
Abstract
The emergence of viral-resistant strains is a major problem for the medical management of HIV-infected individuals. The aim of this study was to characterize viral subtypes and drug-resistance mutations (DRMs) in HIV-1 isolates from patients failing antiretroviral therapy (ART). A total of 45 HIV-1-infected patients failing ART were enrolled. The viral RT and Prot genes were amplified and sequenced to determine subtypes and potential DRMs. The subtype distribution was 74% subtype B, 11% subtype A, 9% CRF02-AG, 4% subtype G, and 2% subtype C. Virus samples from 34% of the patients had no DRM while 53%, 27%, and 2% of samples carried at least one DRM conferring resistance to drugs of one, two, or three classes, respectively. DRMs were observed in 50% of the patients infected with non-B strains. The prevalence of nucleoside transcriptase inhibitor (NRTI) mutations was 48%, M184V being largely predominant. The prevalence of nonnucleoside reverse transcriptase inhibitor (NNRTI) mutations was 13%, with K103N present in 57% of samples from NNRTIs-exposed patients. The prevalence of protease inhibitor (PI) mutations was 22%, with major mutations V82A and M46I seen in 16% and 11% of viruses from PI-exposed individuals, respectively. Our study shows the emergence of DRMs in HIV-1 isolates from Moroccan patients failing ART. Although not surprising, the data plead for longitudinal surveys of the dynamics of emergence of DRMs (with a focus on multidrug resistance) in treated patients and circulation of resistant HIV-1 strains in this country.
Introduction
O
In Morocco, antiretroviral drugs (ARVs) were introduced in 1998 under combinations of three drugs (highly active antiretroviral therapy, HAART). Available ARVs are nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors (PIs). First-line HAART consists of two NRTIs in combination with one NNRTI or one unboosted PI, more recently with boosted PI. Treatment initiation is recommended for patients with CD4+ T cell counts <300 cells/μl, acute or symptomatic infection, or pregnancy. 4
We have reported previously a relatively low prevalence of drug resistance mutations (DRMs) in naive patients of Morocco. 5 However, there are no data so far on the molecular characterization (including DRMs) of HIV-1 isolates from patients exhibiting ART failure in Morocco. We report here HIV-1 DRMs in Moroccan patients failing HAART together with some additional data on the subtypes and CRFs circulating in the country.
Materials and Methods
The patients included in this study were HIV-1-infected patients followed-up at the Dermatology Department at Mohammed V Military Teaching Hospital in Rabat.
Inclusion criteria were as follows: all patients with HIV-1 infection who began ART between 2005 and 2010. ART failure was defined either as failure to achieve virological suppression or as detection of at least two plasma viral loads above 500 copies/ml after virological suppression. Demographic characteristics, treatment information, and measurements of viral load and CD4+ T cell counts were collected for all the patients.
The plasma samples were analyzed for sequencing provided they had a volume of at least 1 ml with a viral load threshold of 40 copies/ml (Cobas TaqMan HIV-1 Test, version 1.0, Roche Diagnostics Systems). RNA extraction was carried out using High Pure Viral RNA Kit (Roche Diagnostics Systems). The viral RNA was used for reverse transcription polymerase chain reaction (RT-PCR) followed by a nested PCR of reverse transcriptase (RT) and protease (Prot) genes, using two sets of primers in a GeneAmp PCR System 9700 (Applied Biosystems, Foster City, CA) thermal cycler. The outer and inner primers used are as previously described. 5 The obtained fragments were sequenced on both strands using the CEQ DTCS Quick Start kit on an automated sequencer Beckman Coulter GenomeLab GeXP DNA Analyzer System. Phylogenetic trees with bootscanning methods were inferred using the neighbor-joining method from matrix distances calculated after gapstripping of alignments, with a Kimura two-parameter algorithm. The DRMs were defined according to ANRS algorithm updated in 2010. 6 GenBank accession numbers for the sequences reported in this study are JN185274 to JN185318 and JN185229 to JN185273 for RT and prot sequences, respectively.
Results
Among 124 patients recruited and starting ART between 2005 and 2010, 45 patients (36%) were at ART failure: 8 patients (7%) failed before 1 year, 6 (5%) between 1 and 2 years, 7 (6%) between 2 and 3 years, and 23 (18%) after 3 years of treatment. The characteristics of the patients included are shown in Table 1. More than 93% of patients were males, 89% reported heterosexual contamination, and 71% of patients were already diagnosed with AIDS. The mean duration of previous ART was 25 months. The mean time between the virological failure and the date of sampling for resistance genotypic analysis was 2 months.
ART, antiretroviral treatment.
All patients were treated by two NRTIs; 33 received unboosted PIs and 12 received NNRTIs, three of them having received unboosted PIs and one a boosted PI as subsequent therapy.
The phylogenetic tree showed 74% subtype B, 11% subtype A, 9% CRF02_AG, 4% subtype G, and 2% subtype C (Fig. 1).

Subtypes in Moroccan patients failing ARV treatment.
Among the 45 patients, according to the ANRS algorithm, DRMs were observed for 24 patients (53%), resistance to NRTIs was detected in 22 patients (48%), resistance to NNRTIs in 6 patients (13%), and resistance to PIs in 10 patients (22%). The different mutation patterns of resistance to the three drug classes are reported in Table 2.
NRTIs, nucleoside reverse transcriptase inhibitors; NNRTIs, nonnucleoside reverse transcriptase inhibitors; PIs, protease inhibitors.
For NRTIs, the most frequent mutation detected was M184V observed in 20 patients (44%), M41L observed in 3 patients (7%), T215Y and M184I in 2 patients (4%), and D67N, K70R T215I, T215D, and L210W in 1 patient (2%) out of 45 NRTIs-exposed patients. The K103N, K101E, E138K, and P225H mutations, associated with NNRTIs resistance, were detected, respectively, in 4 (33%), 1 (8%), 1 (8%), and 1 (8%) of 12 NNRTIs-exposed patients. For PIs, the major mutations were V82A detected in 6 isolates (16%), M46I in 4 (11%), M46L, I54V, and L90M in 2 (5%), and V32I, I47V, I54A, L76V, and N88S in 1 patient (3%) out of 37 PI-exposed patients. Resistance to both NRTIs and NNRTIs was observed in 3 patients (13%), to NRTIs and PIs in 9 patients (38%), and the three-class resistance was found in 1 patient (4%).
The proportion of patients with DRMs to different classes according to duration of exposure (years) is shown in Fig. 2; 7% to NRTIs for less than 1 year (3 of 45), 7% between 1 and 2 years (3 of 45), 11% from 2 to 3 years (5 of 45), and 24% after 3 years (11 of 45). The proportions of patients with resistance mutations to NNRTIs by year of exposure were 17 % for less than 1 year (2 of 12), 8% 1–2 years (1 of 12), 8% 2–3 years (1 of 12), and 17% more than 3 years (2 of 12). The proportions of patients bearing virus with mutations to PIs by year of exposure were 3% for less than 1 year (1 of 37), 5% 1–2 years (2 of 37), 5% 2–3 years (2 of 37), and 14% more than 3 years (5 of 37).
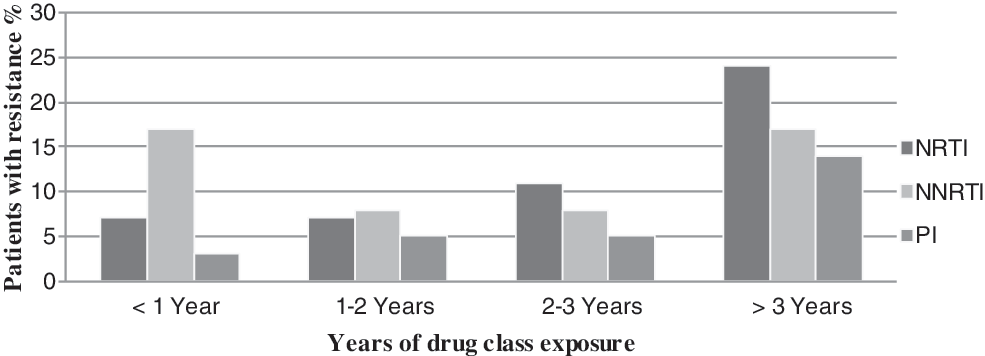
Prevalence of mutations of resistance to antiretrovirals (ARVs) (ANRS 2010 consensus) among patients failing treatment by year of exposure to drugs of the same class.
Among the 12 patients exhibiting treatment failure and infected with non-B strains, DRMs were observed in 6 patients (50%), resistance to NRTIs was detected in 2 patients (33%) with subtype A1 and CRF02_AG, and resistance to both NRTIs and PIs was observed in 3 patients (50%) with subtypes G, A1, and C. The three-class resistance was found in 1 patient (16%) with subtype G.
There was a high prevalence of minor resistance mutations in PR in non-B subtypes at positions M36I (92%), H69K (92%), and L89M (92%), while in the B subtype they were 6%, 3%, and 3%, respectively. Other minor resistance mutations L10I/F, K20R, L33I, D60E, L63P, and A71V were found in B and non-B subtypes.
Discussion
These results confirm our previous publication detailing the predominance of subtype B and the increasing prevalence of HIV-1 non-B subtypes (A, CRF02-AG, G, and C) in Morocco. 5 which can be mainly associated with the increasing immigration of Sub-Saharan Africans to European countries via Morocco. 7
This study provides the first estimation of the prevalence of DRMs in patients failing ARV therapy in Morocco. Our study showed that 53% of the sequences were exhibiting at least one DRM. Mutations conferring resistance to drugs of two classes were present in viruses from 27% of the patients tested while triple-class resistance was relatively uncommon (2%). These findings contrast with data from patients with treatment failure in South Africa, Uganda, Brazil, France, and Switzerland, which noted the presence of at least one DRM in 71% to 83% of the sequences, “dual resistance” ranging between 48% and 58%, and “triple resistance” between 13% and 20%. 8 –11 The prevalences of resistance, in our study, may be underestimated, because resistance mutations generally disappear from the plasma once drug treatment is interrupted and the genotypic assays used in this study were performed on plasma and thus potentially underestimate resistance. 12,13
The absence of DRMs was observed in 47% of patients failing ARV therapy in our work, whereas other international studies have revealed lower prevalences (ranging from 14% to 22%) of wild-type viruses 14 –18 ; that may be linked to insufficient adherence, 1,19 These findings show the need to better understand and to reduce adherence barriers in healthcare settings in Morocco, although an educational program to improve the management of HIV patients has been introduced in some departments of infectious diseases in the country since 2000. 20 In our study, assessment of adherence was not systematic across trials; therefore, we were unable to analyze its impact on virological failure and resistance rates.
All patients were exposed to NRTIs, thus explaining the high number of NRTI-related mutations (48%). About 26% of patients were exposed to NNRTIs and a majority of them presented NNRTI-related mutations (50%). The PI used by 80% of patients was unboosted indinavir, representing the pattern of drug usage when these patients started therapy and PI-related mutations have been observed in 27% of these patients. Only one patient was exposed to boosted lopinavir available since 2008 in Morocco. Boosted PIs can be more appropriate for use in first-line regimens in our country; these drugs produce greater increases in the CD4 cell count than do NNRTIs 1 and this could be important for Moroccan patients who initiate ARV with very low CD4 cell counts. Therefore, the risk of developing resistance is higher during NNRTI treatment than during boosted PIs. 21,22
The mutation M184V was the predominant mutation in this sample and its prevalence (70%) was comparable with that described for HIV patients failing HAART in other settings. 23 –25 This can likely be attributed to the wide use of 3TC in Morocco. The M184I was observed in two patients infected with a subtype B who had recently initiated therapy with 3TC.
RT mutations associated with high-level NNRTI resistance were detected in 50% of them, with major mutation K103N seen in 67%; this is not surprising given the low genetic barrier of resistance to these drugs. Most of the other studies similarly reported high prevalences of these mutations. 14,26,27
Patients starting HAART with a regimen including PI presented PI mutations in 50% of them, which can likely be attributed to the wide use of indinavir in those patients. The PI-related mutations were comparable to many other international series. 12,14 –16 The most prevalent mutations were at codons 46 (60%) and 82 (60%), followed by codons 54 (30%), 90 (20%), 32 (10%), 88 (10%), and 76 (10%). These prevalences were different from those reported in other series where M46L, V82A, and L90M occurred, respectively, in 21–25%, in 19–23%, and in 26–37% of patients. 12,24,26
We found that the prevalence of mutations related to NRTIs and PIs increased yearly with exposure to drugs of the same class. For NNRTIs a high level of mutation was observed within 1 year of treatment failure. Those results are in agreement with previous data. 28 The analysis of the frequency of DRMs by subtype revealed the global frequency of viral resistance was slightly smaller in patients infected by non-B subtypes; 50% had a resistant virus (6/12, 2 A1, 2 G, 1 C, and 1CRF02_AG) compared to 54% (18/33) for patients infected with a B strain. Mutations conferring resistance to both NRTIs and PIs were more frequently present in non-B subtype (50%) than in B strains (33%), while triple-class resistance was observed in subtype G. Interestingly, the distribution of minor resistance mutations in protease at positions 36, 69, and 89 was observed more frequently in non-B subtype (92%); the reported prevalence is similar to the prevalence reported in other studies, 29,30
This is the first study of HIV-1 resistance mutations in patients failing ARV therapy in Morocco; it will be important to collect more extensive data on resistance mutations in HIV-1 isolates from patients experiencing virological failure while receiving ART, together with surveys of DRMs in naive patients.
Conclusions
We showed a high frequency of resistance mutations to antiretroviral drugs in patients with virologic failure on ART in Morocco. Our data support the need for continued surveillance of resistance patterns to help guide therapeutic approaches, to limit transmission of these variants, and to guide the introduction of new drugs in a specific population in Morocco.
Footnotes
Acknowledgments
This study has been granted by CNRS UMR 5234; Hicham El Annaz has been trained in the virus laboratory of Bordeaux with the support of Mohammed V University at Souissi.
Author Disclosure Statement
No competing financial interests exist.