G > A] and *27 [686C > A] alleles are more commonly found in comparison with white populations, and the *37 [(TA)8TAA] allele is less common except for African populations. 8
In this study, we aimed to clarify the contribution of UGT1A1 polymorphisms to plasma raltegravir concentrations in Asian patients. Therefore, we analyzed the UGT1A1*6, *27, and *28 genotypes in Japanese HIV-1-infected patients, and then examined the correlation between each allele and plasma raltegravir concentrations.
Materials and Methods
Patients
A total of 56 Japanese HIV-1-infected patients who were treated with raltegravir-containing regimens at the National Hospital Organization Nagoya Medical Center, Japan, were examined for their allelic variants of UGT1A1*6, *27, and *28. The mean age and body weight of these patients (50 males and 6 females) were 50 years (range: 23–82 years) and 62.9 kg (range: 34–101 kg), respectively. Subjects were treated using raltegravir (400 mg, twice daily) in combination with other antiretroviral agents. The mean therapy duration was 15 months (range: 1–35 months). Drug adherence by each patient was confirmed by interview and viral load during raltegravir-containing therapy. The coadministered antiretroviral agent was etravirine in 12 patients, tenofovir/emtricitabine in 29 patients, abacavir/lamivudine in 9 patients, zidovudine/lamivudine in 3 patients, and others in 3 patients. At initiation of raltegravir-containing therapy, the mean CD4 cell count was 288 cells/mm3 (range: 3–725 cells/mm3) and the mean viral load was 211,632 copies/ml (range: <40–4,040,000 copies/ml).
This study was approved by the Institutional Review Board of the National Hospital Organization Nagoya Medical Center, and each subject provided written informed consent.
Genotyping
Genomic DNA was isolated from peripheral blood using a QuickGene SP kit DNA whole blood (Fujifilm, Tokyo, Japan). Genotyping of *6 and *27 in UGT1A1 was performed with a Taqman Drug Metabolism Genotyping Assay (Applied Biosystems, Foster, City, CA). Genotyping of *28 in UGT1A1 was performed using the primers described by Ehmer et al. 9 The detection run consisted of a hot start at 95°C for 10 min and 50 cycles of 92°C for 15 s and 60°C for 90 s (*6 and *27), or 50 cycles of 95°C for 15 s and 58°C for 60 s (*28). All assays were performed as 20 μl PCR mixtures containing 10 ng genomic DNA, 900 nM primers, 200 nM TaqMan minor groove binder (MGB) probes, and 12.5 μl Eagle Taq Master Mix with Rox (Roche, Mannheim, Germany) using the ABI 7300 Real-Time PCR system (Applied Biosystems, Foster City, CA).
Plasma raltegravir concentration
Blood samples were drawn between 11 and 16 h (mean, 13 h) after dosing. We selected this sampling time based on the 12-h trough previously reported in raltegravir (twice-daily dosing) pharmacokinetic studies. 12 Plasma was isolated by centrifugation (5 min at 3500×g) on the same day as blood sampling and stored at −80°C until analysis. Plasma raltegravir concentrations were determined using our previously reported LC-MS equipment and methodology. 10 For the present study, plasma raltegravir concentrations were determined from an average of three separate draws for each patient (range: 2–6 times/individual).
Results
Frequency of UGT1A1*6, *27, and *28 alleles
We analyzed the presence of genotypic variants (*6, *27, and *28) among the 56 patients recruited at the National Hospital Organization Nagoya Medical Center. Among the 56 patients, the UGT1A1 genotype in two patients was the *6 homozygote. Heterozygous variants were found in 13 patients for *6 and in 11 patients for *28, while all of the patients were found to carry wild-type sequences at the position corresponding to the *27 allele. Patients heterozygous for both *6 and *28 were not found in this study.
Correlation between UGT1A1 genotype and raltegravir concentration
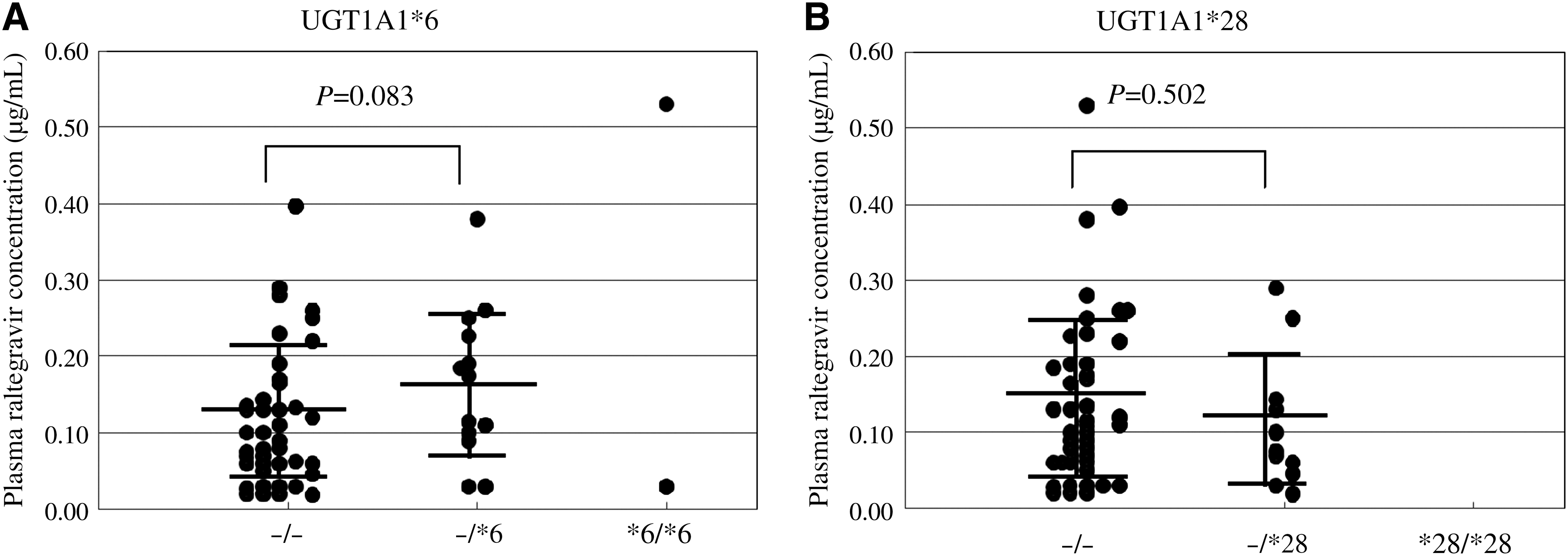
Among the 56 patients who were treated with raltegravir-containing regimens, only two (one male, one female) were found to be homozygous for the *6 allele. The male *6 homozygote patient had modestly higher plasma raltegravir concentration (0.53 μg/ml) than other patients who were wild type (0.12 μg/ml) or heterozygous (0.16 μg/ml) for the *6 polymorphism (Fig. 1A). The female UGT1A1*6 homozygote had a lower plasma raltegravir concentration (0.03 μg/ml); this patient had been treated with an etravirine-containing regimen. On the other hand, patients heterozygous for the *6 or *28 allele did not display significantly different plasma raltegravir concentrations when compared to patients homozygous for the respective wild-type allele (Fig. 1A and B).
Correlation between UGT1A1*6 genotype
Table 1 shows plasma raltegravir concentrations and patient characteristics sorted by the UGT1A1 genotype of the 56 patients. The body weights of the two patients with the *6 homozygote were lower than those of patients who were wild type or heterozygous for this allele, and this difference was statistically significant. However, the other differences in patient characteristics for each UGT1A1 genotype (*6 and *28) were not significant, indicating that these characteristics did not correlate with the differences in raltegravir concentration seen among UGT1A1 genotypes.
n.s., not significant (p>0.05). All of the patients were found to be wild type for the *27 allele (i.e., *27−/−).
Table 2 shows the relationship between UGT1A1 genotype (both *6 and *28) and raltegravir concentration in the 56 patients. Plasma raltegravir concentrations were 0.12 μg/ml (*6−/− *28−/−; n=30), 0.11 μg/ml (*6−/− *28−/+; n=11), and 0.16 μg/ml (*6−/+ *28−/−; n=13). There were no statistically significant differences in the plasma raltegravir concentrations between patients carrying wild-type alleles and those heterozygous for *6 or *28.
Discussion
The polymorphisms (*6, *27, and *28 alleles) associated with the UGT1A1 locus lead to deficiencies in UGT1A1 activity. As a result, individuals with these alleles may have higher plasma raltegravir concentrations. In fact, Wenning et al. 11 reported that plasma raltegravir concentrations are modestly higher in individuals with the UGT1A1*28 homozygote compared to those carrying the wild-type allele. Regrettably, we could not confirm this result because we identified no patients with the *28 homozygote among our 56 recruited patients. Within our patient sample, there were no statistically significant differences in plasma raltegravir concentrations between patients with wild-type and *28 heterozygous genotypes. Further assessment of the relationship between the UGT1A1*28 genotype and plasma raltegravir concentrations will require studies on additional subjects.
The UGT1A1*6 and *27 polymorphisms are commonly found among Asians, where the UGT1A1*6 polymorphism is more common than UGT1A1*28. 8 Among our 56 recruited patients, we found 2 patients with the *6 homozygote and another 13 patients with the *6 heterozygote. On the other hand, all 56 of our patients carried wild-type sequences at the position corresponding to the *27 allele. In the single male patient homozygous for *6, the plasma raltegravir concentration (0.53 μg/ml) was modestly higher than that seen in patients with wild-type alleles (0.12 μg/ml) or *6 heterozygosity (0.16 μg/ml). The single female patient homozygous for *6 had a lower plasma raltegravir concentration (0.03 μg/ml). Thus, in this study, we examined only a small number of patients with the *6 homozygote. In addition, the intraindividual variability in raltegravir concentration is known to be very large. 12 As a result of these limitations, we could not demonstrate any correlation between UGT1A1*6 homozygosity and plasma raltegravir concentration. This observation is similar to that of Neely et al. 13 who reported that the high degree of variability in raltegravir concentration and small population size appeared to obscure any pharmacogenomic effects on plasma raltegravir concentrations by the *28 allele.
Our results also indicated that heterozygosity for the reduced-function *6 and *28 alleles appeared to have no significant effect on plasma raltegravir concentrations in Japanese HIV-1-infected patients. Additional clarification of the contribution of the UGT1A1 *6 and *28 polymorphisms to plasma raltegravir concentrations will require further investigations with larger subject populations.
Footnotes
Acknowledgments
This study was supported in part by a Grant-in-Aid for Clinical Research from the National Hospital Organization to M.T.
Author Disclosure Statement
No competing financial interests exist.