
Abstract
Cryptococcal meningitis has emerged as a leading cause of infectious morbidity and mortality in patients with AIDS. A retrospective analysis of records of HIV-infected individuals registered in the Immunodeficiency Clinic of a tertiary care hospital and research institute was carried out. Records of 6900 HIV-infected individuals who were enrolled in the clinic between January 2002 and March 2011 were analyzed. Records of 6900 HIV-infected individuals were screened. Ninety-one were diagnosed with cryptococcal meningitis (1.32%). In 68 individuals cryptococcal meningitis was the presenting illness. Nine patients developed meningitis within 6 months of starting antiretroviral treatment (ART). Six patients were receiving ART for more than 6 months at the time of diagnosis. The remaining eight patients were not on ART at the time of development of meningitis. The mean baseline CD4 count of patients was 77.7±61 (range, 4–259, n=91) cells/mm3. Seventy-four patients had a CD4 value of less than 100 at the time of diagnosis of cryptococcal meningitis. Eleven of these ninety-one patients had a relapse of cryptococcal meningitis while receiving a maintenance dose of fluconazole. During follow-up 37 died, two were lost to follow-up, while 52 patients were on regular ART. Mortality due to cryptococcal meningitis amounted to 0.54% (37/6900). There was no correlation between survival and duration of ART at the time of cryptomeningitis (Pearsons χ2=0.241, p=0.884). There was a significant difference in the CD4 counts of the HIV-infected individuals who died with cryptomeningitis and those who survived (Pearson's χ2=9.1, df=4, p=0.05). The frequency of cryptococcal meningitis was 1.32%. Cryptococcal meningitis leads to high mortality in HIV patients. Management of cryptococcal infection remains a key facet of AIDS care in India.
Introduction
C
Treatment of a patient with cryptococcal infection is a challenge for both the physician and the patient, but rewarding, as many would recover with timely and adequate antifungal therapy. The spectrum of infection varies from a harmless colonization of the airways to potentially fatal meningitis and disseminated disease, the major determining factor being the immune status of the patient. Defects in cell-mediated immunity predispose to more serious infection. Reports had shown the incidence of cryptococcal infection in AIDS patients was 6–10% in the United States and 30% in Africa. 3 Mortality from developed countries is in the range of 10–30% while in developing countries the mortality rate is substantial, around 13–40%. 4,5 However, the wider availability of fungicidal drugs and the expansion of antiretroviral programs now raise the prospect of transforming the prognosis of these patients and narrowing the differences in these statistical figures. A sizable proportion of the cryptococcal disease burden is thought to be due to symptomatic relapse of previously treated infection. Without secondary prophylaxis at least 50–60% of patients will have disease relapse. 6 Secondary fluconazole prophylaxis is highly effective when used properly, increasing recurrence-free survival by over 13-fold at 6 months. 7 We have conducted this study in our institution to determine the frequency of cryptococcal infection among AIDS patients in the HAART era.
Materials and Methods
This study was conducted in the center of excellence, Department of Internal Medicine, Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh, India. The study period extended from January 2002 to March 2011. A retrospective analysis of records of HIV-infected individuals registered in the Immunodeficiency Clinic was done. Records were analyzed to collect information on all HIV-positive patients ever diagnosed with cryptococcal meningitis. Cryptococcal meningitis was defined as clinical features of meningitis/meningoencephalitis along with positive cerebrospinal fluid (CSF) cryptococcal antigen test or positive CSF India ink preparation or isolation of Cryptococcus neoformans in the CSF culture.
Data were collected on demographic profile, risk factors for acquisition of HIV, CSF picture, concomitant infections, complications, and hospital outcome. All HIV patients presenting with clinical features of meningitis/meningoencephalitis were subjected to CSF examination. Cryptococcal antigen test, India ink, and culture for Cryptococcus were routinely done for all CSF samples. All patients diagnosed with cryptococcal meningitis received amphotericin-B (0.7 mg/kg/day) for 2 weeks. Flucytosine was not given as it was not available. Fluconazole (400 mg/day) was given for the next 8 weeks. Subsequently, secondary prophylaxis with fluconazole (200 mg/day) was continued until the CD4 count increased to more than 200 cells/mm3 on two occasions at least 6 months apart. 8 Baseline CD4 cell count, CD4 count at the time of diagnosis of cryptococcal meningitis, and improvement in the CD4 cell count at 6 months of initiation of antiretrovirals and antifungals were recorded.
Follow-up data of these patients after discharge were recorded. During follow-up any recurrence of cryptococcal meningitis, possible reasons of recurrence, type of treatment received, complications developed, and outcome were recorded. Statistical analysis was performed using SPSS-16 software. Correlation of survival with age, sex, baseline CD4 cell counts, and duration of antiretroviral therapy (ART) received was calculated using Pearson's correlation. A p value≤0.05 was considered as statistically significant.
Results
Records of 6900 HIV-infected individuals who were enrolled in the Immunodeficiency Clinic were analyzed. Ninety-one of these HIV-infected individuals had been diagnosed with cryptococcal meningitis (1.32%). These included 73 males and 18 females. The mean age of these patients was 35.3±8.1 (22–62) years. The commonest mode of transmission was multiple heterosexual unprotected sexual contacts, seen in 85 patients. Two patients each had history of unsafe blood transfusion and intravenous drug abuse. The majority patients were drivers by profession (n=35) and a majority came from a rural background (n=73, 80%). A detailed demographic profile is shown in Table 1. Seventy-five (82%) of the patients at the time of presentation in the Immunodeficiency Clinic were in WHO Clinical Category IV. 9 Of all 91 patients diagnosed with cryptococcal meningitis, this was the presenting illness in 68 patients, which led to a diagnosis of HIV. Nine patients developed meningitis within 6 months of starting ART. Six patients were receiving ART for more than 6 months at the time of development of cryptococcal meningitis. In two of these patients there was failure of first line therapy and they had to be started on second line ART and four patients had poor compliance on ART. These 15 patients were receiving antiretrovirals for a mean duration of 19.9±30.5 (1 to 120) months prior to the diagnosis of cryptococcal meningitis. The remaining eight patients were not on antiretroviral treatment at the time of development of meningitis. The most common presentation was in the form of headache (n=82), fever (n=71), altered mental status (n=23), and visual disturbances (n=12). Their mean baseline CD4 cell count was 77.7±61 (4–259) cells/mm3. The duration of HIV seropositivity at the time of diagnosis of cryptococcal meningitis ranged from 0 to 10 years with a mean duration of 2.6±2.2 years (n=91). The mean CD4 cell count at the time of diagnosis of cryptococcal meningitis was 79.3±54.9 (4–260, n=91) cells/mm3.
IVDU, intravenous blood use.
As is evident from Fig. 1A, 74 patients had a CD4 value of less than 100 at the time of diagnosis of cryptococcal meningitis, with only 17 patients having a value of more than 100, and with four patients having a value of more than 200. Figure 1B shows the number of hospital admissions due to cryptococcal meningitis since 2002. The available neuroimaging (CT head/MRI) findings of 55 patients are represented in Table 2. All patients had hypoglycorrhachia (CSF sugar less than half of concomitant blood sugar), with an average CSF sugar of 45.4 mg/dl and an average concomitant blood sugar of 117.9 mg/dl. CSF protein of more than 40 mg/dl was seen in 56 patients (61.3%). Thirty patients had no cells in light microscopic examination of CSF. Lymphocytic predominance was seen in 33 patients and the rest of the 28 patients had a predominant polymorphonuclear response. India ink was positive in 54/91 (59.3%) patients. A cryptococcal antigen test in CSF was positive in 73/91 (80.2%) patients. Fifty-five (60%) patients had a CSF culture positive for Cryptococcus neoformans.

Table 3 shows other infective conditions concurrently seen with cryptococcal meningitis in our patients. Tuberculosis was the most common concomitant infection seen, with Pulmonary Kochs being the commonest form of tuberculosis (Table 4). This was followed by oral candidiasis. Six patients were diagnosed with disseminated cryptococcosis. The diagnosis was based on cryptococcoci seen lymph node biopsy in four patients, skin biopsy in one patient, bone marrow culture in one patient, and bronchoalveolar lavage (BAL) fluid in two patients. Twenty-six of the total patients who survived the episode developed one or the other complication of cryptococcal meningitis. Seizures were the commonest of these followed by cranial nerve palsies (Table 5). Seventy-two patients received ART. Thirty patients were receiving a combination of stavudine (d4T)+lamivudine (3TC) and nevirapine (NVP). Another 19 patients were receiving d4T+3TC+efavirenz (EFV). Zidovudine (AZT)+3TC+NVP combination was prescribed in 11 patients and 10 patients were receiving a combination of AZT+3TC+EFV. Two patients were receiving second line ART in the form of a combination of tenofovir, lamivudine, and lopinavir boosted with ritonavir. Seventeen patients did not receive ART. In one patient cryptococcal meningitis occurred after 5 years on regular ART and heralded clinical failure to first line therapy. The mean duration of the hospital stay after diagnosis of cryptococcal meningitis was 14 days. Sixty-five patients developed some adverse effects to amphotericin-B. The commonest side effect was hypokalemia seen in 59 patients. Acute febrile reaction occurred in 34 patients. An increase in urea and creatinine was seen in 23 patients. Eleven of these 91 patients had a relapse of cryptococcal meningitis while receiving a maintenance dose of fluconazole. Table 6 shows the detailed demographic profile, CD4 cell count, and probable reason for relapse of cryptococcal meningitis in these patients. At present, out of these 91 patients, 37 have died, 2 were lost to follow-up, while 52 patients are on regular ART. Mortality due to cryptococcus meningitis amounted to 0.54% (37/6900).
CMV, cytomegalovirus.
TB, tuberculosis; TBM, tubercular meningitis.
ART, antiretroviral therapy.
Predictors of survival
Age and sex had no correlation with survival (Kruskal–Wallis test, p value 0.624 and 0.354, respectively). There was no correlation between survival in relation to the occurrence of cryptomeningitis with respect to duration of ART (Pearsons χ2=0.241, p=0.884). No correlation was noted between survival and cryptococcal relapse (Pearson's χ2=0.698, p=0.403). There was no statistically significant difference in the mean age of HIV-infected individuals who died with cryptomeningitis and those surviving (Mann–Whitney U test, z=2.5, p=0.8). There was a significant difference in the absolute CD4 cell count of the HIV-infected individuals who died with cryptomeningitis and those surviving (Pearson's χ2=9.1, df=4, p=0.05). To compare the survival of 91 patients with different CD4s, data were divided into five groups. Group I had CD4 count<50 cells/μl (n=27, survived: 15, death:12), Group II had CD4 count between 50 and 100 cells/μl (n=47, survived: 22, death: 23, lost to follow-up: 2), Group III had CD4 count between 101 and 150 cells/μl (n=7, survived: 6, death: 1), Group IV had CD4 count between 151 and 200 cells/μl (n=6, survived: 5, death: 1), and Group V had CD4 count>201 cells/μl (n=4, survived: 4, death: 0). In all, 52 individuals have survived and 37 have died. There is a significant difference in survival of HIV patients with baseline CD4 <50 (n=27) when compared with a group of patients with CD4 >100 (n=17), log rank (Mantel-Cox), chi-square 6.2, p=0.01. Again a significant difference was noted in the survival in patients with CD4 count between 50 and 100 (n=47) and >100 (n=17), log rank (Mantel-Cox), chi-square 10.187, p=0.001) (Fig. 2). The estimated survival time is given in Table 7.
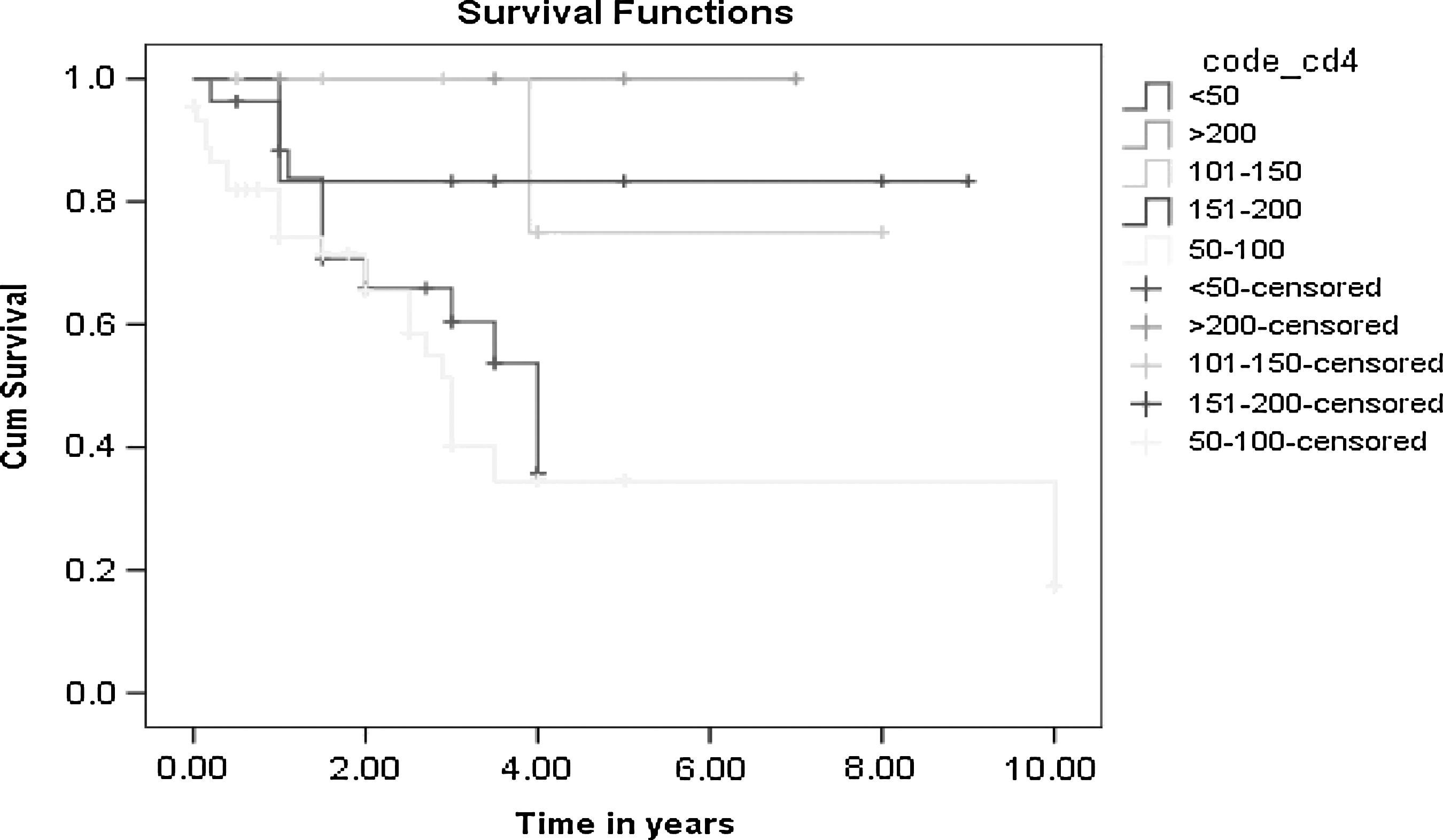
Cumulative survival in years for group of patients with CD4 count <50, 50–100, 101–150, 151–200, and >200.
Estimation is limited to the largest survival time if it is censored.
Discussion
Cryptococcosis is the most common lethal fungal infection in patients with AIDS. 2 Understanding the burden of cryptococcal disease is particularly important for public health officials to adequately plan and prioritize needed resources for disease prevention and control. To understand the public health attention to this infection, we reviewed available data and estimated the burden of cryptococcal meningitis among persons living with HIV in a hospital setting. Many of the incidence estimates used here were determined prior to the current effort to provide wide access to free antiretroviral treatment. However, as the number of persons needing antiretroviral drugs is likely to be stable or even increasing, due to the evolution of the HIV epidemic, expanding access to ART is not likely to impact the global burden of cryptococcal disease soon. In many of the developing countries in sub-Saharan Africa and South and Southeast Asia, the capacity to perform the complicated management of severe cryptococcal meningitis is limited. 10 An important step in reducing the impact of this infection undoubtedly is the marked expansion of ARV access therapy for HIV, as risk of cryptococcal disease is substantially reduced among persons receiving these treatments. 11 However, because the number of people with advanced immunosuppression from HIV and cryptococcal disease will continue to remain high despite expanded access to antiretroviral therapy, specific public health efforts are needed.
Prevention of disease is the ultimate public health goal in the approach to cryptococcal meningitis, though this may be difficult to achieve. Another strategy that warrants further investigation is screening for early cryptococcal disease with the serum cryptococcal antigen test. Nonmeningeal cryptococcal infection often precedes meningitis but is underrecognized or misdiagnosed. 12 –16 Early detection and treatment of asymptomatic or latent cryptococcal infection may allow fluconazole to be used as the first-line therapy, a much less expensive and highly available option. A focused effort to improve diagnostic capacity, expand treatment options, and identify effective measures for the prevention of cryptococcal disease is urgently needed.
The introduction of combined ART has markedly decreased the overall mortality for these advanced HIV-infected patients. 17 Treatment of cryptococcal meningitis in patients with AIDS with amphotericin B plus flucytosine is associated with a failure rate of 20–30%. In the absence of chronic suppressive therapy, 40–60% of patients develop recurrent disease. 3 After the onset of the HIV pandemic, cryptococcal meningitis has emerged as a frequently encountered cause of meningitis in these patients.
The prevalence of cryptococcal meningitis in our population was 1.32%. The estimated global burden of the disease is 0.04–12% per year. 18 Previous studies from East Asia have put this figure at 1.7 % per year. 18 There is considerable geographic variation in the prevalence of cryptococcal infection, the incidence being higher in Africa and Southeast Asia and successively lower in the United States and in Europe. The median age of 36 years (range, 22–62) is the same as reported in previous similar studies. 19 Our patients belonged to both rural and urban backgrounds and a predominance of patients from rural areas probably only reflects the fact that a major proportion of the population from our part of the world resides in rural areas. Historically, most of the reported cases of cryptococcal meningitis are males. This has been represented in earlier studies and this continues to be evident in our findings. In South Africa, where women represent more of the AIDS population, 61% of the cases of cryptococcal meningitis in HIV-infected patients are female. 20
Cryptococcosis has been seen more frequently in those without a previous diagnosis of HIV, and tends to develop when the CD4 count drops to 50 cells /mm3 or less. In our study, 24% of the patients had been diagnosed with HIV before they were determined to have cryptococcal meningitis. This may also represent an inherent selection bias as our institution is well associated with HIV care and offers the largest quantum of HIV-related admissions in this part of the country. The mean CD4 count of our patients was 79 cells/mm3.
Nine of our patients developed cryptococcal meningitis within 6 months of starting ART. The timing and clinical features of these patients with cryptococcal meningitis suggest that the events were due to an immunological response associated with ART and hence a reflection of immune reconstitution inflammatory syndrome (IRIS). IRIS is usually accompanied by an increase in CD4 cell count due to successful ART. Most cases of IRIS occur in patients with a low CD4 cell count at the time of ART initiation. 21 In noncryptococcal IRIS, most patients present in the first 8 weeks after the start of ART. 22 –24 However, there is little information regarding the timing of cryptococcal IRIS. Previous small studies have indicated that cryptococcal IRIS can occur from as little as <2 weeks to 22 months after initiation of ART. 21,25
The development of new or recurrent World Health Organization (WHO) stage 3 or 4 conditions after the first 6 months of ART is considered functional evidence of HIV disease progression, which occurred in six patients due to poor compliance or first line failure. Various studies reported that 8–50 % of HIV patients with cryptococcal infection who responded to ART developed cryptococcal IRIS. 21,26 Earlier a study from our center reported 40 cryptomeningitis patients in 3 years; of these four patients had cryptococcal IRIS. 27 Lortholarya et al. have demonstrated that independent risk factors for the occurrence of cryptococcal IRIS are HIV infection that was revealed by cryptococcosis, low CD4 cell count, fungemia at baseline, and initiation of antiretroviral treatment within 2 months of cryptococcosis. 26 IRIS presenting during the first 3 months of ART reflects an immune response against an active infection by opportunistic pathogens, whereas late IRIS may result from an immune response against the antigens of nonviable pathogens. 28 This may explain why secondary prophylaxis of cryptococcosis cannot prevent cryptococcal IRIS. During the first 3 years of ART, immune reconstitution cryptococcosis should be recognized in patients presenting with culture-negative cryptococcosis, and the occurrence of this syndrome should not indicate ART failure.
Our study demonstrates 40.6% (37/91) mortality due to cryptococcus meningitis. There was a significant difference in the survival of patients with a CD4 count <50 when compared with those who had CD4 100 cells/μl. A study from Thailand has demonstrated a substantial increase in survival time of HIV-infected patients with cryptococcal meningitis by initiating ART even in a resource-limited setting (no flucytosine, local combined antiretroviral drugs with NVP-based regimens). 29 In another study from Uganda, survival with cryptomeningitis was compared before and after the availability of HAART and it was found that even with the availability of HAART, the 6-month rate of survival after cryptomeningitis was only 41%. 30 The 1-year survival rate for cryptomeningitis in Uganda with HAART available remains 4-fold worse than that in France and ∼2-fold worse than that in Thailand. 31,32 Ongoing HIV care, with or without the use of potent antiretroviral agents, has been established as a deterrent to the development of cryptococcal disease. 11 In our study, the majority of deaths occurred in patients who were not on ART at the time of diagnosis of cryptococcal meningitis, i.e., 83.3 % of patients who died were not on ART. Although use of HAART and early detection of HIV infection may eventually lead to a reduction in opportunistic infections, including cryptomeningitis, management of opportunistic infections remains a key facet of AIDS care in India.
Cryptococcal meningitis is an important cause of morbidity and mortality in HIV patients. Awareness of its occurrence might lead to early diagnosis and better treatment options for the patient.
Footnotes
Author Disclosure Statement
No competing financial interests exist.