
Abstract
Human T-lymphotropic virus type 1 (HTLV-I) is an important global health problem in the world mainly in the endemic areas of HTLV-I infection. It was previously reported that Mashhad, in northeastern Iran, is a new endemic region of HTLV-I. The aim of this study was to examine the prevalence and phylogenetic analysis of HTLV-I in Sabzevar, located in the southeast of Mashhad. In this cross-sectional study 1445 individuals were selected by multistage cluster sampling. Serum samples were screened for anti-HTLV-I antibody using enzyme-linked immunosorbent assay (ELISA); all of the ELISA-positive samples were confirmed by polymerase chain reaction (PCR). Long terminal repeat (LTR) sequencing was carried out to determine the type of HTLV-I in Sabzevar. In the primary screening by ELISA, 26/1445 (1.8%) of those sampled were reactive for HTLV-I antibody. Twenty-four out of 26 samples were confirmed HTLV-I infection by PCR (24/1445). The overall prevalence of HTLV-I infection in Sabzevar is 1.66%. The prevalence of the virus infection in men and women was 2.42% (11/455) and 1.31% (13/989), respectively. Seroprevalence was associated with age, increasing significantly among those older than 30 years (p=0.015), and a history of surgery (p=0.002), imprisonment (p=0.018), and hospitalization (p=0.005). Three out of 24 positive HTLV-I samples were selected for sequencing and phylogenetic analysis of LTR. The results showed that HTLV-I in Sabzevar belonged to the cosmopolitan subtype. The present study showed Sabzevar is a new endemic area for HTLV-I infection. Our study emphasizes that systemic HTLV-I screening of blood donors in Sabzevar and other cities in Khorasan province is important and should be taken into account.
Introduction
Human T-lymphotropic virus type 1 (HTLV-I) is an envelope, double-stranded RNA type C retrovirus that is associated with two main type of diseases: HTLV-I-associated myelopathy/tropical spastic paraparesis (HAM/TSP) and adult T cell leukemia (ATL). 1,2 Infection with HTLV-I is one of the important global health problems, particularly in the endemic areas of HTLV-I infection. It is known that HTLV-I has spread worldwide; however, it is endemic only in distinct regions such as southwestern Japan, 3,4 the Caribbean islands, 5 Central and South America, 6,7 and west of Africa. 8
We have previously reported that the northeast of Iran, Mashhad, the capital of Razavi Khorasan province, is a new endemic region of the virus and the prevalence of HTLV-I infection is estimated to be 2.1% in the general population and 0.44% in blood donors. 9,10 Epidemiologic studies in other parts of Iran estimated the prevalence of HTLV-I infection to be 0.34% in the general population of Uromia in the northwest and 0.62% in Chaharmahal and Bakhtiari in the southwest. 11,12
Furthermore, studies in some specific populations of Iran including both thalassemics and hemodialysis patients have shown high HTLV-I prevalence in these subjects (about 6.8%). 12 The high prevalence of HTLV-I infection has also been reported in thalassemic patients in Shiraz (1.25%) and Zahedan (1.6%). 13,14 Phylogenetic analysis of the viral DNA sequence has indicated that the HTLV-I present in Mashhad belongs to the HTLV-I cosmopolitan “A” subtype. 15
The sporadic cases of HTLV-I carriers and HAM/TSP patients in other cities of Razavi Khorasan province, including Sabzevar, suggest that this virus could be present in this city. The aim of this study was to investigate the prevalence of HTLV-I infection in Sabzevar, an important ancient city in the northeast of Iran. Phylogenetic analysis was also carried out to determine the type of the virus in this city. The association between HTLV-I infection and risk factors of HTLV-I infection such as age, sex, and socioeconomic status was also examined.
Materials and Methods
Study design
This cross-sectional study was conducted in the city of Sabzevar in 2008. From all 10 areas of the city according to the Urban Health Centers registries, 1445 apparently healthy residents were selected by multistage cluster sampling. Three clusters in each area were selected proportional to their population. A questionnaire was provided for data collection on demographic and clinical information and the risk factors for HTLV-I acquisition. The study was approved by the ethics committee of Mashhad University of Medical Sciences (MUMS) and Sabzevar University of Medical Sciences. Informed consent was obtained from each participant or the next of kin before any interview was conducted.
Serologic and confirmation tests
Six milliliters of venous blood samples was taken from each individual. Serum was separated and DNA was extracted. Both samples were kept at −20°C before using. Serum samples were screened for anti-HTLV-I antibody using enzyme-linked immunosorbent assay (ELISA; Dia Pro Diagnostic bio probe, Italy) according to the manufacturer's instruction. All of the ELISA-positive samples were confirmed by polymerase chain reaction (PCR).
PCR was also carried out on all positive ELISA samples for further confirmation of HTLV-I infection. Briefly, genomic DNA was extracted from peripheral blood mononuclear cells (PBMCs) using an available commercial kit (Blood mini kit, Qiagen, Germany). PCR amplification was performed in a 25 μl reaction containing 20 mM Tris-HCl (pH 8.4), 100 mM KCl, 2 mM MgCl2, 200 mM dNTPs, 0.5 U Taq DNA polymerase, 10 pmol/μl of each specific primer Tax Forward (5′-AGGGTTTGGACAGAGTCTT-3′), Tax anti-forward (reversed) (5′-AAGGACCTTGAGGGTCTTA), LTR forward (5′-CATAAGCTCAGACCTCCGGG-3′), LTR anti-forward (5′-GGATGGCGGCCTCAGGTAGG-3′), and genomic DNA (50–100 ng). PCR consisted of initial denaturation at 94°C for 4 min, followed by 35 cycles of 94°C for 50 s, 60°C for 50 s, 72°C for 1 min, and a final extension at 72°C for 5 min. PCR products were analyzed on 2% agarose gel stained with ethidium bromide, and evaluated under UV light. The sizes of PCR products were estimated according to the migration pattern of a 100-bp DNA ladder.
DNA sequencing and phylogenetic analysis
For sequencing and phylogenetic analysis, the long-terminal repeat (LTR) region of proviral DNA was amplified by PCR. The LTR proviral (777 bp) was divided into two overlapping fragments (GenBank accession number J02029.1). PCR amplification was performed in a 25 μl reaction containing 20 mM Tris-HCl (pH 8.4), 100 mM KCl, 25 mM MgCl2, 10 mM dNTPs, 0.5 U Taq DNA polymerase, and 10 μmol/liter of each specific primer LTR-A (5′-TTCTGACAATGACCATGAGC-3′), LTR-A anti-forward (5′-GCGCgTGAAGGAGAGATG-3′), LTR-B forward (5′-GCTCGCATCTCTCCTTCAC-3′), and LTR-B anti-forward (5′-CGCTACGGGAAAAgATTTGG-3′). The protocol for PCR was as follows: initial denaturation at 94°C for 4 min, followed by 35 cycles of 94°C for 45 s, 54°C for 45 s, 72°C for 1 min, and a final extension at 72°C for 7 min. PCR products were purified and double-stranded sequencing was carried out by Seq Lab Company, Germany.
All the fragments that resulted from sequencing by both LTR-AF/R and LTR-BA/F were combined to build the longest possible contig. Overlapping nucleotides in the binding site for primers LTR-AR and LTR-BF were used for contig assembly by Geneious software (Biomatters Ltd., Auckland, New Zealand). This contig was finally used for BLAST search and the first 50 or 25 hits were used for phylogenetic analysis. The phylogenic (maximum likelihood) tree was built using PHYLM v2.4.5 16 integrated inside Geneious software. The model of nucleotides substitution was HKY85 and the stability (robustness) of the tree was evaluated by bootstrap test with 100 data sets.
Statistic analyses
Descriptive data were summarized as mean, standard deviation, and/or percents and were analyzed by SPSS 16.0 using Chi square and t tests. In addition, logistic regression analysis was applied to assess factors related to HTLV infection. A p value <0.05 was considered statistically significant.
Results
A total of 1445 individuals ranging in age from 5 to 88 years (mean age 36.6±15.6) were included in this study. Nine hundred and ninety (68.5%) were women and 455 (31.5%) were men; the ratio of women to men was 0.45. In the primary screening by ELISA, 26 (1.8%) were reactive for HTLV-I antibody. All positive samples were examined by PCR, of which 92.31% (24/26) were positive. According PCR results, the overall prevalence of the HTLV-I infection in the study population was 1.66% (24/1445) (CI 95% 1.07–2.46). The HTLV-I rate of infection for men was 2.42% (11/455) and for women was 1.31% (13/989). No significant differences in HTLV-I seroprevalence were observed between men and women (p=0.12).
In univariate analysis (Table 1), seroprevalence was associated with age, increasing significantly among those older than 30 years (p=0.015), history of surgery (p=0.002), imprisonment (p=0.018), and hospitalization (p=0.005). In the logistic regression analysis (Table 2), history of imprisonment was the only variable that had a significant association with the infection (p=0.004).
Sociodemographic and Clinical Factors Related to HTLV-I Infection in the General Population of Sabzevar, Iran, 2009
Including Turk, Kurd, and Arab.
Logistic Regression Analysis of the Association of HTLV-1 Infection with Selected Variables, Sabzevar, Iran, 2009
Three out of 24 positive HTLV-I samples were selected for sequencing and phylogenetic analysis of LTR. The assembled contig (HTLV-I/Sab-Ir, isolated from Sabzevar, Iran) turned out to be a subgroup with cosmopolitan subgroup HTLV-Ia along with the sequences previously reported to have originated from Iran, Kuwait, and Mashhadi Jews in Israel (Fig. 1). These records were clustered together and became separated from the other BLAST hits reported from the other parts of the world including Central Africa, South Africa, Peru, Japan, the United States, and Brazil. 17 –25 HTLV-I/Sab-Ir was 100% similar [BLAST search E-value=0, Score=756, Bitscore=1397.19, Identities=756/756 (100%), Positives=756/756 (100%), Gaps=0/756 (0%)] to nucleotides 924–1679 of record AF003010 in GenBank, which was isolated from an Iranian patient with mycosis fungoides in Germany. 26 In alignment analysis, three to five mismatches were detected between HTLV-I/Sab-Ir and the other hits with the same geographic origin including Mashadi Jews. The presence of an A in motif CCCCCTAAAGACAA instead of G is the signature of all these hits from Iran, Kuwait, and Mashadi Jews in Israel. This change removed the restriction site for a few enzymes including Eco57I, AcuI, Eco57MI, MboII, BbsI, BpiI, BpuAI, and Bstv2I. The presence of a G rather than an A in motif ATGTTTGTCGAGCCGCCCT is the other common feature among these hits, which was shared with hits AY040796 and AY818430 isolated from natives of British Colombia in Canada and one patient in Central Africa, respectively (Fig. 2).

Phylogenic analysis for the long terminal repeat (LTR) region of HTLV-I provirus isolated from a sample of patients in Sabzevar, Iran. DNA extraction, PCR amplification of the LTR region, and purification of PCR product were carried out. DNA was then sequenced and the overlapping fragments were assembled in a 787-nucleotide contig using Geneious software. This contig was used for a BLAST search and the geographic origin of each BLAST hit was extracted from either the comments inside the GenBank record or from the literature in which the sequence was published. The unrooted phylogenic (maximum likelihood) tree was built using the PHYLM algorithm integrated inside Geneious software. The position of HTLV-I/Sab-Ir is indicated by an arrow in the tree. The geographic region from with the majority of hits in each cluster have been reported is also mentioned next to each cluster. Branches are labeled with the accession number of each hit in GenBank followed by the geographic origin. Bootstrap proportion values are shown for each branch.
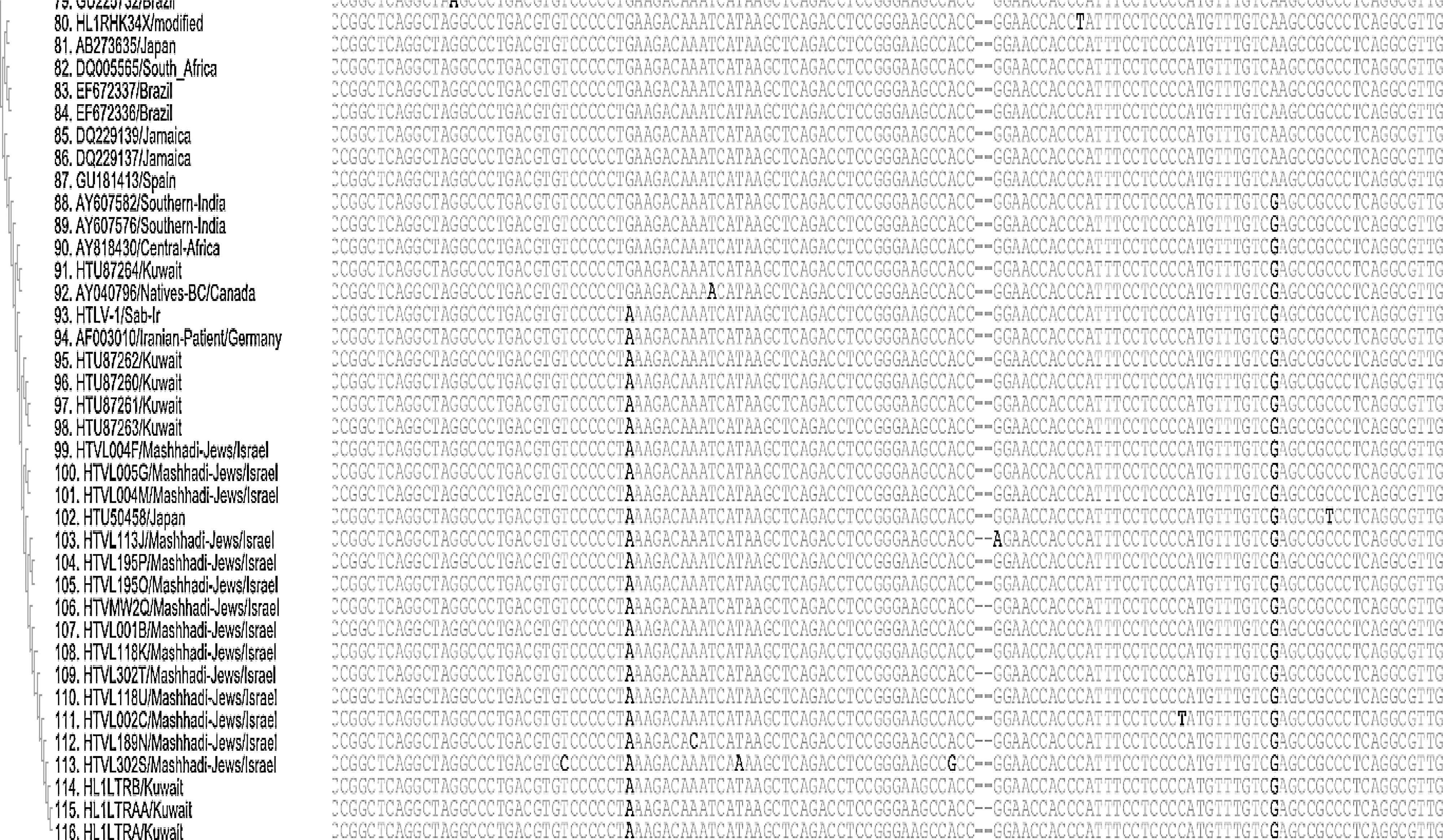
Alignment view of the phylogenetic tree. The variations among hits from the Middle East region (Iran, Kuwait, and Mashhadi Jews in Israel) and other parts of the world are highlighted.
This change, however, creates a restriction site for TaqI, BplI, CviJI, and CviKI-1. HTLV-I/Sab-Ir was highly similar (99%) to the record AY818430 [Blast search E-value=0, Score=742, Bitscore=1371.33, Identities=752/757 (99%), Positives=752/757 (99%), Gaps=0/757 (0%)]. This record represents the LTR region of the HTLV-I strain 2472LE LTR isolated from a patient in Central Africa and belongs to the only globally disseminated HTLV-I. 27
Discussion
Several sporadic cases of a T cell leukemia link to HTLV-I have been reported among immigrants to Israel and Germany who were from Mashhad. 28,29 It has been reported that 0.3–3.4% of the general population in Iran was infected with this virus. 30 So far, Neishabour (3.4%) and Mashhad (3%) have the highest HTLV-I prevalence rate in Iran. 31,32 However, the infection rates and the risk factors associated with HTLV-I infection in other important cities in the vicinity to Mashhad have not been assessed. Routine screening procedures of HTLV-I in blood donors in Khorasan Razavi province by the Blood Transfusion Center in Mashhad indicated that the virus is present in Sabzevar; thus, we examined the seroepidemiology of HTLV-I infection in a large representative sample of individuals of all ages selected from all districts in Sabzevar. The results demonstrated that the overall prevalence of HTLV-I infection was 1.66%; therefore, this city is considered to be a new endemic region of HTLV-I in Iran. Phylogenetic analysis showed that the HTLV-I subtype circulating in Sabzevar belonged to the cosmopolitan subtype, suggesting that the origin of the virus is the same as in Mashhad.
Sabzevar is the second largest city in the Razavi Khorasan province and it is approximately 220 km west of Mashhad (Fig. 3). The Royal Road (the major road in the Persian Empire), the Ritual Road, the Silk Road, and the Eurasian Route passed through Khorasan province and its cities, especially Mashhad and Sabzevar. This city was completely ruined after the attack of the Mongols and reconstructed many times throughout history. Sabzevar has become one of the fastest growing cities in the province with an estimated population of 214,582 in 2006. The entry of the HTLV-I virus in Mashhad, Neishabour, and Sabzevar is not clear; however, it seems that the virus may have entered through one of the following route: trade and skill road, an invading group such as the Mongols, pilgrims to the holy Muslim shrine, and African slaves. 9 Slavery seems more likely to have introduced the virus to these cities, because it has been widely practiced even before the rise of Islam in these cities. It has been suggested that the endemicity of the virus depends on variable factors such as environmental, social, behavioral, and cultural. 33

Mashhad and Sabzevar geographic location.
Despite the common origin and similarity of the virus in the region, different prevalences of HTLV-I have been reported in countries near Iran such as Kuwait, Iraq, and Turkmenistan. 34 –36 Furthermore, the social interaction among countries such as international trade, tourism, and pilgrimage seems to be playing a pivotal role in virus distribution. 37 In fact, the real reason for the extreme variation of the prevalence of HTLV-I in the continents, the countries, or even in different parts of a country is a challenging issue; thus, it is difficult to explain the difference in the prevalence of HTLV-I in Mashhad and Sabzevar, although it is more likely that pilgrimage might have a role in this issue. Therefore, it is necessary to perform large seroepidemiologic studies in other cities of Khorasan province to determine the seroprevalence of HTLV-I in this part of Iran.
Our results demonstrated that HTLV-I infection increases with age, particularly among those older than 30 years; this is similar to the previous cross-sectional study in Mashhad, which suggested that HTLV-I prevalence increases among those older than 35 years. 9 It has been shown that HTLV-I seroprevalence increases with age 38,39 and is higher among subjects more than 40 years than in those less than 40 years. 40 Sexual contact is more likely to be the primary route of virus transmission after age 30 years and breastfeeding during infancy has a small role in HTLV-I transmission. 41,42
Although the rate of infection is associated with age, other variables such as marital status, breastfeeding, and literacy are not risk factors for HTLV-I transmission. In this study, a greater prevalence of infection was associated with imprisonment, hospitalization, and a history of surgery, which is consistent with previous studies that reported that the virus is transmitted through contaminated needles and syringes among injecting drug users and following surgery. 43 HTLV-I transmission has occurred following surgery; however, income level, ethnic background, and place of birth had no significant effect on the rate of HTLV-I infection.
In conclusion, the present study showed that Sabzevar is a new endemic area for HTLV-I. It is clear that systemic HTLV-I screening of blood donors in Sabzevar and the other cities of Khorasan province should be taken into account. Furthermore, HTLV-I screening of pregnant women in this city will decrease the risk of HTLV-I infection and appropriate counseling regarding the risk of HTLV-I transmission by prolonged breastfeeding can be recommended for those pregnant women who are infected by the virus. Educational programs in Sabzevar are needed to prevent HTLV-I sexual transmission for those who are of a sexually active age. Considering the risks associated with HTLV-I infection, similar seroepidemiologic studies need to be conducted in other parts of Khorasan province to identify the prevalence of the virus in this region of Iran as a first step toward controlling the infection.
Footnotes
Acknowledgments
We would like to thank the Vice Chancellor of Research of Mashhad and Sabzevar Universities of Medical Sciences for financial support. The authors thank Dr. Fabiola Martin of York University for critical reading of the manuscript and helpful suggestions.
Author Disclosure Statement
No competing financial interests exist.