
Abstract
Recent reports have suggested an increased risk of acute hepatitis C (AHC) infection in homosexual HIV-infected men and that early treatment with interferon-alfa, alone or associated with ribavirin, significantly reduces the risk of chronic evolution. A retrospective analysis of 38 HIV-infected patients who were consecutively diagnosed as developing AHC, defined by both seroconversion of anti-hepatitis C virus (HCV) antibodies and detection of serum HCV-RNA in those with previous negative results.
Thirty-six patients were men with history of unprotected sexual intercourse with men and two were women with sexual and nosocomial risk factors. AHC infection was asymptomatic in 26 patients; asthenia and jaundice were the most frequent symptoms. HCV genotype 1 was present in 19 patients and genotype 4 in 14 patients. Thirty-five patients received early antiviral treatment with pegylated interferon-alfa associated with ribavirin; 15 of the 32 patients who completed the follow-up (47%) achieved a sustained virological response, as defined by undetectable HCV-RNA 6 months after the end of therapy. There is a risk of sexual transmission of HCV in HIV-infected men who have sex with men. In our experience, early treatment of AHC with pegylated interferon-alfa plus ribavirin in HIV patients achieves poor results.
Introduction
H
In the past 6 years, a growing number of cases of acute hepatitis C (AHC) have been reported in large urban centers in Europe, 2 –4 the United States, 5 –7 and Australia. 8 Moreover, longitudinal cohort studies have confirmed an increase in the incidence of HCV among HIV-positive homosexual patients. 9,10 Recently, a phylogenetic analysis of transmitted HCV strains showed clustering consistent with transmission inside a social and sexual network of HIV-positive men who have sex with men (MSM) that extends nationally and internationally. 10
The increased incidence of AHC in HIV-positive MSM has been attributed to several factors: the tendency toward a higher HCV viral load in HIV patients' blood and semen, 11 –13 certain sexual practices in which there is an increased risk of mucosal damage, the presence of ulcerative sexual transmitted diseases (STDs) such as syphilis or lymphogranuloma venereum, 14 a greater number of sexual partners, 15 and the use of recreational drugs such as gamma-hydroxylbutyrate (GHB). 16 Nevertheless, acute cases of HCV have been described among MSM who deny all the risk factors mentioned above.
This article describes our experience with AHC in HIV patients, and presents the first report of a Spanish outbreak of AHC in HIV-positive MSM.
Materials and Methods
Patients
All patients who were consecutively diagnosed with acute HCV infection between June 2003 and June 2010 at our HIV clinical unit were included in this retrospective study.
These patients underwent routine follow-up of their HIV infection every 3 months, including clinical and biochemical evaluation and the liver function tests aspartate aminotransferase (AST) and alanine aminotransferase (ALT). Anti-HCV antibody testing was performed at the time of diagnosis of HIV infection and then if patients reported risk factors for HCV infection.
All patients who had an unexplained increase in liver enzyme activities (more than three times the upper normal limit) during routine monitoring of HIV infection and all patients with clinical signs of acute hepatitis (arthralgia, jaundice, severe fatigue, urine and stool discoloration) were screened for HCV infection.
AHC infection was diagnosed on the basis of documented HCV-RNA positivity by transcription-mediated assay [Versant HCV-RNA Qualitative Assay (TMA), detection limit 5 IU/ml, Siemens Healthcare Diagnostics Inc., Tarrytown, NY], HCV-RNA quantification [Versant HCV RNA 3.0 Assay (bDNA), detection limit 615 IU/ml, Siemens Healthcare Diagnostics Inc., Tarrytown, NY], and anti-HCV seroconversion during a period shorter than 6 months (ELISA 3rd generation: HCV Advia Centaur, Siemens Healthcare Diagnostics Inc. Tarrytown, NY). Data on the sexual behavior and other classical risk factors for HCV infection were recorded.
Virological assessments
The HCV genotype was determined by RT-PCR/RFLP. 17 To estimate the date of HCV infection and to confirm AHC, stored plasma samples obtained less than 12 months before diagnosis were screened for anti-HCV antibodies and HCV-RNA in several patients.
Follow-up
Patients were monitored every 2 weeks after diagnosis of HCV infection to measure the fall in HCV-RNA. Those who did not spontaneously clear HCV-RNA 16–20 weeks after the estimated date of HCV infection were offered a 24-week course of pegylated interferon (PegIFN) alfa-2b (1.5 μg/kg/week) or PegINF alfa-2a (180 μg/week) plus ribavirin (RBV) (800–1200 mg/day adjusted for body weight). Sustained virological response (SVR) was determined 24 weeks after the end of treatment.
Ongoing antiretroviral therapy was maintained. The patients were seen every 2 weeks during the first month and every 4 weeks until the end of the treatment period, and then every 3 months in the follow-up period.
Statistical analysis
A descriptive analysis of the baseline variables was conducted, including measures of central tendency and dispersion. Univariate logistic regression was used to confirm the importance of previously identified prognostic factors of SVR. Factors that showed associations in the univariate analysis (p<0.1) were considered as candidates for inclusion in the multivariate logistic regression. A stepwise procedure was then applied to the factors that were significant in the univariate analyses to assess their independence. All reported p-values are two-sided. Statistical significance was defined as a p-value of <0.05. Data were analyzed by STATA (StataCorp. 2005. Stata Statistical Software: Release 9.2. College Station, TX: Stata Corporation).
Results
Baseline characteristics of patients
Patient characteristics at baseline are described in Table 1. The study enrolled 38 HIV-infected patients who were diagnosed consecutively with AHC infection between June 2003 and June 2010 (see Fig. 1). From 2003 to 2006 only three patients were diagnosed, but in recent years a clear outbreak of AHC was detected in our environment (see Fig. 2). Thirty-six patients were men with sexual risk practices (i.e., unprotected sex with other men). HIV infection of the two female patients included in our series was attributed to a possible nosocomial transmission and heterosexual contact.
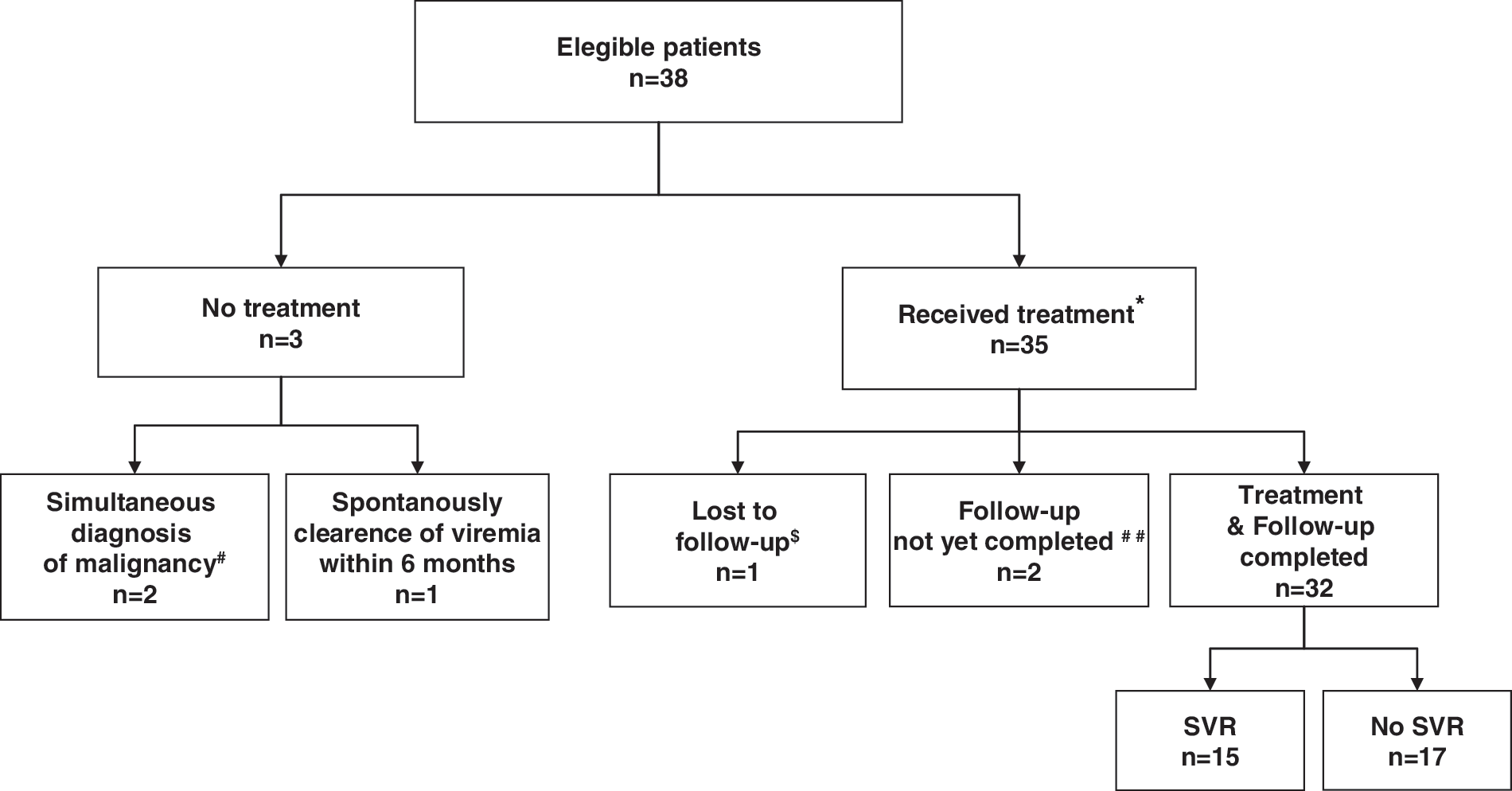
Flow-Chart: patients enrolled in the study and outcome.
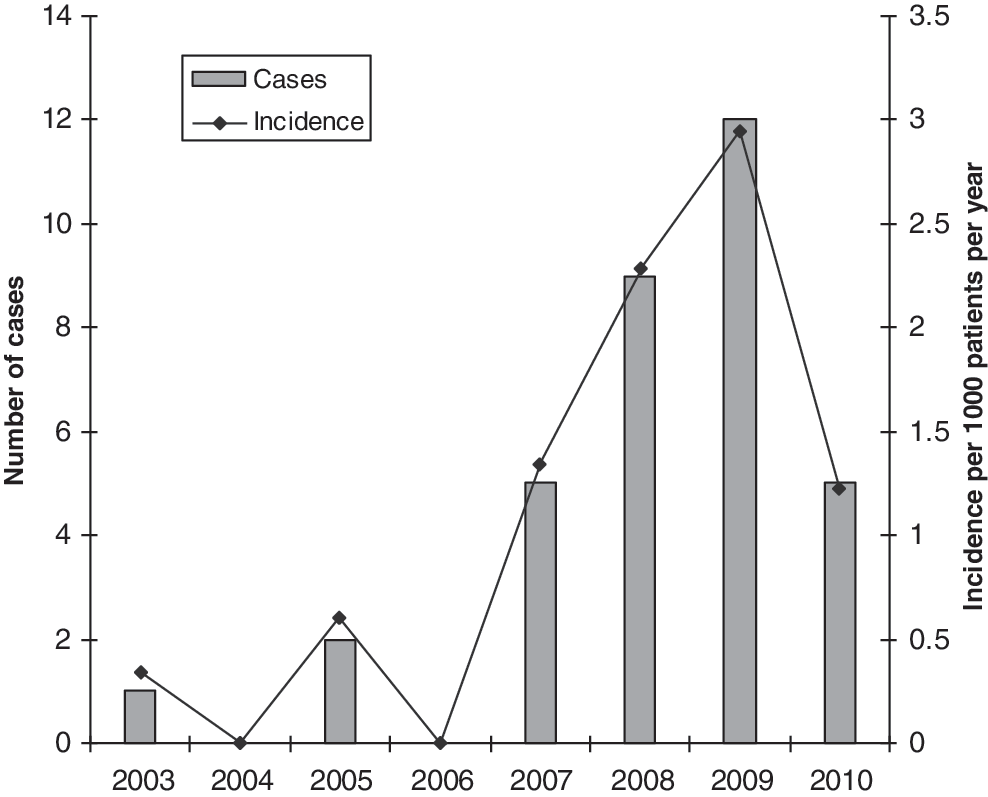
Yearly distribution of incidence (number of cases per 1000 active HIV patients per year) and number of cases.
n (percentage).
HCV, hepatitis C virus; HIV, human immunodeficiency virus; AST, aspartate aminotransferase; ALT, alanine aminotransferase; STD, sexual transmitted disease; PegINF, pegylated interferon.
Median (IQR) age was 40 (32–45) years. Nine of the patients came from South America, two from North America, and the rest were European. The median duration of known HIV seropositivity before the diagnosis of acute viral HCV infection was 5.8 (1.9–9.7) years. In four cases, AHC and HIV diagnoses were concomitant: in these cases, there was no risk factor within the previous 6 months other than unprotected sexual intercourse. Thirty patients were taking combined antiretroviral therapy before AHC diagnosis. All of them except one had an undetectable HIV viral load in blood and a CD4 cell count >200 cells/μl (median 480 cells/μl). Eight patients were category C in the CDC classification for HIV infection.
Most patients included were immunized for hepatitis A and B (79% and 84%, respectively). Twenty-six percent of patients had a history of STD: syphilis in five patients, urethritis in three patients, concomitant syphilis and urethritis in one patient, and lymphogranuloma venereum in one patient.
Characteristics of AHC infection
Twelve patients (32%) were tested for HCV infection because they had clinical symptoms: asthenia in six patients, fever in three patients, and jaundice or influenza-like symptoms also in three patients. The remaining 26 patients were asymptomatic, and acute hepatitis was suspected after detecting a rise in liver enzyme activity during routine follow-up of HIV infection.
The diagnosis of acute hepatitis was based on anti-HCV seroconversion and detection of HCV-RNA. In most patients, serial analytical controls were available for diagnosis of AHC infection. In only four cases was it necessary to test previously collected frozen sera; no HCV-RNA or HCV antibodies were detected in any of these tests. The median time between risk exposure and diagnosis of AHC infection was 3 (2–4) months. At diagnosis, the median plasma aspartate aminotransferase value was 240 (187–389) IU/liter and alanine aminotransferase was 517.5 (404–777) IU/liter (normal values are <40 IU/liter). HCV genotype was identified in 36 patients: type 1 in 19 patients (50%), type 3 in two patients (5.2%), type 4 in 14 patients (36.8%), and mixed type 1 and 4 in one patient. The median plasma HCV-RNA was 1,441,725 (169,000–2,856,000) IU/ml.
Outcome
HCV infection resolved spontaneously in only one patient, 3 weeks after diagnosis.
Anti-HCV therapy was started within 24 weeks of the onset of hepatitis in 35 patients. Two patients had a malignancy (rectal adenocarcinoma) requiring priority surgical treatment and subsequent chemotherapy that contraindicated antiviral treatment for HCV (see Fig. 1).
Antiviral therapy: efficacy
The median time between diagnosis of acute HCV infection and initiation of specific treatment was 3 (2–3) months. All treated patients received PegINF alfa-2b (23 patients) or PegINF alfa-2a (12 patients) associated with weight-adjusted RBV dose.
The results for the first 32 patients to complete 24 weeks of posttreatment follow-up are reported here (Table 2). Treatment is ongoing in the remaining two patients and one patient was lost to follow-up. In our cohort, only 15 patients (47%) presented an SVR to treatment.
Fifteen patients were nonresponders (i.e., HCV-RNA was detected during and after treatment) while two patients tested HCV-RNA negative at the end of therapy and 3 months after HCV therapy discontinuation, but the HCV viral load then bounced between months 3 and 6 of follow-up. In these two patients, an additional course of pegylated interferon in combination with RBV was initiated. Therapy is currently in progress, and the final results of viral response are not available. It is difficult to determine whether these two cases were late relapses or possible reinfections. The study of viral genotype demonstrated the maintenance of HCV genotype 1a in the first patient and the same double viral infection with genotypes 1 and 4 in the second.
Plasma HCV-RNA at week 4 was undetectable (below the detection limit of 615 IU/ml, copies) in 12 patients of the 32 who completed the schedule of treatment and follow-up. Eleven of these patients with rapid virological response (RVR) achieved SVR. The patient that did not achieve SVR had a very low HCV-RNA titer (but detectable at weeks 4 and 12). The positive predictive value (PPV) of SVR in the patients who achieved RVR was 91.6%.
Twenty patients showed early virological response (EVR), defined as a ≥2 log drop of HCV-RNA from baseline at week 12. Among these patients, five did not achieve SVR (PPV 75%). Four of these patients had very low HCV-RNA titers (<615 IU/ml) and one patient had undetectable qualitative determination of HCV-RNA at week 12. Focusing on the subgroup of patients who achieved complete EVR (cEVR defined as RNA undetectable by a qualitative technique at week 12), all except one achieved SVR (PPV 93.5%). None of the patients without cEVR achieved SVR; thus, the negative predictive value (NPV) of not achieving cEVR was 100%.
To examine the influence of potentially important prognostic factors for SVR, we performed a univariate analysis (see Table 3). Among all the variables examined only the RVR values (p<0.0001) were significantly associated with a higher likelihood of SVR. Multivariate analyses could not be performed because this was the only variable that met the inclusion criteria.
HCV, hepatitis C virus; HIV, human immunodeficiency virus; AST, aspartate aminotransferase; ALT, alanine aminotransferase; STD, sexual transmitted disease; PegINF, pegylated interferon; RBV, rivabirin.
Antiviral therapy: adverse events
One patient presented a serious hemolytic anemia that led to hospitalization and withdrawal of RBV. The patient completed 24 weeks of PegINF without achieving viral response.
Two other patients needed a transient RBV dose reduction for a few weeks due to anemia and four more needed a PegINF dose reduction for 2–3 weeks due to neutropenia. The rest of the patients tolerated the treatment without dose modification. No cellular growth factors were required.
Seven patients discontinued treatment before 24 weeks because of failure to reduce HCV-RNA levels at week 12 of therapy.
Twelve patients presented depressive symptoms during therapy, and therapy with citalopram was prescribed between weeks 4 and 24 of treatment.
As expected, the CD4+ cell count fell slightly during AHC therapy. No significant changes in HIV viral load were observed during follow-up.
Discussion
In common with reports from other cities in Europe, North America, and Australia, we also witnessed an outbreak of acute hepatitis C among HIV-positive homosexual patients in Spain. Despite the high prevalence of chronic HCV in Mediterranean countries, no outbreak of AHC in the HIV community had been previously reported in this area. The present study is the first report of an outbreak of this kind.
Excluding our two female patients, all patients with acute hepatitis C presented sexual risk factors for infection. The incidence curve of AHC in our center, which featured a clear peak in the years 2008 and 2009, is difficult to explain. Not all patients presented with the same HCV genotype; they came from different backgrounds and not all patients had used recreational drugs or had an STD. What is more, the literature data clearly reflect a change in the virulence of hepatitis C in recent years. 1
The distribution of HCV genotypes in our series, similar to that reported in other studies, 2 –4,18 –20 showed a higher expected frequency of genotype 4 in our geographic area. This finding may be attributed to the existence of an international sexual network among HIV-positive MSM.
Jaundice is a characteristic clinical sign in the HCV-monoinfected population, but it was present in only a small percentage of our HIV-positive patients. This low prevalence has also been described in other reports. 19 In most cases the diagnosis was made during the routine follow-up control of HIV patients and it was suspected when transaminases were found to be elevated.
HCV has emerged in the recent years as an STD in HIV-positive MSM patients, 18 –21 while its prevalence as an acute infection in the HIV-negative MSM population remains low. 22,23 AHC may appear as a coinfection with other agents such as syphilis, gonorrhea, Chlamydia, and even HIV. In our cohort, nearly one-third of patients presented coinfection. Therefore, screening for HCV should be performed in any patient examined for an STD.
The spontaneous viral clearance rate in the present series was very low. The studies 4,19,20,24 –27 reported in the literature show a wide range of spontaneous resolution rates of AHC, between 4% and 27%. It is known that HIV coinfection, the lack of symptoms, and male sex are factors that are associated with an increased risk of progression to chronicity. 28,29 It is possible that some patients in our hospital may have been infected and may have spontaneously cleared viremia, but they were not detected because they presented few symptoms and their analytical controls were uninformative.
The data on the effectiveness of anti-HCV therapy in HIV patients with AHC are limited and are based on results of small studies. Monotherapy with interferon has shown a poor rate of SVR (0–10%). 2,4,30 Vogel et al. 27 found no advantage of adding ribavirin to PegIFN, but other authors 8,24,31 obtained higher rates of SVR with combination therapy. The optimal duration of treatment is not well established; the NEAT consensus conference, based on the results of different studies, proposes a 24-week course of therapy and advocates reserving a longer duration of treatment for patients with mild initial response (without RVR but with EVR). 32
In our hospital, we used combined therapy with PegINF plus RBV for 24 weeks. We obtained a moderate rate of SVR, nearly 50%, similar to that reported in a small cohort study of HIV patients in the United States 19 but lower than rates obtained by other authors. 8,2,25,31 The risk of reinfection of AHC in HIV-positive MSM cured of a previous HCV infection has been well documented, 33,34 and we observed two cases in our series. These data reinforce the need to implement health promotion campaigns in this population.
Due to the small number of patients included in the studies published, the identification of predictors of response is very difficult. Certain factors have been associated with SVR: elevated baseline ALT and CD4, 25 symptomatic AHC, 35 and rapid HCV negativity. 8,24,31 In our study, no baseline variables were related to SVR: only RVR was positively correlated with SVR in the analyses.
Viral kinetics seems to be very important for identifying a favorable course in HIV patients with AHC who show a good response. If HCV is negative at week 4, the possibility of clearing the virus is very high; in our cohort, the PPV was 93.5%, similar to values reported in other studies. 8,31,35,36 Conversely, lack of EVR at week 12 may be an important predictor of nonresponse to therapy and can be used as a reliable marker for discontinuing therapy.
In this study, as in previous reports, 8,25 the length of time between diagnosis of acute hepatitis and treatment initiation did not influence treatment response. HCV therapy was not more effective when initiated 12 weeks after diagnosis of AHC infection than when started later (between 12 and 24 weeks).
There are very interesting data in the literature on the relationship between certain genetic polymorphisms and the spontaneous clearance of HCV and the SVR to HCV therapy. Recently, two studies reported improved SVR with IL28B C/C alleles in HIV-coinfected patients with chronic HCV. 37,38 However, the same authors did not find this relation in AHC. 38 Unfortunately we cannot provide information about this possible relationship because we do not have the results for the IL28B polymorphism in our patients.
In conclusion, treatment of AHC infection in HIV-coinfected patients with PegIFN plus RBV for 24 weeks yielded a moderate rate of SVR in our cohort of 32 patients. Prevention efforts are required in order to reduce the number of new infections. Regular screening in this population will help to diagnose AHC infections. Finally, it seems essential to evaluate new treatment strategies in HIV-coinfected patients to improve the SVR and to avoid progression to chronicity.
Footnotes
Acknowledgment
Dr. M. Laguno is funded by a grant from the Spanish Ministry of Health (FIS 2007).
Author Disclosure Statement
No competing financial interests exist.