
Abstract
We analyzed serum 25(OH) cholecalciferol [25(OH)D] levels and factors related to deficiency (<20 ng/ml) or insufficiency (<30 ng/ml) in a cohort of Spanish HIV-infected patients and compared them with an age- and latitude-matched population from another study. We prospectively assessed 25(OH)D deficiency/insufficiency in a cohort of 352 HIV patients during 2009–2010. Predisposing factors were recorded and their relationship to low levels was assessed by logistic regression; a nutritional survey examined intake, nutritional status, and sunlight exposure in a subgroup of 92 patients. We studied the correlation of 25(OH)D with parathyroid hormone (PTH) and alkaline phosphatase. Age-, sex-, and race/ethnicity-adjusted vitamin D deficiency (<20 ng/ml) was 44.0% (95% CI, 38.8–49.4%) and insufficiency (<30 ng/ml) was 71.6% (95% CI, 66.9–76.3). Deficiency was 16.4% more prevalent in our sample than in non-HIV-infected Spaniards. Lower sunlight exposure was the only factor related to lower levels in the lifestyle and nutritional survey (p=0.045). In multiple logistic regression, higher body mass index (BMI), black race/ethnicity, lower seasonal sunlight exposure, men who have sex with men (MSM), and heterosexual transmission categories, efavirenz exposure and lack of HIV viral suppression were independently associated with deficiency/insufficiency. These variables predicted 79% of cases [AUC=0.872 (95% CI, 0.83–0.91)]. Patients receiving protease inhibitors (PIs) [OR 4.0 (95% CI, 1.3–12.3); p=0.014] or NNRTI [OR 3.6 (95% CI, 1.7–11.2); p=0.025] had higher odds of increased PTH levels; this was significant only in 25(OH)D-deficient patients (p=0.004). As in less insolated areas, the prevalence of vitamin D deficiency/insufficiency was high in HIV-infected patients in Spain; among treated patients, levels were higher with PIs than with efavirenz.
Introduction
Vitamin D is considered a hormone with widespread effects; its deficiency has a wide impact, exceeding rickets and osteomalacia. There is evidence concerning its relationship to metabolic syndrome, diabetes, autoimmune diseases, arterial hypertension, and cancer. 1,2 It may even be considered a marker of cardiovascular disease. 3 The precise mechanism of the multiple effects of vitamin D in various tissues is unknown; the only common factor is the presence of vitamin D receptor (VDR) in many tissues.
To assess vitamin D status, 25-hydroxycholecalciferol [25(OH)D] is measured. Its serum concentration reflects dietary input, synthesis through sunlight skin exposure, and vitamin D conversion from liver fatty stores. 4,5
Recently reference values have been changed, and a serum level between 30 and 76 ng/ml is considered normal. Using this cutoff point, the prevalence of vitamin D deficiency is as high as 50–80% in the general population. 6,7
The interest in vitamin D in HIV infection relates to its immunomodulatory properties. Nuclear VDRs have been found in immune system cells, such as T, B, and dendritic cells. In immune system cells, 25(OH)D is converted to 1,25(OH)2D. 8 Recently, low vitamin D levels have been related to disease progression of HIV-AIDS and its complications. 9,10 Data from the EuroSIDA cohort, which follows 20,000 subjects, highlight the impact of vitamin D deficiency on global and AIDS and non-AIDS-related mortality. 11
In recent years data on severe vitamin D deficiency in HIV-infected populations in several countries have been published. Studies differ in their populations, measurement methods, and cutoff points, which hinders comparison and obtaining conclusions. This year, results of the SUN study have been presented. 12 At variance with most previous studies, the number of participants was high (n=672). The study compares vitamin D deficiency and insufficiency according to current criteria and a thorough analysis of potential risk factors for vitamin D deficiency and insufficiency has been performed. Vitamin D deficiency (less then 20 ng/ml) and insufficiency (20–30 ng/ml) rates were high, 29.7% and 70.3%, respectively. In HIV-infected patients, HIV virus-related factors and certain antiretroviral drugs contribute to vitamin deficiency, along with malnutrition, exercise, ethnic background, advanced age, and inadequate sun exposure.
HIV may diminish 25(OH)D through several mechanisms. Proinflammatory cytokines such as tumor necrosis factor (TNF)-α 13 drop levels, and macrophages and lymphocytes take up vitamin D as disease progresses. It is used in maturation and proliferation of T lymphocytes. 14 Both protease inhibitors (PIs) and nonnucleoside reverse transcriptase inhibitors (NNRTIs) interfere with vitamin D metabolism. 15,16 PIs block hydroxylation of 25(OH)D and bioactivation of 1,25(OH)2D, 2,14,16 whereas NNRTIs increase 25(OH)D and 1,25(OH)2D metabolism. 17
Five cross-sectional studies show that efavirenz (EFV)-based highly active antiretroviral therapy (HAART) is related to low vitamin D levels. 9,12,17 –19 Additionally, more robust evidence has been found in two retrospective and one prospective cohort studies of naive patients. 20 –22 Until the 2011 MONET 23 and ECHO III 24 clinical trials, there was no controlled trial-based evidence on a causal relationship of EFV in diminishing 25(OH)D levels. Only a single case series of Spanish HIV patients has been published. 25
We undertook this study to assess prevalence of vitamin D deficiency and insufficiency in HIV-infected adults in Spain (40° N) in HAART and to compare it with data on a Spanish noninfected, age-matched population from the same geographic area. 26 We have analyzed in our patients risk factors generally associated with vitamin D deficiency. Specifically, we assessed the influence of ethnic background, the use of HAART, and the type of antiretroviral drugs used on vitamin D metabolism.
Materials and Methods
An observational cross-sectional study of a clinical population-based cohort of 450 HIV-infected patients was conducted. In 2009 and 2010, 352 patients diagnosed with HIV infection who were followed-up ay the infectious disease clinic of the Hospital Severo Ochoa, a public urban hospital close to Madrid, were recruited. Patients receiving biphosphonates, vitamin D supplements, or other therapies for bone metabolism were excluded. We analyzed data of blood chemistries, physical examination, and a nutritional and lifestyle survey. The database had been approved by the institutional ethical review board and patients provided verbal informed consent for data collection and use.
For this study we assessed comorbidities related to vitamin D deficiency or insufficiency, as well as HIV infection-related variables.
Laboratory methods
Serum 25(OH)D levels were assessed with a Cobas e 411 multichannel analyzer employing electrochemiluminescence (ECL) technology (Roche), intact PTH with IMMULITE 2000, a solid-phase two-site chemiluminescent immunoassay (Siemens), CD4 count by means of flow cytometry, and HIV viral load using with real time polymerase chain reaction (PCR) (Taqman); less than 50 RNA copies/ml was considered undetectable. Other chemistries were assayed with standard automated techniques.
Based upon previous studies, we chose <30 ng/ml to define vitamin D insufficiency and <20 ng/ml for deficiency. Intact parathyroid hormone (PTH) was considered increased when its plasma level was above 66 pg/ml.
To compare the prevalence of vitamin D deficiency and insufficiency with that of an age-matched Spanish population of the same geographic area we used data published by M. Calatayud. 26
In our study a subgroup of cohort subjects (n=92) agreed to participate in a nutritional and lifestyle substudy. A nonvalidated survey about nutrition and lifestyle was administered by a certified nutrition specialist, gathering information on sunlight exposure, use of UVA cabins, dietary vitamin D intake, vitamin supplements, sunscreens, and exercise.
Statistical analysis
Vitamin D deficiency (<20 mg/ml) and insufficiency (<30 ng/ml) estimates with 95% CI were performed, both global and adjusted for age, ethnic background, and gender.
We divided patients in tertiles according to vitamin D levels. Qualitative variables were compared by χ2 or Fisher's exact tests; for continuous variables nonparametric Kruskal–Wallis was used.
Correlation between 25(OH)D, PTH, alkaline phosphatase (excluding subjects with alanine aminotransferase ≥40 IU), and CD4+ cell count was analyzed with Spearman's correlation test.
The effect of putative vitamin D deficiency predictors was studied by logistic regression. Variables with a p value of <0.20 in univariate analysis were included in the multiple logistic regression model. Thereafter, a reduced model was selected using backward elimination. To include all cases in multivariable analysis, unknown values were replaced by assigned values using the expectation maximization algorithm. Simple linear regression was used to assess the difference of change in the level of vitamin D related to the variables found in the simplified logistic regression. Factors associated with the upper quartile of alkaline phosphatase and iPTH were studied by means of logistic regression.
Associations were considered significant if p<0.05 in a two-tailed test. Statistical analysis was performed with SPSS version 15.0 (SPSS Statistics).
Results
Table 1 shows characteristics of study participants. The median 25(OH)D level was 22 ng/ml (IQR 14.22–31.7 mg/ml). Samples were classified in tertiles according to vitamin D level. The upper tertile included a significant excess of white race subjects (p=0.001) and former intravenous drug users (IDUs) (p=0.0001), and an increased proportion of blood samples drawn in summer (p=0.0001) and patients on antiretroviral therapy (0.006).
Baseline Characteristics of the Study Sample
IQR, interquartile range; IDU, intravenous drug user; MSM, men who have sex with men; BMI, body mass index; ART, antiretroviral treatment.
Among study participants, the age-, sex-, and race-adjusted prevalence of vitamin D deficiency (25[OH]D <20 ng/ml) was 44.0% (95% CI, 38.8–49.4), and the prevalence of vitamin D insufficiency (<30 ng/ml) was 71.6% (95% CI, 66.9–76.3). Only in 28.4% (95% CI, 23.7–33.1) could vitamin levels be considered optimal (≥30 ng/ml).
Compared with the general Spanish adult population, 26 the percentage of subjects with optimal levels of vitamin D was higher in our sample, although the difference was not statistically significant. However, vitamin D deficiency was more prevalent in the study subjects (16.4%; 95% CI, 6.8–26.09; p=0.001).
Table 2 shows results of the dietary intake and lifestyle questionnaires filled out by 92 subjects. Among many factors studied, only increased sunlight exposure showed statistically significant differences toward optimal vitamin D levels (p=0.045).
Results of Nutritional and Lifestyle Survey
Rda, recommended dietary allowance.
Of the 352 subject studies, 139 (39.5%) were taking PIs, 129 (36.6%) NNRTIs, and 21 (6%) received coformulated zidovudine/lamivudine/abacavir. There were statistically significant differences in vitamin D levels, which were highest in patients on PIs monotherapy and lowest in those receiving EFV or zidovudine/lamivudine/abacavir. Figure 1 shows the percentage of patients with vitamin D deficiency or insufficiency.
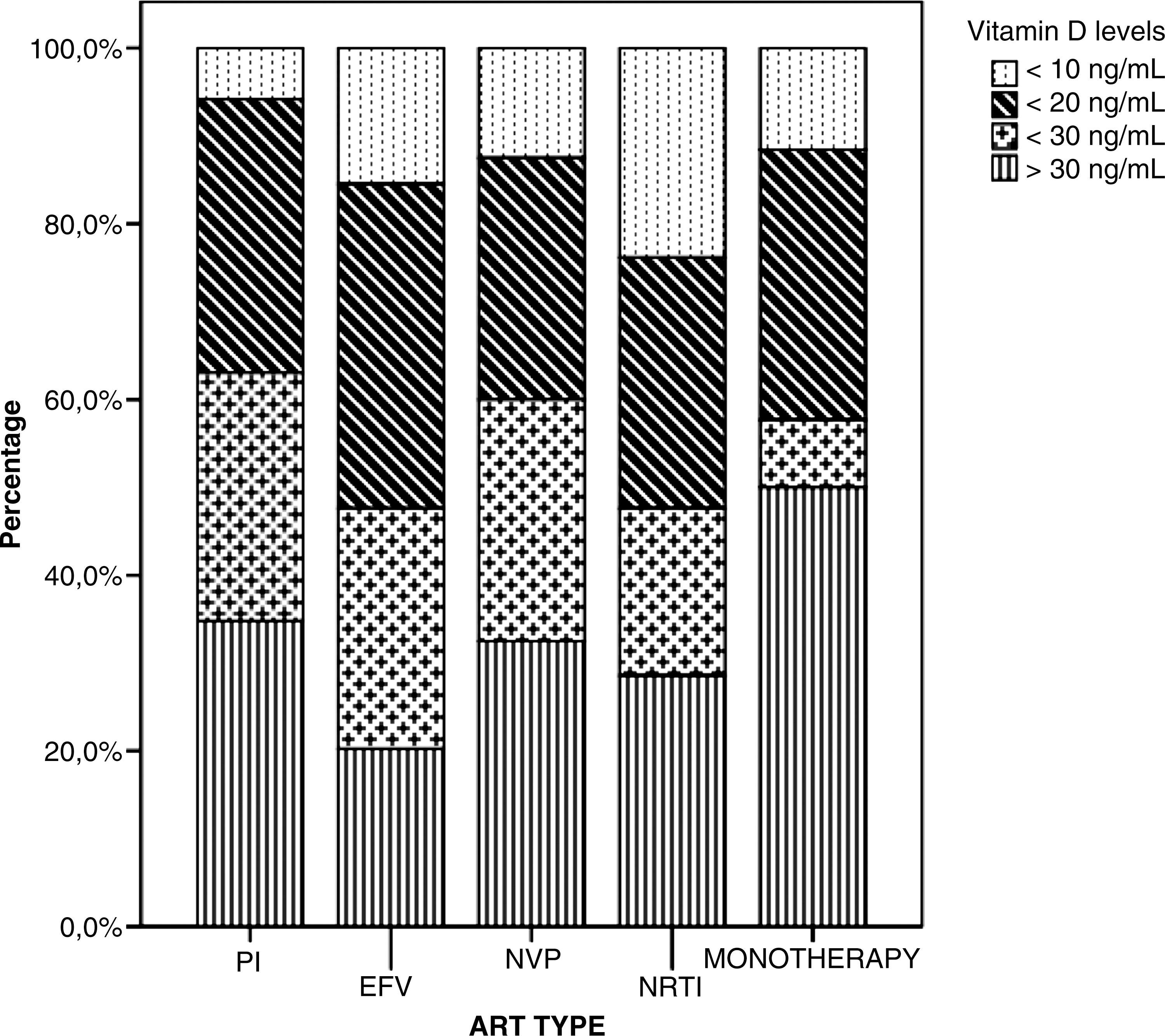
Vitamin D levels related to antiretroviral (ART) use.
Univariate and multivariate analysis of vitamin D deficiency- and insufficiency-associated factors in HIV-infected patients (Table 3)
Baseline Demographic and Clinical Factors Associated with Vitamin D Insufficiency or Deficiency
IQR, interquartile range; BMI, body mass index; ART, antiretroviral treatment; ALT, alanine aminotransferase; HDL, high-density lipoprotein; HOMA, homeostatic model assessment (for insulin resistance); PI, protease inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; MSM, men who have sex with men; IDU, intravenous drug user. * p<0.05.
In a univariate analysis, the absence of antiretroviral therapy (ART), nonsuppressed viral load, shorter duration of HIV infection, and lower CD4+ cell counts were associated with increased odds of vitamin D deficiency or insufficiency.
Regarding ART, EFV exposure was associated with significantly higher odds of vitamin D insufficiency or deficiency, whereas IPs exposure seemed protective (p=0.014). We did not observe significant associations between vitamin D insufficiency or deficiency and NRTI, tenofovir, or nevirapine exposure.
In univariate analysis of non-HIV-related factors, black race/ethnicity, lesser UV exposure (lower levels in spring/fall than in summer/winter), increased body mass index (BMI), GPT <40 IU, the absence of hepatitis C virus (HCV) coinfection, and estimated GFR ≥60 ml/min/1.73 m2 (MDRD) were associated with increased odds of vitamin D insufficiency or deficiency (p<0.05).
In logistic multiple regression, factors independently associated with increased odds of vitamin D insufficiency or deficiency were BMI, black race/ethnicity, less UV exposure in winter and spring, men who have sex with men (MSM) and heterosexual HIV transmission categories, EFV exposure, and unsuppressed HIV viral load (Table 4).
Multiple Linear Regression Analysis of Correlates of 25-Hyroxyvitamin D Concentrations
MSM, men who have sex with men; IDU, intravenous drug user; BMI, body mass index; HCV, hepatitis C virus; ALT, alanine aminotransferase; ART, antiretroviral treatment; EFV, efavirenz; PI, protease inhibitor. * p<0.05.
Using this predictive model, which included the aforementioned variables, the sensitivity of predicting vitamin D insufficiency or deficiency (25[OH]D <30 ng/ml) was 87.3%, the specificity was 58%, and the discriminatory power was 79%. The final model has an acceptable power for classification, since it is higher than 75%. Its receiver-operating characteristics (AUC) is 0.872 (95% CI, 0.83–0.91).
In a multiple linear regression model including the same independent variables as the abovementioned logistic regression model, the significance of the association of heterosexual and MSM transmission categories with 25(OH)D deficiency or insufficiency is lost (p=0.153 and 0.187). Years since HIV infection diagnosis and absence of ART are significantly associated with low 25(OH)D, whereas higher levels are found in HCV-infected subjects and in those with ALT ≥40 IU. The remaining significant variables in the logistic regression model retained their independent association with serum 25(OH)D concentration.
Eighty-eight patients (25%) had high PTH levels (upper quartile, ≥66 pg/ml). Among subjects with vitamin D insufficiency, 66 (26.2%) had elevated PTH levels. The odds of high levels of PTH were higher in patients receiving PIs (OR 4.05; 95% CI, 1.33–12.3; p=0.014) or with NNRTI (OR 3.6; 95% CI, 1.7–11.17; p=0.025) than in untreated patients. PTH levels in PI-treated patients were not significantly higher than in NNRTI-treated patients (p=0.72).
Tenofovir-exposed patients had higher PTH levels, but this difference was significant only in patients with vitamin D insufficiency (p=0.004). The significant increase in alkaline phosphatase in patients receiving tenofovir was independent of vitamin D status. There were no differences in phosphate and calcium levels. We observed a negative correlation between serum PTH and 25(OH)D levels (r=0.098; p=0.048) and a positive one with alkaline phosphatase (r=0.0105; p=0.024).
Discussion
Our cohort's vitamin D deficiency or insufficiency rates, 71.59%, are very similar to prevalence rates of other series of HIV-positive patients studied in areas of lower insolation. 12,17,18,21 Another recent paper observed a 74% rate of vitamin D insufficiency in postmenopausal HIV-infected women, similar to the control group of African-American women, the category of highest vitamin D insufficiency prevalence. 27
A 71.59% rate of vitamin D deficiency or insufficiency in our cohort of HIV-infected adults of the Hospital Severo Ochoa is high, and close to the prevalence observed in the general population of the Comunidad de Madrid (Spain), as shown by Calatayud. 26 This latter study was performed in a sample of similar age recruited in the same geographic area, in May and June. Although the prevalence of vitamin deficiency or insufficiency was similar in both studies, we would like to emphasize the fact that deficiency—probably more clinically important—was significantly more prevalent in HIV patients (16.4%; 95% CI 6.8–26.1, p=0.001). Our findings are similar to rates of the general population elsewhere. 1,7,28
A lower limit of the reference range has recently been set at 30 ng/ml. There are several reasons for this value. In studies performed several years ago, PTH levels were found to be increased in the population whenever 25(OH)D levels dropped below this level. 1 More recent data show optimal calcium absorption when the 25(OH)D level is 32 ng/ml or higher. 4 Another measure to define an optimal 25(OH)D status is the value at which no further increase of 1,25(OH)2D is noted after administration of vitamin D. When 25(OH)D levels were below 25 and 30 ng/ml, increases in 1,25(OH)2D were found. 29
Findings from a nutritional and lifestyle survey highlight the relevance of sunlight exposure. Only high exposure, which was linked to outdoor jobs, was related to optimal vitamin D levels.
Considering the prevalence of vitamin D insufficiency, the analysis of the relationship between certain antiretroviral drugs and vitamin D metabolism seems very interesting. Patients on darunavir/ritonavir or lopinavir/ritonavir monotherapy had greater immune recovery, longer HIV infection duration, and closer to optimal vitamin D levels. Our results were similar to those of the MONET study. 23 This exploratory findings should be confirmed in future larger studies on bone health in effective boosted PI monotherapy.
Data on EFV and vitamin D deficiency have accumulated in recent years. Our data show that the odds of vitamin D insufficiency or deficiency increased 2.87 times with the use of this drug, and levels were 5.2 ng/ml lower than with other therapeutic regimes. This is not an NNRTI class effect on vitamin D metabolism. At variance with others, 12 we did not observe a relationship between tenofovir exposure and higher vitamin D levels.
We were unable to show a relationship between HIV infection, degree of immune suppression or AIDS diagnosis, and vitamin D levels, but we did observe lower levels of 25(OH)D in patients with unsuppressed viral load. Other factors significantly associated with 25(OH)D deficiency or insufficiency in multivariate analysis, such as being overweight, black race/ethnicity, and season, are in accordance with previous literature. A surprising finding of our study is higher vitamin D levels in former IDUs. We have no explanation for this; more frequent outdoor jobs and less use of EFV in this transmission category could have a role.
The final model predicts vitamin D deficiency or insufficiency in HIV-infected patients with high discrimination power (79%).
Among multiple comorbidities and drugs, only diabetes mellitus showed an association with lower levels of vitamin D (p<0.10). Although not statistically significant (p=0.089), diabetes mellitus was associated with a clinically significant increase in the odds for vitamin D insufficiency (OR 4.5; 95% CI 0.8–24.9). Osteocalcin production requires adequate vitamin D levels, and recombinant osteocalcin administration may revert to hyperglycemia and hyperinsulinemia 30 ; this points to a link between vitamin D, bone, fat, and glucose metabolism.
Among NRTIs, tenofovir produces major concerns on bone health and vitamin D metabolism. Tenofovir-based regimens in naive 31,32 and nonnaive 33 patients are associated with decreases in bone mineral density (BMD). The precise mechanisms of this loss are not known, but the Swiss Cohort has described an increased fractional excretion of phosphate in the urine in 30–40% of patients, and an increase in alkaline phosphatase, a marker of bone remodeling. 34 Two recent cross-sectional studies described a significant increase in median PTH levelsin healthy individuals with vitamin D deficiency. 35,36 We had similar findings: PTH was significantly higher in tenofovir-exposed patients, but only in those with vitamin D insufficiency. However, the significant increase in alkaline phosphatase was independent of vitamin D level. Assessing the contribution of vitamin D, PTH, calcium, phosphate, and certain antiretrovirals such tenofovir to BMD seems advisable.
Although vitamin D insufficiency is widespread, identifying its predictors in HIV-infected patients, such as efavirenz exposure and nonsuppressed viral load, will make it possible to identify those patients at highest risk. The latest European Guidelines for treatment of HIV-infected adults in Europe (October 2011) advise screening patients at risk of vitamin D deficiency. 37
Our study has several limitations. The absence of an HIV-negative comparison group limits reaching conclusions on prevalence rates in HIV-positive outpatients. Recruitment of patients in a single hospital with specific geographic and social characteristics in his catchment area may limit the external validity for the whole population living in Spain. The cross-sectional design prevents the establishment of causal relationships. Most patients had fairly good CD4+ cell counts, which may have an impact on the results.
Footnotes
Acknowledgments
We have obtained substantial assistance from Susana Pastor in data retrieval and from Rebeca Sanz in performing the nutritional survey.
Author Disclosure Statement
No competing financial interests exist.