
Abstract
Knowledge of the genetic diversity of HIV-1 constitutes a fundamental premise in the epidemiological surveillance. In the present study, the HIV-1 genetic variability from 142 Cuban patients who were diagnosed with HIV-1 infection during 2009 and 2010 was determined. HIV-1 subtypes were determined by partial RT-PCR and sequencing of the HIV-1 pol gene. The phylogenetic analysis showed that 47 (33.1 %) samples were subtypes B and 95 (66.9 %) were non-B subtypes, where G, H, and C subtypes, as well as the recombinant forms CRF19_cpx, CRF18_cpx, and CRFs BG, were included. The circulation of CRF05_DF was detected for the first time in Cuba. The analyses of recombinants showed the presence of recombinant CRF18_cpx/CRF19_cpx. The study confirms the high genetic diversity of HIV-1 and the circulation of new genetic variants in the studied population, which indicates the importance of maintaining constant epidemiological surveillance in Cuba.
B
The epidemiology of HIV is constantly changing, due to travel, migrations, as well as the social and cultural changes that influence the global distribution and prevalence of the subtypes. Subtype C accounted for nearly half (48%) of all global infections, followed by subtypes A (12%) and B (11%), CRF02_AG (8%), CRF01_AE (5%), and subtypes G (5%) and D (2%). Subtypes F, H, J, and K together caused fewer than 1% of infections worldwide. 2
Although initial studies reported that subtype B was the predominant genetic form in Cuba, a mosaic of subtypes and recombinant viruses has been described subsequently. 3,4 The knowledge of the genetic diversity of HIV-1 constitutes a fundamental premise in the surveillance of the epidemic, because the variation among the different subtypes can affect the development of new therapeutic strategies. The goal of the present study was to characterize the HIV-1 genetic diversity in recently diagnosed Cuban patients.
For this purpose, 142 HIV-infected patients diagnosed between 2009 and 2010 were included in the study. Written informed consent from each subject was obtained. Patient age, sex, transmission route, and province were determined at the time of diagnosis.
Patients were categorized as either recently or chronically infected, according to the presence or not of documented seroconversion in the preceding 12 months or clinical evidence of acute HIV infection. 5 Plasma HIV RNA was quantified using the COBAS Ampliprep/COBAS Taqman HIV-1 Test (Roche Diagnostics GmbH, Mannheim, Germany) with a limit of detection of 40 copies/ml. For the genotypic analysis, viral RNA was isolated from 200 μl of plasma using the High Pure Viral Acid Nucleic Acid kit (Roche Diagnostics, GmbH, Mamheim, Germany).
The pol gene was amplified from positions 2143 to 3798 (HXB2 numbering) by reverse transcriptase-polymerase chain reaction (RT-PCR) followed by nested PCR, and sequenced in a CEQ 8800 sequencer (Beckman Coulter, Fullerton, CA), as described.
6
Phylogenetic analyses were performed with neighbor-joining trees, based on Kimura's two parameter distances, using MEGA 3 program.
7
Sequences were individually analyzed by SimPlot 2.5 and jpHMM.
8,9
The reliability of tree topologies was assessed by bootstrapping with 1000 replicates, with a bootstrap support of ≥50%. Reference sequences of viruses included in the phylogenetic analyses were downloaded from the Los Alamos database (
Categorical data were analyzed using the X 2 test. A comparison of two proportions with independent samples was carried out. For all statistical tests a p value ≤0.05 was considered significant.
Table 1 shows the baseline characteristics of patients included in the study. Twenty individuals were identified as recently infected, whereas 122 individuals were characterized as chronically infected. No significant differences were detected when comparing the proportions of recently infected with chronically infected patients, according to transmission route, age, and viral load.
No., number; SD, standard deviation; IQR, interquartile range.
A phylogenetic tree constructed using sequences from the pol region of isolates included in the study is shown in Fig. 1. Our analysis showed that 47 (33.1%) samples were grouped with reference sequences of the subtype B, genetic forms predominant in the present study. A group of 39 (27.5%) samples was grouped with reference sequences of the CRF 19_cpx and 22 (15.5%) sequences formed a cluster with reference sequences of the recombinants BG, where three subclusters corresponding to CRFs 20, 23, and 24 were evidenced. Another cluster of 22 (15.5%) samples was grouped with the reference sequences corresponding to CRF18_cpx.
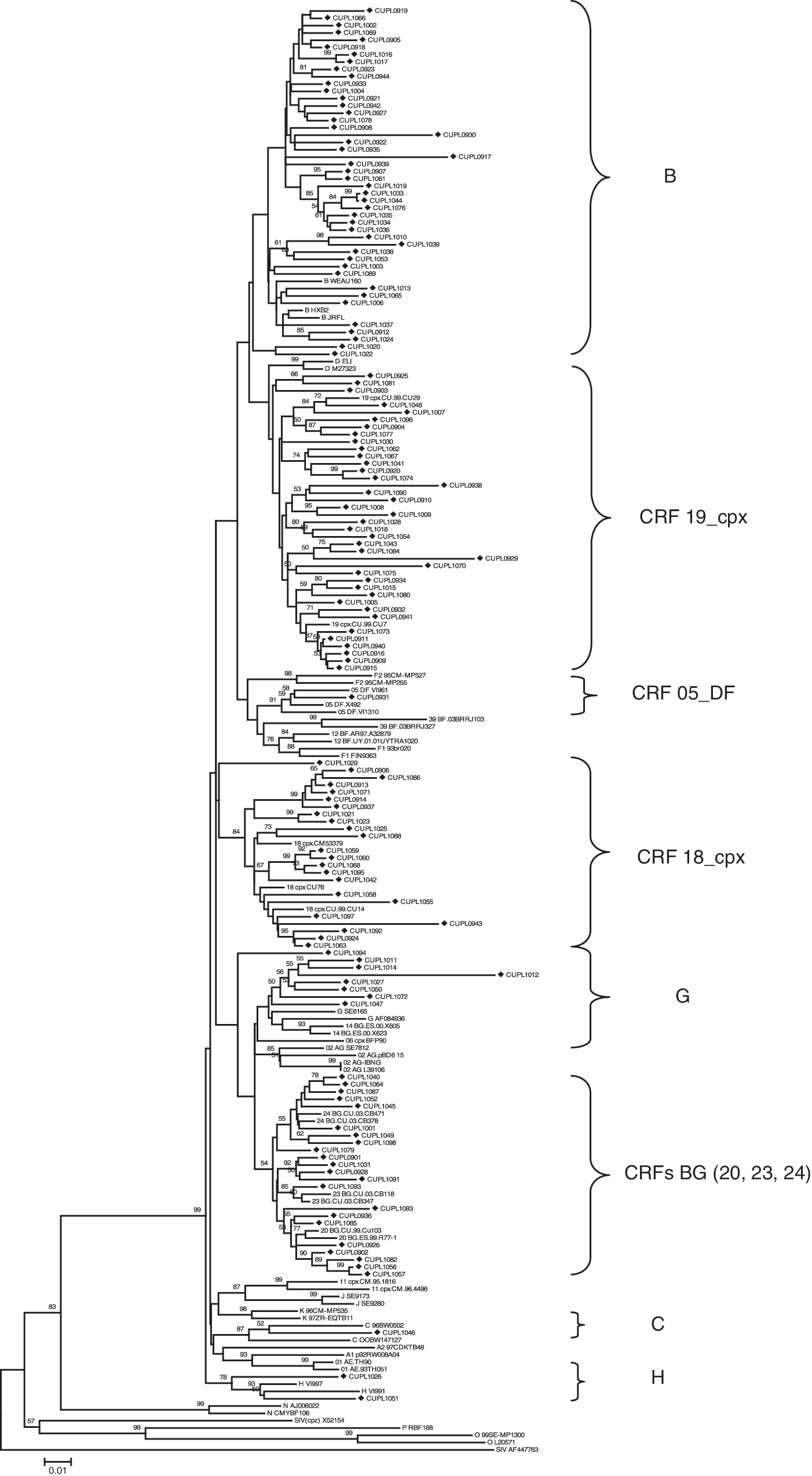
Neighbor-joining tree using pol sequences from the 142 HIV-1-infected Cuban patients diagnosed during 2009 and 2010. The tree was constructed using Kimura's two parameter distances. Bootstrap values ≥50% are shown. Subtype and CRF reference viruses are denoted by the corresponding subtype or CRF names followed by the name of the isolates. Viruses whose names begin with CUPL correspond to the Cuban viruses of this study.
Inside the same one, eight sequences were grouped in a subcluster; the subtype was determined using the REGA HIV subtyping tool (

Recombinants analysis.
Eight (5.6 %) samples were grouped with strains of subtype G, two (1.4%) samples with reference sequences of the subtype H, one (0.7%) sample with subtype C, and one (0.7%) sequence with reference strains corresponding to CRF05_DF. The detection of CRF 05_DF constitutes the first report of the circulation of this variant in the Cuban epidemic.
The analysis of recombination by bootscanning and jpHMM of the sample classified as CRF 05_DF showed a breakpoint between subtypes D and F1, in the nucleotide positions 2572 and 2607 (HXB2 numbering) of the pol gene (Fig. 2b). The distribution of HIV-1 subtypes and recombinant forms for 142 individuals included in the study is presented in Table 2.
Previous studies of molecular epidemiology reported a high prevalence of subtype B in the Cuban population infected with HIV-1. 3,4 However, an important element to consider is that 66.9% of the analyzed samples were classified as non-B subtypes, which indicates a decrease in subtype B, in comparison with previous reports. 3.4 One explanation for the decrease of this subtype in the population of recently diagnosed and treated naive patients is the considerable increase in the proportion of CRF 19_cpx (recombinant between the subtypes A1, G, and D) 10 (p=0.016) in comparison with the results obtained by Pérez et al. in 2007 and the expansion of the CRFs BG (20, 23, and 24) that present the parental strains of subtypes B and G in their mosaic structure. 11,12 Similar behavior has been described in countries such as Brazil and Argentina, with the expansion of the recombinant forms BF in the seropositive population and in regions denominated geographic hot spots, such as Eastern Africa, southeast Asia, and central Myanmar, in those that cocirculate diverse variants of HIV-1 and emerge as new recombinant forms. 13
Two samples classified as subtype H (CUPL1026 and CUPL1051) were isolated from two women from Artemisa and Cienfuegos provinces, respectively. Previous studies reported that the prevalence of subtype H is remarkable in Santiago de Cuba. 12
CRF 05_DF was detected in a heterosexual woman from Havana. This genetic variant has been reported in Belgium, the Democratic Republic of Congo, Spain, and Costa Rica. 14 The report of this variant in Cuba emphasizes the importance of maintaining epidemiological surveillance programs in recently diagnosed populations and it is an indication that illustrates the dynamics of the Cuban epidemic in relation to the genetic diversity described by other authors. 3,4,11
Several authors have described the circulation of CRF 18_cpx and CRF 19_cpx in Cuban patients 10,15 ; for this reason the recombination among both complex forms in the infected population is not a new fact in the Cuban epidemic. In 2006, Pérez et al. reported this genetic variant in two out of 425 patients (0.5 %) studied. 12 Of the eight samples classified as CRF18_cpx/CRF19_cpx in our study, one individual (CUPL0906) was classified as recently infected, which constitutes an indication of the transmission of this recombinant form. Among these patients there is no evidence of an epidemiological relationship, although all come from the Western region of the country (Havana, Mayabeque, and Matanzas) and 87.5% (7/8) have engaged in homosexual conduct.
In conclusion, this study confirms the high genetic variability of HIV-1 in a group of patients diagnosed between 2009 and 2010, and the circulation of the unique recombinant CRF 18_cpx/CRF 19_cpx and of the CRF 05_DF, which constitutes the first report of the circulation of this genetic variant in Cuba. The analysis of the pol gene in this study made it possible to confirm the frequency and diversity in recombinant forms, which is changing in the course of time in comparison to previous reports carried out in Cuba. The results obtained will be a great contribution to the program of epidemiological surveillance; it would also reinforce the studies about the implications of HIV-1 genetic diversity, the pathogenesis, the development of vaccines, and the design of new therapeutic strategies.
Sequence Data
GenBank accession numbers for the sequences reported here are from HQ655334–HQ655409 and JN000005–JN000070.
The accession numbers of HIV-1 pol reference strains used in the phylogenetic analysis are as follow: p92UG037A40, AB253429; p92RW008A04, AB253421; CY01741, AF286237; 97CDKTB48, AF286238; WEAU1-60, U21135; HXB2, K03455; JRFL, U6363; OOBW1471.27, AF443091; 96BW05.02, AF110967; ELI, K03454; M27323; 93br020, AF005494; FIN9363, AF075703; 95CM-MP535, AJ24923; 95CM-MP255, AJ249236; AF084936; SE616, AF061642; VI991, AF190127; VI997, AF190128; SE9173, AF082395; SE9280, AF082394; 96CM-MP535, AJ249239; 97ZR-EQTB11, AJ249235; RBF168, GQ328744; L39106; SE7812, AF107770; VI1310, AF193253; VI961, AF076998; BFP90, AF064699; 99FR-MPI307, AJ291720; URTR23, AF385934; ARMA159, AF385936; X605, AF450096; X397, AF423756; CU76, AY586540; CM53379, AF377959; CU14, AY586541; CU38, AY588970; R77, AY586544; CB134, DQ020274; CB347, AY900572; CB118, AY900571; CB619, AY900576; CB378, AY900574; CMYBF106, AJ271370; AJ006022; 99SE-MP1300, AJ302647; CIV, X52154.
Footnotes
Acknowledgments
The authors thank Dr. Felipe Rolo, Dr. Eladio Silva, Dr. Otto Cruz, and Lic Maria D. Bermudez for their useful comments and manuscript revision. These data were presented in part at the 6th Conference on HIV Pathogenesis, Treatment and Prevention (IAS 2011), Roma, Italy, July 2011 (abstract MOPE039).
Author Disclosure Statement
No competing financial interests exist.