
Abstract
We evaluated the HIV/AIDS epidemic among men who have sex with men (MSM) in Hunan Province using the Asian Epidemic Model (AEM) and explored the impact of both condom use and standardized STD treatment on HIV prevention programs. The AEM was used to estimate HIV infection under four different scenarios: (1) condom use among MSM maintained at the 2005 level, (2) condom use among MSM improved since 2005, (3) the sexually transmitted infection (STI) prevalence rate among MSM maintained at the 2008 level, and (4) the STI prevalence rate among MSM improved since 2008. Compared with the rate of condom use at the 2005 level among MSM, if the rate of condom use had continuously improved, the number of new infections would have been reduced by 79.1% and the number of people living with HIV and AIDS would decrease by more than 8600 by 2020 and the cumulative number of new infections would have been reduced by 63.6% since 2006 while the number of new HIV infections among females would decline from 2015 with a drop of over 35% by 2020. When compared with the projection based on an unchanged rate of STI infection, the number of new HIV infections would decrease by 49.4% by 2020, and the decreased number of people living with HIV and AIDS would be more than 4000. The total number of 5200 newly infected HIV cases could be reduced from 2006 to 2020 and the number of newly infected HIV cases among the general female population would be reduced by 15.4%. With both the increased rate of condom use and standardized STD treatment for the MSM population in Hunan Province, the spread of HIV infection in both MSM and the general female population would decrease.
Introduction
T
In 2004, funded by the Central Government's Transfer Payments, a condom promotion (100% condom use) program was implemented in all the entertainment establishments in Hunan Province. In recent years, the proportion of condom use related to the latest commercial sex activity among high-risk populations in different entertainment establishments increased from 2–31% to 56–100%, with the majority being more than 80%. Meanwhile, the sales of condoms throughout the province have increased by 50–300%. A Global Fund supported program was started in 2005, which was focused on both condom promotion and standardized sexually transmitted diseases (STD) treatment.
In this article, the Asian Epidemic Model (AEM) was used to estimate the HIV/AIDS epidemic and to explore the impact of condom use and standardized STD treatment on men who have sex with men (MSM) in Hunan Province related to HIV prevention. Globally, enormous manpower and material resources have been devoted to HIV/AIDS prevention. In 2009, the total investment from governments and international organizations had reached 15.9 billion dollars, but this was still insufficient to meet current needs. In 2010 UNAIDS estimated 4 that 10 billion U.S. dollars would be needed to fill in the gap. We need to realize that the money being allocated for HIV/AIDS prevention is not infinite, which makes the evaluation of the effect of various interventions more important in terms of the allocation of resources. Thus, methods of evaluation have become quite important in HIV/AIDS research. Many methods including mathematical modeling have been used to evaluate the effects of interventions, and the AEM was one of them.
The AEM was developed by the East West Center in the United States to estimate the epidemic and simulate the spread of HIV throughout other countries. 5 It could also be used as a useful tool to evaluate the effects of preventive measures. In one research study carried out by Saidel et al. 6 in 2003, the number of HIV infections was estimated in three well-designed "scenarios" to reveal the potential impact of IDUs on their noninjecting sexual partners and to project its role of transmission on epidemics in the general population. The objective of this article is to evaluate the impact of condom use and standardized STD treatment as preventive measures among MSM in Hunan under different scenarios through the application of the AEM.
Description of the AEM
The AEM was developed by Dr. Tim Brown in the East West Center, based on Asian HIV transmission patterns, with funding from the United States Agency for International Development. It has worked well in Asian settings. The AEM provides a useful tool with which to estimate the HIV epidemic, to review policy, and to analyze programs in Asian countries. IDUs, female sex workers (FSWs), and MSM are the major factors affecting the Asian epidemic. With epidemics evolving over time, infected FSW clients and IDU's sexual partners have become the main groups involved in local heterosexual transmission. 7,8 Compared with other models, the AEM is semiempirical, but not theoretical in nature. With behavioral and epidemiological inputs being widely used and Asian transmission patterns involved, the estimation may more closely approximate the real situation.
The AEM is a valuable tool for evaluating preventive methods. When various intervention programs are carried out, behavioral characteristics change over time. The AEM calculates the number of HIV infections and HIV prevalence based on all the parameters that have been input into the model. The model calculates the number of new infections of each transmission pattern based on the number of high-risk behaviors per year and the transmission probability of contacts, adjusted by modifying factors such as STI infection and condom use. According to the natural history of HIV infection, the number of AIDS patients and AIDS deaths can be calculated. The number of new AIDS patients and AIDS deaths yearly is subtracted from the accumulation of new infections, which is the number of existing infections. 5 When behavior parameters are changed, the AEM recalculates the epidemic and outputs a new projection. The variances in HIV prevalence and infection number reflect the impact of preventive methods. Based on the simulation, advice can be given on how to adjust the preventive measures accordingly. 9,10
Sources of data
There are three types of parameters and seven categories of inputs. (1) Biological parameters include the probabilities of HIV transmission via different routes, such as MSM, needle-sharing among IDUs, and mother-to-child transmission. (2) Parameters on epidemiology and demography include factors such as the size of high-risk populations, their proportions in the general population, and the mean duration of high-risk behavior in risk groups. (3) Behavioral parameters include factors such as the proportion of condom use, data on injection behavior and needle sharing, and sexual behavior among IDUs and sex workers. All the data that the AEM model needs can be divided into seven categories: population size, heterosexual risk behavior, homosexual risk behavior, injection behavior, epidemic parameters, prevalence, and situation of migration.
Sources of data involved in this study include the following items: 1. Data regarding HIV epidemics and the size of high-risk populations are from a Workbook estimation of the Hunan Province HIV epidemic undertaken by the Chinese Center for Disease Control and Prevention. 2. Data related to demography and epidemiology are mainly from the surveillance points, offered by the Hunan Provincial Center for Disease Control and Prevention and partially from the published statistical yearbooks and other references.
11
–21
3. Biological parameters, such as the probability of HIV transmission among MSM, on needle-sharing among IDUs, and on mother-to-child transmission, are from published references. 4. Related behavioral data are from published references, selected in descending order as follows: studies conducted in Hunan Province, in other Chinese provinces, and from published foreign studies.
Materials and Methods
In this study, the AEM is used to estimate HIV infection in various populations under different scenarios. 6 Based on the estimation, the impact of condom use and standardized STD treatment among MSM in Hunan Province on HIV prevention is evaluated.
Based on the epidemiological pattern in China, seven different populations have been involved in this study: clients of the FSWs, general males, MSM, male sex workers (MSW), general females, FSWs, and IDUs. In addition, each group is divided into uninfected or infected. As individuals often move from one group to another, changes in the population need to be considered. The overriding consideration of the AEM has been the rate of HIV infection among the adult population group (15–49 years old). HIV infection among children is calculated from related parameters such as fertility rate of the females, HIV prevalence, and mother-to-child transmission.
As previously shown, three types and 137 parameters have been collected.
A series of equations was used to calculate the new infection numbers for every transmission route. Based on an overall consideration of new infections and the natural history of HIV infection and AIDS, the AEM calculates the number of people living with HIV, new AIDS patients, and HIV-related deaths on a yearly basis. HIV prevalence rates and the impact of preventive measures are calculated for different levels of condom use and standardized STD treatment among MSM in Hunan Province.
Results
Projection on the HIV epidemic
The results show (Table 1) that the number of HIV infections in Hunan Province remained low prior to 1994, indicating a slow growing period for HIV/AIDS. However, the number increased rapidly between 1995 and 2006, indicating a relatively fast HIV growing period. From 2007 to 2020, a slow growing trend in the HIV epidemic is illustrated, with no downward trend in HIV infections as shown in Fig. 1 before 2020.
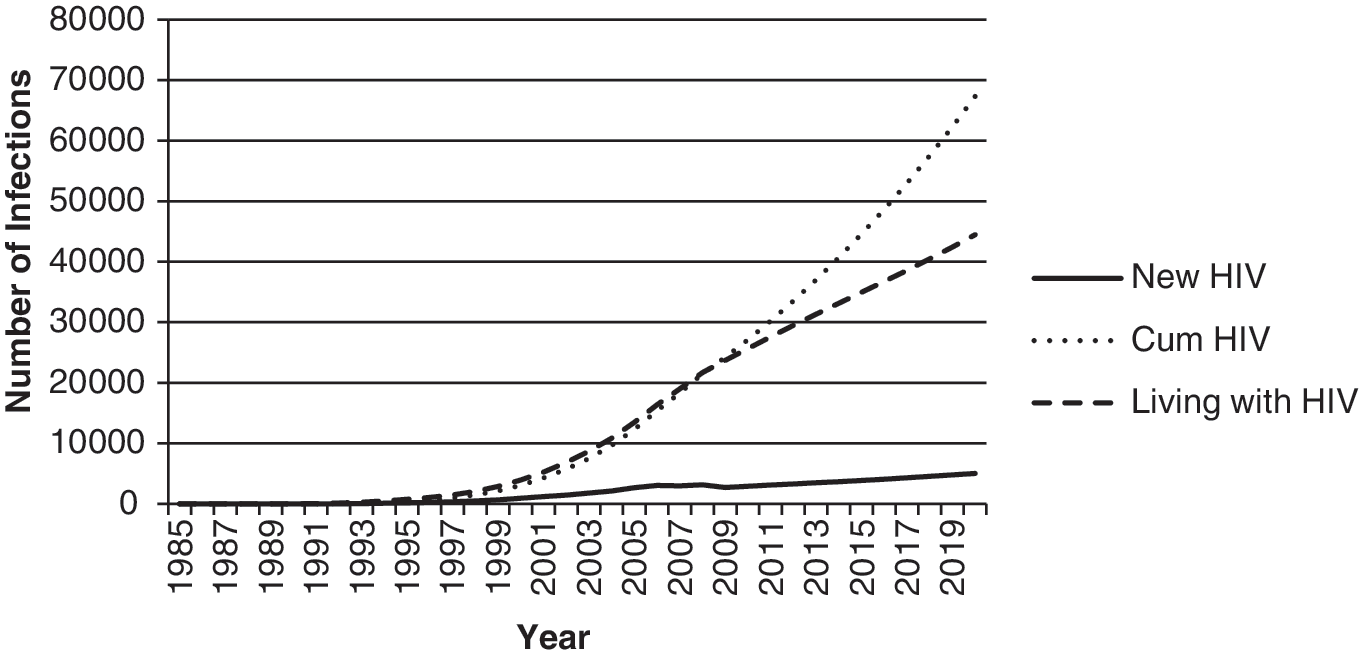
Estimations and projections of HIV infections in Hunan Province with the Asian Epidemic Model (AEM).
AEM, the Asian Epidemic Model.
The HIV/AIDS epidemic was mainly spread by IDUs at the earlier stage in Hunan Province, followed by sexual transmission, with heterosexual transmission dominating. The main populations involved include IDUs, FSWs, and their clients. Subsequently, changes took place concerning the AIDS epidemic, dominated by sexual transmission. In particular, the fast-growing spread of heterosexual transmission, along with the declining numbers in IDUs but growing numbers in MSM, is shown in Table 2. The number of HIV infections among MSM increased rapidly after 2010 as shown in Fig. 2, and is much higher than that of other groups, indicating that effective measures should be taken for this targeted high-risk population now and in the future.
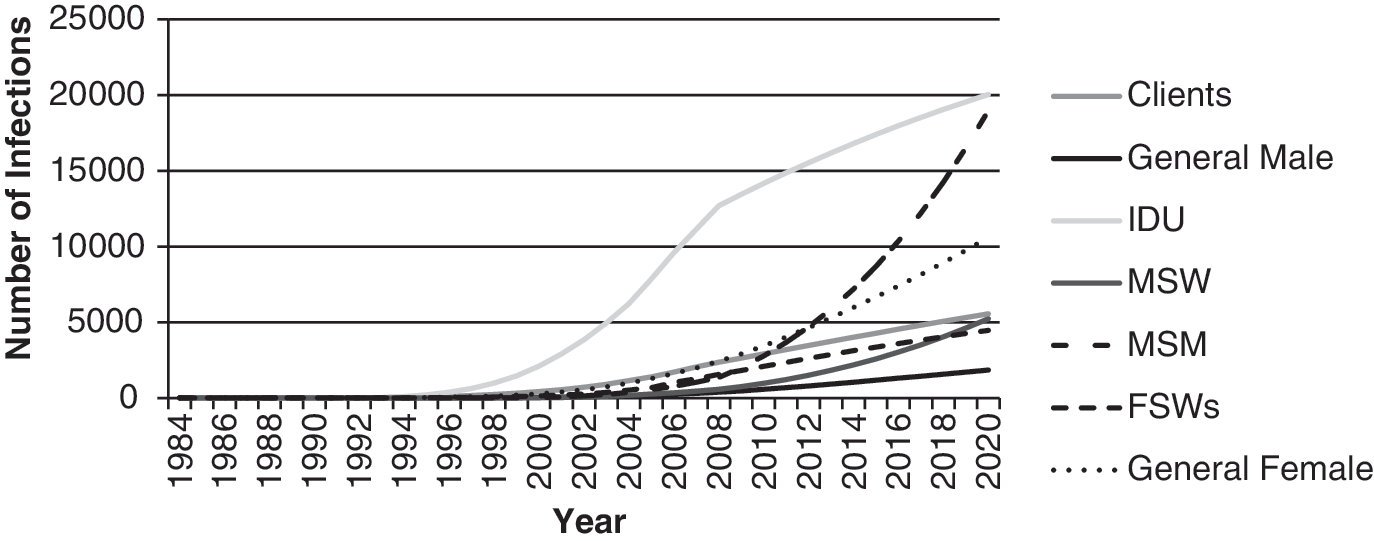
Estimations and projections of the cumulative number of HIV infections by groups in Hunan Province with the AEM.
AEM, the Asian Epidemic Model; IDU, intravenous drug user; MSW, men who have sex with women; MSM, men who have sex with men; FSWs, female sex workers.
Evaluation of the effect of HIV control by promoting condom use among MSM with the AEM
The HIV/AIDS epidemic has been growing rapidly in Hunan Province with MSM the hardest hit. As a result, a province-wide condom promotion project was launched in 2005 with MSM the target population. An effect assessment was performed by the AEM by comparing the new infection rates between groups using condoms and those groups not using them.
As shown in Table 3 and Fig. 3, the number of HIV infections among MSM would have increased gradually year by year if no condom promotion project had been in effect. Since the implementation of the project, the rate of condom use has been on the rise and the results calculated through the indicator in the model show that the number of new infections among MSM was reduced significantly after 2009, with a further decline projected after 2016, indicating that this measure has a significant protective effect against HIV infection. Compared with the unchanged rate of condom use at the 2005 level among MSM, if the rate of condom use continuously improves, the number of new infections would be reduced by 79.1% and the decrease in the number of people living with HIV and AIDS would exceed 8600 by 2020. Again, the cumulative number of new infections would have been reduced by 63.6% since 2006.

Projections of new HIV infections under different condom use rates among men who have sex with men (MSM) with the AEM.
AEM, the Asian Epidemic Model; STI, sexually transmitted infection.
Promotion of condom use can not only reduce the HIV infection rate among MSM, but can also benefit the general population (as shown in Fig. 4). The number of new HIV infections among general females will decline from 2015 and drop by more than 35% by 2020 if there is continuous improvement in the rate of condom use.
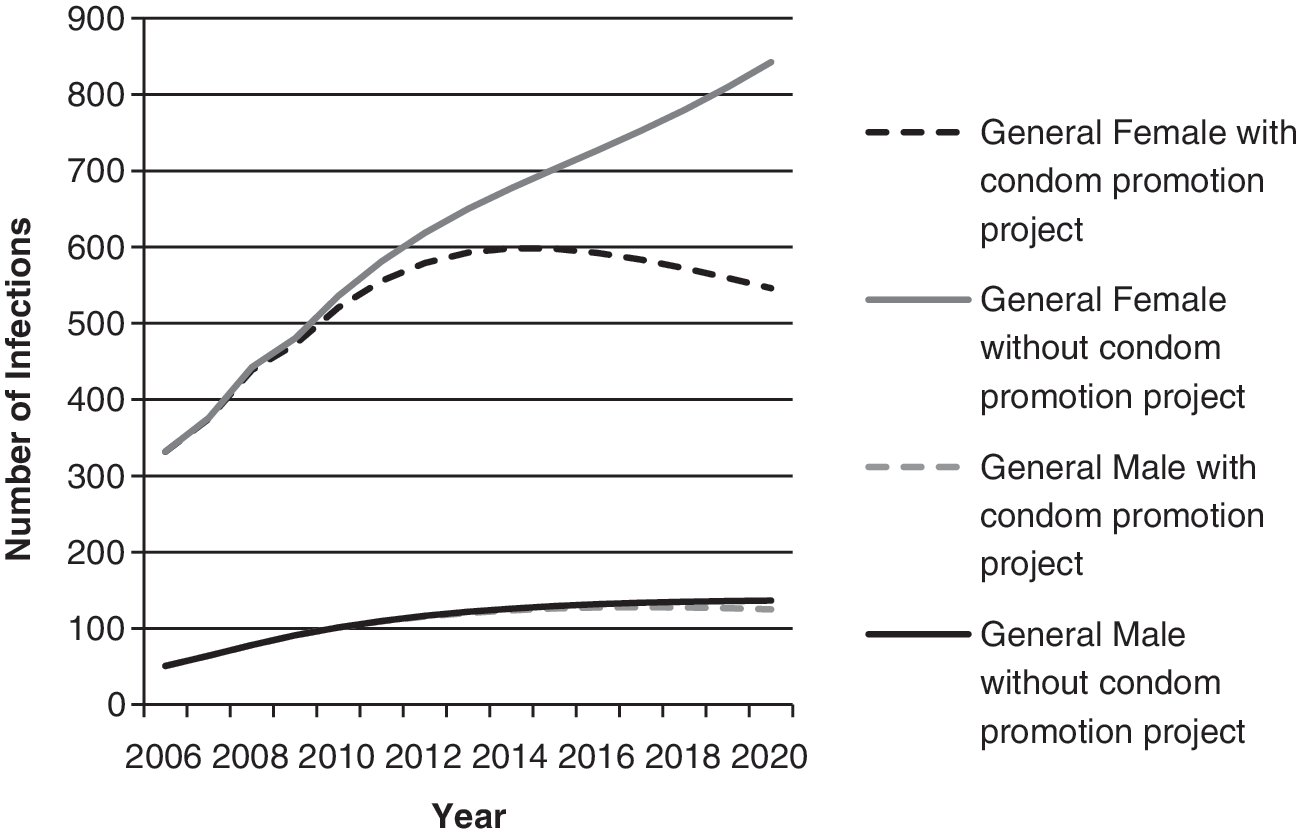
Projections of new HIV infections under different condom use rates among the general population with the AEM.
Projection of the effect through treatment of STDs using the AEM
To study the effect of STI reduction on HIV infection among MSM, it was assumed that the STI prevalence rate among MSM was maintained at a constant rate or there was less than a 1% annual decline after 2008, and that it ultimately was maintained at a 5% level. The HIV infection rates are then projected, respectively. The results are shown in Fig. 5.
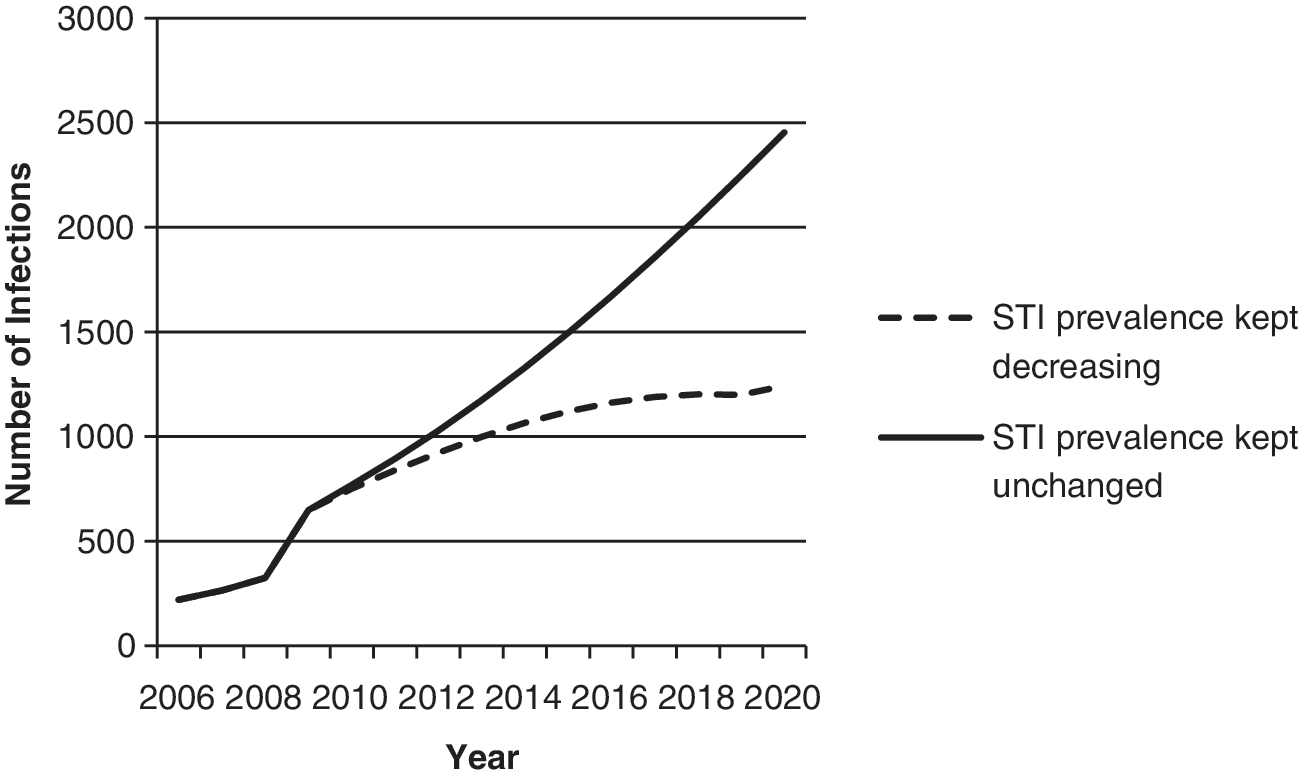
Projections of new HIV infections under different sexually transmitted infection (STI) prevalence rates among MSM with the AEM.
As shown in Fig. 5, if the STI infection rate among the MSM population remains at the 2008 level, new HIV infections will continue to increase at a higher rate, and the number of new infections will exceed 1500 after 2015, with no sign of easing until 2020. Meanwhile, the number of people living with HIV and AIDS will exceed 10,000 by 2017, without any trend of decreasing in the foreseeable future. If measures are taken to reduce the STI prevalence rate in a continuous way (with the assumption of an annual 1% rate of decline), the growth rate of new HIV infections will significantly slow down, and even remain at a low level after 2015. The increase in the number of people living with HIV and AIDS will then become more moderate, and when compared with the projection based on an unchanged rate of STI infections, the number of new HIV infections will have decreased 49.4% by 2020. The reduced number of people living with HIV and AIDS will exceed 4000, with a total number of 5200 reductions in new HIV infections from 2006 to 2020 (Table 3).
As a large proportion of MSM have sex with both male and female partners in China, the reduction of STI infection rate among MSM can not only reduce HIV transmission within the MSM population, but also lower HIV intertransmission between different populations. Figure 6 shows variations in new HIV infections in general male and female populations based on different assumptions. The number of new HIV infections among general females changes from its original slow growing status to a stabilized level, around 700 cases each year, based on a low STI infection rate among MSM populations. Compared with the unchanged STI infection rates, the number of new HIV infections among general females will be reduced by 15.4%. Variations of STI infection rates among the MSM population seem to have a minimum effect on new HIV infections among general males.
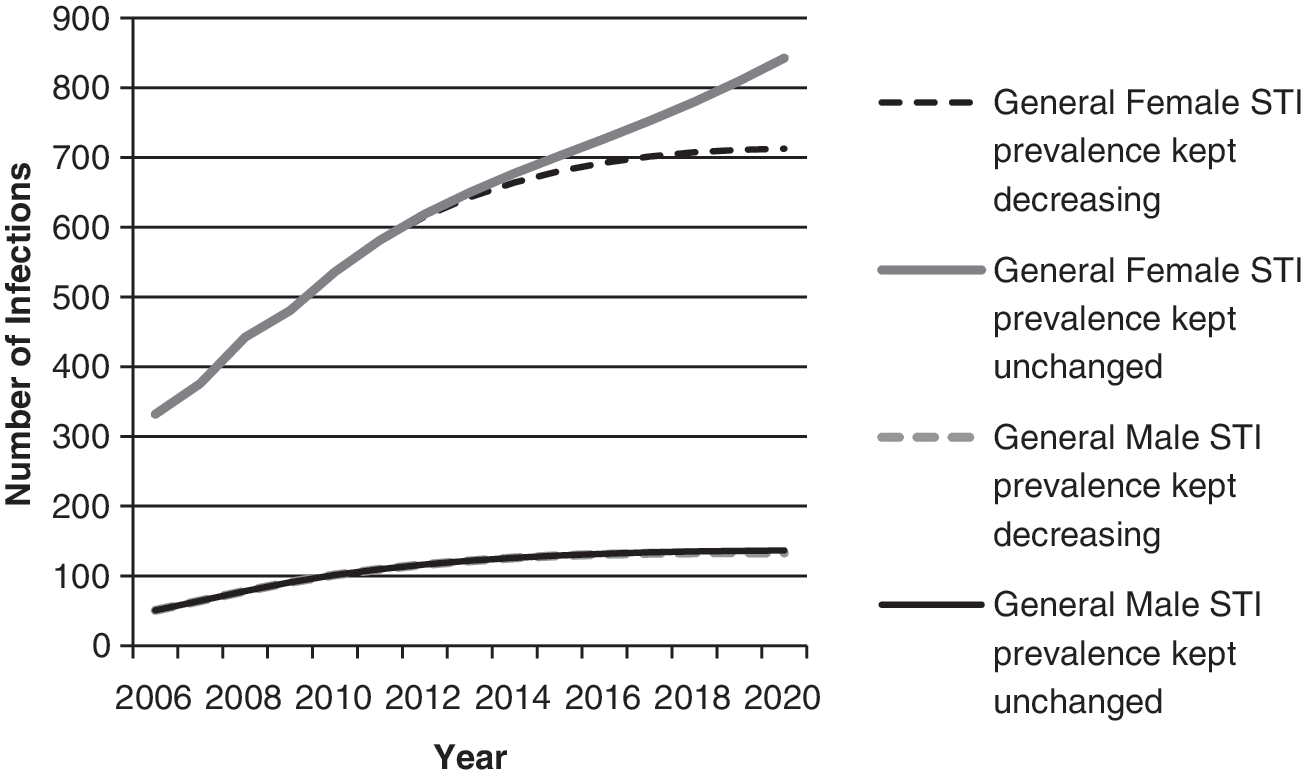
Projection of new HIV infections under different STI prevalence rates among the general populations with the AEM.
Discussion
Our research findings indicate that factors such as the transmission modes of HIV in Hunan Province, with an early spread mainly through IDUs, followed by a trend toward sexual transmission and homosexual transmission, are rapidly dictating the major characteristics of the HIV epidemic in the province. This change is in agreement with variations in the AIDS epidemic in China and with literature reported in Hunan Province. The change in the mode of HIV transmission suggests that the focus of AIDS interventions in Hunan Province will need to shift to control the transmission through sexual activities; both homosexual and heterosexual transmission should receive special attention, with the MSM population in particular, in the years to come. HIV transmission in this population seems to be rapid, with the cumulative survival numbers of infections significantly increasing within a short time; this indicates that if measures promoting condom use and control of STI infections continue, the epidemic will slow down and it will be possible to avoid the rapid growth of infection.
The AEM model can be used not only to estimate the AIDS epidemic and to forecast its trend, but also to explore different possible impacts on the epidemic by designing different “scenes” to simulate the implementation of intervention programs. In 2003, 6 a study using the AEM model simulated three scenarios in intravenous drug users. It compared times before the HIV epidemic, at the same time as the HIV epidemic, and after the HIV epidemic in the general population (mainly through heterosexual transmission) and estimated how these affected the infection rate among the whole population. Assumptions were also made to determine how intervention programs begun at different stages among intravenous drug users can affect the total number of infected cases. Research 22 carried out in Shenzhen China also used the AEM model to estimate the effect of intervention programs implemented individually or integrated, and incorporated with the disease control targets, in providing the basis for the determination of prevention and control measures.
In this study, during the adjustment process of the model parameters, we notice that condom use and STD infection rates are highly sensitive indicators in every population while the change of estimated numbers of HIV infections can significantly affect the results, especially for sexually transmitted infections. The change can affect the rate of HIV transmission not only within a single population, but also between populations, and can further be magnified by those factors. In practical preventive programs, these two indicators can be controlled by strengthening intervention programs. If specific measures can be implemented and improved, good results will be achieved, suggesting that the intensity of such interventions should be continued and strengthened to control the AIDS epidemic.
Because the AEM model requires extensive HIV epidemiological and behavioral data and indices, inevitably it also contains some shortcomings, with an excessive reliance on a large number of monitoring data in particular. Before choosing to use the AEM model, it is necessary to assess the availability of the model and to determine how representative those local relevant data are. The AEM model is adequate only when there are sufficient data sources. Otherwise, the model is not suitable for the estimation and projection of HIV/AIDS epidemics. Because this study is restricted to the architectural design of the AEM, biomedical interventions such as antiretroviral therapy (ART) for prevention, preexposure prophylaxis, and ART-loaded rectal microbicides are not presented. To explore the impact of these biomedical interventions, the calculation mechanisms of the AEM must be redesigned.
Footnotes
Author Disclosure Statement
No competing financial interests exist.