
Abstract
The rates of virological failure (VF) and HIV-1 drug resistance were evaluated in a cross-sectional study in HIV-1-infected children living in Dakar, and taking antiretroviral treatment (ART) according to WHO recommendations. The plasma HIV-1 RNA load was measured using the Abbott m2000 RealTime HIV-1 assay. The full-length protease gene and partial reverse transcriptase gene were sequenced, and resistance mutations were assessed by reference to the Stanford University HIV drug resistance database. Of 125 included children (median age, 7 years) taking first-line ART for a median duration of 20 months, 82 (66%) showed detectable HIV-1 RNA load, and 70 (56%) met the 2010 revised WHO criteria of VF (defined as plasma HIV-1 RNA load ≥3.7 log10 copies/ml). Drug resistance results were available for 52 children with plasma HIV-1 RNA load ≥3.0 log10 copies/ml, and viruses carrying resistance mutations were found in 48 (92%) children. Among these 48, mutations conferring resistance to nucleoside reverse transcriptase inhibitors (NRTIs) or non-NRTIs (NNRTIs) were found in 42 (88%) and 47 (99%) children, respectively. The NRTI-resistant viruses harbored the M184V/I (95%), Q151M (2%), and thymidine-analogue mutations (40%), and the NNRTI-resistant viruses harbored the K103N (34%), Y181C (32%), G190A (23%), and K101E (21%) mutations. A high rate (56%) of VF was demonstrated in Senegalese children after 20 months of first-line ART and therapeutic failure was assessed by the presence of antiretroviral drug resistance mutations in 9 out of 10 children in VF. These findings point out the difficulties of optimizing ART in children living in sub-Saharan Africa, and the crucial need of laboratory monitoring reinforcement.
Introduction
M
Children are highly vulnerable to HIV infection, and ART failure, especially in resource-limited settings. Previous studies examining ART in children primarily infected with non-B HIV-1 subtypes have identified several specific difficulties in treating pediatric HIV infection in a sub-Saharan Africa. 5 The principal factors compromising ART efficacy in HIV-infected children include the limited number of available pediatric-formulated antiretroviral drugs, the frequently observed poor adherence to drug therapy schedules, and an increased viral load, which may favor the risk of therapeutic failure and drug resistance. 6 –10 While virological failure (VF) is variably defined according to different studies, high rates of VF have been reported in African children treated with ART, ranging from 13% to 75%. 5,6,10,11 –13 Furthermore, plasma HIV-1 variants resistant to at least one antiretroviral drug were found in 71–100% of children with a detectable plasma viral load while on ART. 5,6,8,11,12,14 The wide heterogeneity in the reported data examining VF in HIV-positive pediatric patients in Africa also suggests that the quality of the public health system could constitute a significant contributing factor in therapeutic failure. 15
For more than 10 years, Senegal has been developing an operational, structured program to prevent the spread of HIV and to provide health care for HIV-infected patients. Therefore, the HIV epidemic has remained concentrated, with a low prevalence in the general population. 1 In addition, the Senegalese Antiretroviral Drug Access Initiative provides free antiretroviral drugs to infected patients. In adults, the rate of therapeutic success was similar to that generally observed in developed countries, reaching 84% after 24 months of highly active ART, 16 indicating the efficacy of the health care afforded to HIV-infected individuals in Senegal.
However, Senegalese pediatric cohorts receiving ART still have not been biologically evaluated, despite the high risk of therapeutic failure in antiretroviral drug-treated children previously reported in several African countries. 5,14 This prompted us to evaluate the rate of VF as well as the rate of therapeutic failure as assessed by drug resistance mutation profiles, in a cohort of HIV-1-infected children living in Dakar and receiving first-line ART according to the World Health Organization (WHO) recommendations for resource-constrained countries. 17
Materials and Methods
Study population
In 2010, a cross-sectional study of HIV-1-infected children followed at the Hôpital d'Enfants Albert Royer of Dakar was conducted. In this principal health care center for pediatric AIDS in Senegal, physicians used the 2006 revised WHO recommendations for the management of pediatric HIV infection. 17 Thus, ART was indicated based on clinical staging and the CD4 T cell count. The recommended ART in children was a combination of two nucleoside reverse transcriptase inhibitors (NRTIs) with one non-NRTI (NNRTI). 17 Children, aged less than 15 years, and treated with NRTI- and NNRTI-based first-line ART for at least 6 months, were included for the study. Feedback was given to the pediatricians and children's parents on all tested parameters carried out during the study period.
Virological analyses
Two aliquots of a K3-EDTA blood sample obtained by venipuncture in pediatric Vacutainer tubes (Becton Dickinson, Franklin Lakes, NJ) was obtained and plasma was kept at −80°C until processing.
The plasma HIV-1 viral load was measured using the Abbott m2000 Real Time HIV-1 assay (Abbott Molecular, Des Plaines, IL). The lower limit of detection for the assay is 40 copies/ml. 18
Genotypic resistance testing was performed in treated children whose HIV-1 RNA load was greater than 3.0 log10 copies/ml at the time of virological analysis. HIV-1 RNA was extracted from plasma samples using the QIAamp Viral RNA Extraction Kit (Qiagen, Valencia, CA). Sequencing of the protease and reverse transcriptase (RT) genes was performed according to the consensus technique of the Agence Nationale de Recherches sur le SIDA et les Hépatites Virales (ANRS, Paris, France), as previously described.
19
Genotypic resistance was defined as the presence of antiretroviral drug resistance mutations associated with impaired drug susceptibility, using the Stanford University HIV drug resistance database (
The protease and RT sequences were submitted to GenBank with the following accession numbers: HM002496, HM002497, HM002502, HM002505 to HM002508, HM002510, HM002512 to HM002521, HM002523, HM002524, HM002526, HM002528 to HM002533, HM002535, HM002537 to HM002541, HM002545, JN193483 to JN193492, and JN193494 to JN193501.
Results
Study population and HIV-1 RNA load distribution
A total of 125 HIV-1-infected children receiving first-line ART for at least 6 months were included. The median age was 7 years [interquartile range (IQR), 2–15 years], and 51 (40%) were female. The main therapeutic combination used was zidovudine (AZT)/lamivudine (3TC)/nevirapine (NVP). The median duration of treatment was 20 months (IQR, 6–120 months).
Among the 125 children, 60 had viral load at 6 months of ART, 75 had viral load at 12 months of ART, and 66 had viral load at 24 months of therapy. The rates of virological failure according to 2010 revised WHO criteria, after 6, 12, and 24 months of ART, were 32%, 53%, and 55%, respectively.
Among the 125 study children who had virological analysis carried out after a median duration on ART of 20 months, 43 (34%) had an undetectable HIV-1 viral load whereas 82 (66%) displayed detectable HIV-1 viremia, with a median viral load of 5.0 log10 copies/ml (IQR: 2.0–7.0 log10 copies/ml) (Fig. 1): eight (6%) children showed a detectable HIV-1 RNA load less than 3.0 log10 copies/ml, four (3%) had a plasma HIV-1 RNA load between 3.0 and 3.7 log10 copies/ml, and 70 (56%) displayed a viral load greater than 3.7 log10 copies/ml (5,000 copies/ml), e.g., the threshold of VF according to the 2010 revised WHO criteria. 21

Distribution of plasma HIV-1 RNA viral load in 125 children receiving first-line antiretroviral treatment according to the WHO recommendations, and followed-up in the Hôpital d'Enfants Albert Royer of Dakar, Senegal. The threshold of HIV-1 RNA load detection of the Abbott m2000 RealTime HIV-1 assay (40 copies/ml) and the threshold of virological failure according to the 2010 revised (5,000 or 3.7 log10 copies/ml) WHO criteria are indicated.
Among the 43 children with undetectable plasma HIV-1 RNA load, 22 (51%) never had an interruption in treatment, based on pharmacy refill records. The remaining 21 children (49%) had at least one treatment interruption, with a median duration of 53 days (IQR, 20–150 days). Of the 82 children with detectable HIV-1 RNA load, 59 (72%) had at least one treatment interruption with a median duration of 60 days (IQR, 12–160 days). The percentage of episodes of treatment interruption was higher in children with detectable HIV-1 RNA load than in those with undetectable load (p<0.025 by χ2 test). A possible relationship of treatment interruption and treatment complication or side-effects could not be documented.
Genotypic resistance profiles
Genotypic resistance test results were available for viruses isolated from the plasma of 52 study children with HIV-1 RNA load greater than 3 log10 copies/ml. The median duration of ART at the time of genotyping was 26 months (IQR, 8–84 months). The antiretroviral drug combinations used were AZT/3TC/NVP (65%), stavudine (d4T)/3TC/NVP (19%), AZT/3TC/efavirenz (EFV) (12%), d4T/3TC/EFV (2%), and AZT/abacavir (ABC)/EFV (2%). The median viral load at the time of genotyping was 4.9 log10 copies/ml (IQR, 3.2–6.8 log10 copies/ml); 49 (94%) children were in VF according to the WHO 2010 revised criteria. Based on pharmacy refill records, at least one treatment interruption occurred in 45 (87%) out of the 52 children.
Among the 52 children with available genotypic results, only four children (8%) had viruses remaining sensitive to NRTI, NNRTI, and protease inhibitor (PI) classes. Mutations conferring resistance to at least one antiretroviral drug were found in 48 (92%) children, and resistance to both NRTIs and NNRTIs was present in 42 (88%) children.
Three out of the 48 (6%) children whose viruses showed drug resistance mutations had plasma HIV-1 RNA load between 3.0 and 3.7 log10 copies/ml. Based on WHO 2010 VF criteria, these children would not have been included.
The median number of drug resistance mutations observed was three (ranging from one to nine mutations). No correlation could be found between that median number of drug resistance mutations and therapy duration (by linear regression; p>0.05).
NRTI resistance mutations
Major mutations conferring drug resistance to NRTIs were found in viruses isolated from 42 (88%) of the 48 children with drug-resistant viruses. The M184V/I mutation was identified in viral isolates from 40 (95%) of the 42 children with NRTI-resistant viruses, while the Q151M mutation was detected in only one (2%) of these children (Fig. 2A). The patient with Q151M had been receiving AZT/3TC/NVP for 34 months and had 90 days of treatment interruption. Thymidine-analogue mutations (TAMs) were present in viruses from 17 (40%) of the 42 children, and included the following mutations: T215Y/F in 16 genotypes (38%), L210W in eight (19%), M41L in eight (19%), D67N in five (12%), K70R in four (10%), and K219Q/E in four (10%). Of the 17 children infected with TAM-containing viruses, eight (47%) carried viruses with at least three TAMs. The M184V mutation was found in combination with at least one TAM in viral isolates from 16 (38%) of the 42 children infected with NRTI-resistant viruses. If the M184V mutation was excluded, eight (17%) children who received a first-line regimen had viruses harboring at least one drug-resistant mutation to an NRTI or NNRTI.
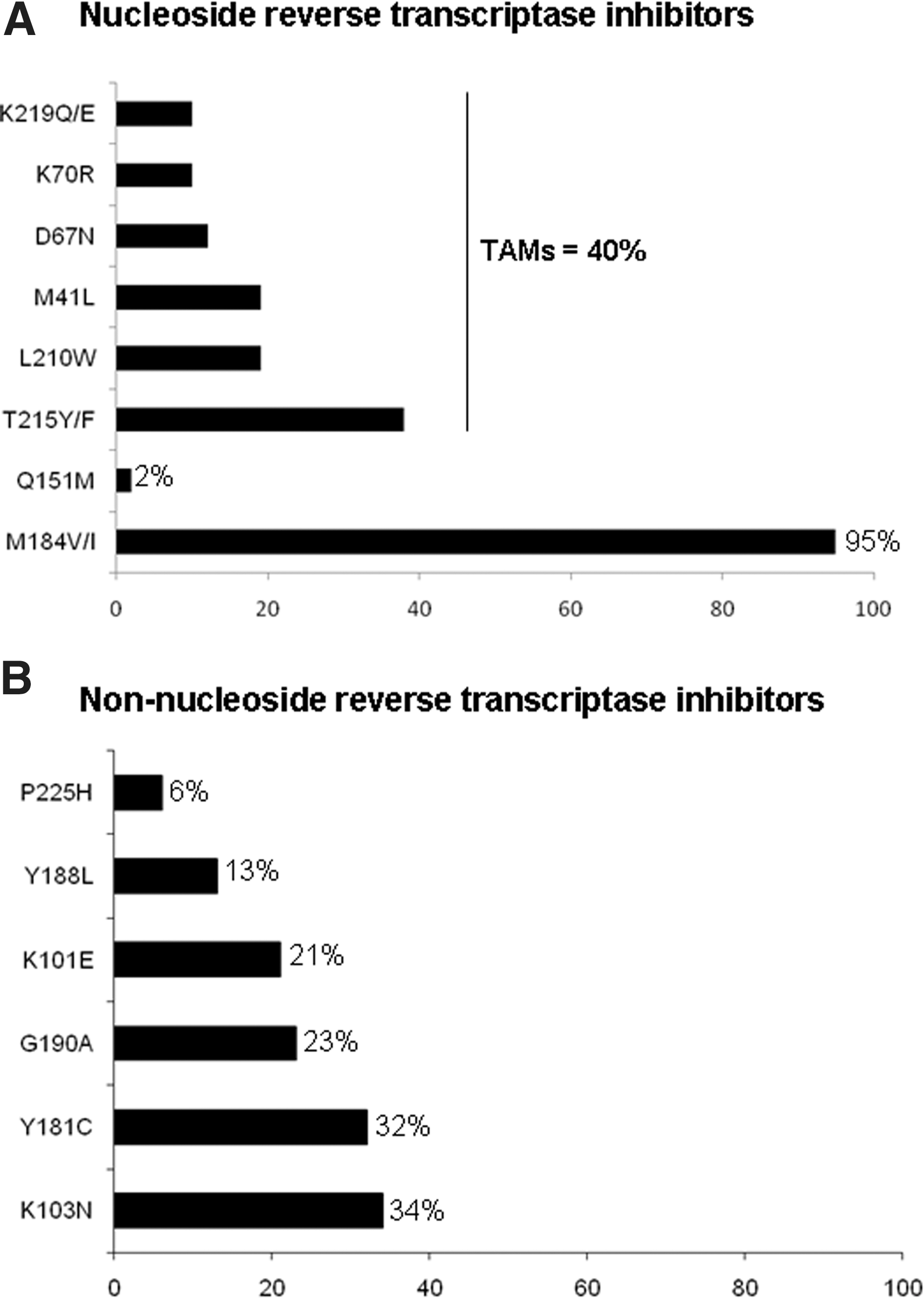
Percentages of resistance-associated mutations to nucleoside reverse transcriptase inhibitors
Multi-NRTI resistance was found in 18 children (43%) out of the 42 with viruses harboring NRTI resistance mutations. Among the 18 cases, the main profiles were as follows: M184V–T215Y/F in 15 (83%), M184V–T215Y/F–L210W in seven (39%), M184V–T215Y/F–M41L in six (33%), and M184V–T215Y/F–D67N in three (17%). The median duration on ART was 34 months (13–84 months).
Among the 42 children with NRTI-resistant viruses, 24 (57%) had a single resistance mutation. The main mutation was M184V/I found in 23 cases (96%). The median duration on ART was 27 months (7–59 months). Based on ART duration, no difference could be found between the group with multi-NRTI resistance and the one with a single resistance mutation (p>0.05).
NNRTI resistance mutations
At least one NNRTI resistance mutation was found in viral isolates from 47 (99%) of the 48 children with drug-resistant viruses. The pattern of NNRTI resistance mutations was as follows: K103N in 16 genotypes (34%), Y181C in 15 (32%), G190A in 11 (23%), and K101E in 10 (21%) (Fig. 2B). NNRTI resistance profiles were not different in children failing NVP compared to EFV.
Multi-NNRTI resistance was found in 27 children (57%) out of the 47 having viruses harboring NNRTI resistance mutations. Among those 27, the main patterns of mutations were K101E–G190A in eight (30%), K103N–Y181C in three (11%), and K101E–Y181C in three (11%). The median duration on ART was 29 months (7–84 months). Twenty children out of the 47 with NNRTI-resistant viruses had single resistance mutation. The main mutations were K103N in eight (40%), Y188L in five (25%), and Y181C in five (25%). The median duration on ART in these latter children was 24 months (11–79 months). No difference on ART duration could be found between the group with multi-NNRTI resistance and the one with a single resistance mutation.
Among the 48 study children with resistant viruses, eight children (17%) had viruses harboring both multi-NRTI and multi-NNRTI resistance mutations. The median duration on ART in these latter children was 34 months (18–84 months).
Considering the patterns of NRTI and NNRTI resistance mutations, no correlation could be found with therapy duration.
PI resistance mutations
No major mutations conferring PI resistance were detected.
HIV-1 genetic diversity
Phylogenetic analysis of the 52 genotyped viral isolates showed that CRF02_AG was most represented with 39 viral isolates (75%) (Fig. 3). Subtype C was found in three (6%) cases and CRF06_cpx was found in one child (2%). HIV-1 subtypes D and G were each found in one child (2%). Recombinant viruses were also found: CRF02_AG/A1 in two cases, CRF06_cpx/CRF02_AG in two cases, and A1/CRF02_AG, CRF02_AG/CRF09_cpx, and U/CRF14_BG in one child each. There was no relationship between resistance mutations patterns and HIV-1 subtypes.
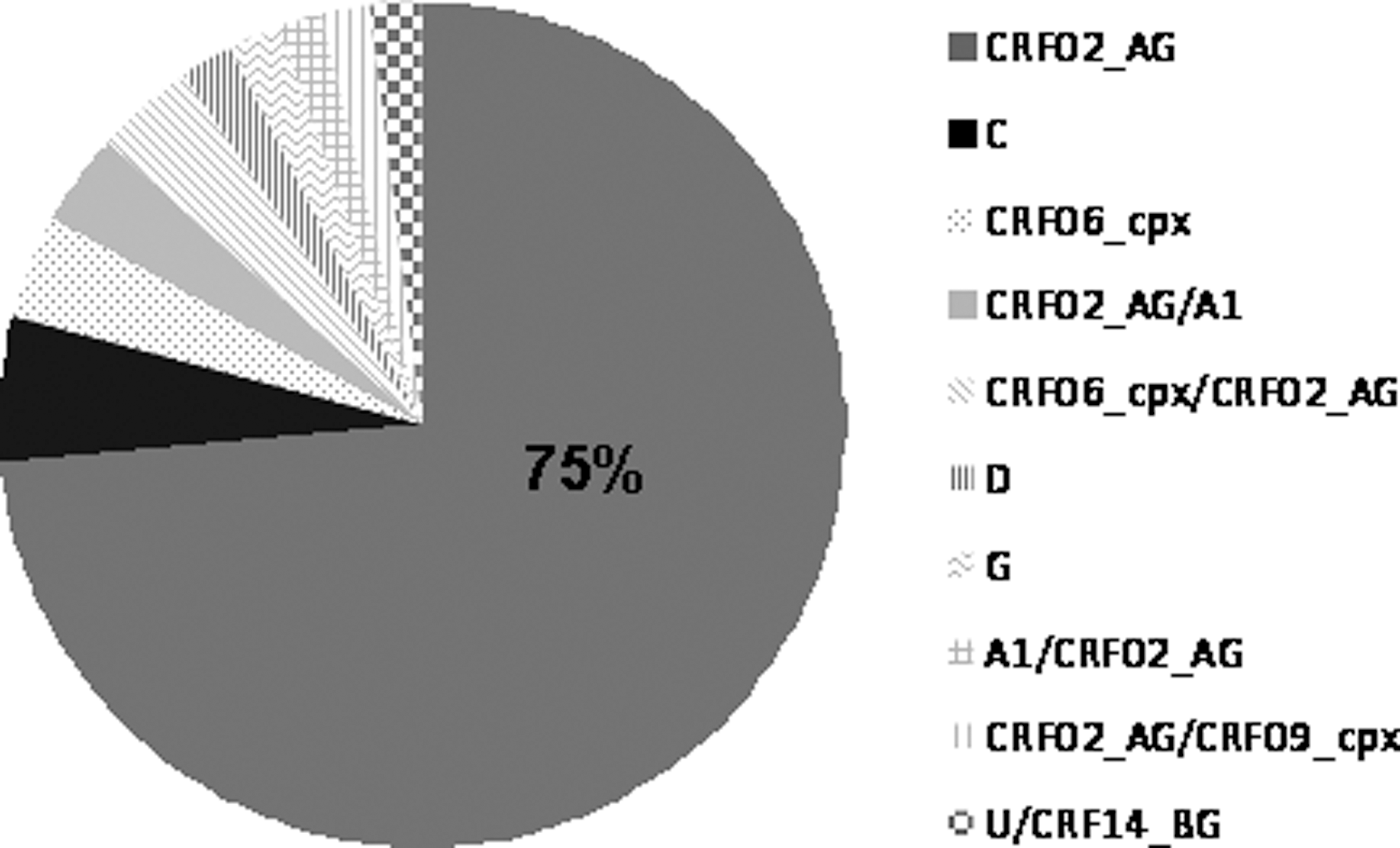
Distribution of HIV-1 subtypes and circulating recombinant forms among 52 HIV-1-infected children followed in Dakar, Senegal, treated by first-line antiretroviral drugs.
Interpretation of genotypic resistance tests and possible future therapeutic options
Genotypic resistance profiles were interpreted according to the Stanford University HIV drug resistance database for all drugs proposed for second-line regimens, according to the revised 2010 WHO recommendations.
Among the 48 sequenced viruses found in children in first-line regimen and harboring resistance mutations, 36 (75%), 38 (79%), and 39 (81%) remained susceptible to ABC, ddI, and tenofovir (TDF), respectively. These data show that the NRTI drugs recommended by the WHO for second-line regimens in Africa are expected to be active in the majority (≥75%) of children requiring therapeutic switch. Conversely, the use of first-generation NNRTIs appeared largely compromised in children taking first-line ART in VF, as 90% of them showed circulating viruses resistant to EFV and NVP. Moreover, resistance to etravirine (ETR), a newly available second-generation NNRTI, was observed in 10 viruses (21%), including an intermediate level of resistance in four, a low level in three, and a high level of resistance in three viruses. The PI drug class remained fully active in all children after first-line therapeutic failure.
Discussion
In the present series of Senegalese HIV-1-infected children, more than half of the children taking ART according to the WHO recommendations for resource-poor countries for 20 months in median were in VF according to the 2010 revised criteria. Furthermore, 92% of children in VF harbored resistant viruses, and 17% of them showed at least one major drug resistance mutation to NRTI or NNRTI after excluding the M184V mutation. The rate of VF in the present study children under first-line ART (56%) appears higher than those previously reported in Uganda (13–26%), 13,22 South Africa (16%), 23 Thailand (16%), 24 Mali (44%), 12 and Cambodia (19%), 25 but similar to that previously reported in children living in Bangui, Central African Republic after 6 months of ART. 10 These observations indicate that the risk of therapeutic failure in treated children is high, even in countries whose health care system and care of HIV-infected adults is associated with high rates of therapeutic success, such as Senegal. 16 Treatment of pediatric HIV infection remains difficult, mainly because the ART options are limited, the pediatric dosing of antiretroviral drugs is complicated, and adherence to treatment is challenging to achieve, so that complete suppression is rarely observed. 10 Taken together, these observations confirm that virological suppression and long-term ART success are more difficult to achieve in children than in adults. 26
Three study children whose viruses showed antiretroviral drug resistance mutations had plasma HIV-1 RNA load between 3.0 and 3.7 log10 copies/ml, thus demonstrating that therapeutic failure may be underdiagnosed with the current criteria of VF according to the 2010 revised WHO criteria (e.g., plasma HIV-1 RNA≥3.7 log10 copies/ml). 21 Whether persistent low levels of viral replication may be associated with therapeutic failure in children taking ART warrants further investigation. These findings indicate that maintaining first-line ARV treatment, despite a detectable viral load, is associated over time with an increased risk of increased plasma viral load and further VF, and also confirm and emphasize the need in antiretroviral-treated children to improve biological monitoring in order to diagnose VF as early as possible with the aim of preserving future therapeutic options.
The viruses isolated from the majority of antiretroviral drug-treated children in VF carried resistance mutations to NRTIs or NNRTIs. The high selection rates of TAMs and NNRTI resistance mutations in the present study children are likely associated with the prolonged duration of ART. Similar high prevalences of resistance mutations have been reported in children in VF living in other sub-Saharan African countries who were also infected with various non-B subtypes, including Ivory Coast (71%), 6 Central Africa Republic (77% 10 and 85%), 14 Mozambique (92%), 11 South Africa (98%), 27 Uganda (100%), 28 and Kenya (100%), 8 as well as in those living in developed countries where infection with subtype B predominates. 29 A high rate of drug resistance was also found in children in Thailand, where the main circulating form of HIV-1 is CRF01_AE. 30 In our series, the distribution of HIV-1 subtypes was similar to that previously reported in Senegalese adults, 16 with a predominance of the CRF02_AG subtype. Furthermore, no relationship between resistance mutations patterns and HIV-1 subtypes could be evidenced. Taken together, these findings confirm that the rate of antiretroviral drug resistance mutation selection does not appear to be influenced by viral genetic diversity, as previously observed. 6,31
The M184V/I mutation was the most commonly observed (95%) NRTI resistance mutation, most likely due to the systematic use of 3TC 32,33 in ART regimens recommended by the 2006 and 2010 revised WHO guidelines for pediatric AIDS in resource-poor regions. 17,21 According to the WHO guidelines, the presence of the M184V resistance mutation, which confers resistance to 3TC/emtricitabine (FTC), does not preclude further systematic use of 3TC/FTC in a second-line treatment. Furthermore, the systematic use of 3TC/FTC in second-line WHO-recommended regimens of ART is thought to be beneficial, because of decreased viral fitness of HIV-1 strains mutated at codon 184. 34,35 However, the effective in vivo impact of the M184V resistance mutation in children receiving second-line treatment should be further investigated in African pediatric cohorts. Furthermore, in adults infected with HIV-1 subtype B, the M184V mutation has been demonstrated to delay the emergence of TAMs, 36 –38 suggesting that it would remain advantageous to maintain 3TC-containing treatment even in patients with a detectable viral load. 36 In the present cohort, TAMs were found in more than one-third (40%) of children harboring NRTI-resistant viruses, most likely due to the large use of AZT in the pediatric first-line WHO-recommended regimen. 17,21 The relatively middle proportion (40%) of TAMs selection in study children in therapeutic failure may be in part explained by the high frequency of the M184V mutation, conferring increased sensitivity to AZT and d4T, thus contributing to the lower frequency of TAMs. 36,39 Whether the selection of TAMs in the present population of children mainly infected with non-B subtypes would have been hampered by the previous selection of the M184V mutation would need further investigation. Furthermore, the low rate of TAMs makes it possible to conserve sensitivity to TDF, whose resistance needs the accumulation of at least three TAMs. 40 Nearly all children (99%) infected with viruses carrying genotypic resistance mutations had viruses harboring resistance mutations to NNRTIs. This resistance pattern is most likely due to the wide use of NVP or EFV, two drugs with a low genetic barrier to resistance selection, 41,42 or to the previous selection of NNRTI resistance mutations in mothers receiving chemoprophylaxis to prevent mother-to-child transmission. 43 Finally, in the present series, the antiviral activity of antiretroviral drugs of the second-line regimens proposed by the 2010 revised WHO recommendations in case of VF was not largely impacted, with a predictive activity of ABC, ddI, and TDF in 75%, 79%, and 93% of cases, respectively.
Compliance to ART continues to remain a major concern of caring for HIV-infected children. 44 In the present study, the rate of treatment interruption was higher in treated children in VF than in those with undetectable plasma HIV-1 RNA load. Treatment interruption provides problems of adherence, which constitutes a crucial factor in the effectiveness of ART. Interestingly, some study children were in VF and showed circulating viruses harboring antiretroviral drug resistance mutations, despite the lack of treatment interruption, as assessed by pharmacy refill records. This observation suggests the possibility of an initial infection with primary resistant viruses. Indeed, drug resistance-associated mutations in untreated children have been reported in sub-Saharan African countries where single-dose NVP is widely used for preventing HIV mother-to-child transmission. 45,46 In addition, even with good pharmacy refill records, poor adherence at home may account for therapeutic failure.
Remarkably, wild-type viruses sensitive to all major antiretroviral drug classes were detected in 8% of children receiving first-line ART in VF (plasma viral load>3.7 log10 copies/ml). This finding is reminiscent of the 20% rate found in adult patients displaying VF associated with wild-type viruses, previously reported in Douala 47 and in Bangui. 14 VF associated with wild-type viruses is likely due to poor adherence, which needs urgent correction. Indeed, the level of adherence in antiretroviral drug-treated children was found to be inversely associated with HIV-1 RNA plasma level after 6 months of ART. 10 Virological monitoring appears to be a particular challenge in HIV-infected children who are known to have difficulties in maintaining good adherence. In addition to poor adherence, the toxicity of antiretroviral drugs may also make it necessary to opt for an alternative first-line or second-line regimen, as previously reported in 2% of antiretroviral drug-experienced children living in Malawi. 48
In the present series, 45 (94%) out of the 48 children with viruses carrying NNRTI resistance mutations needed a second-line, PI-based regimen, as both NVP and EFV could no longer be used. Based on results from genotypic resistance tests, interpreted by the Stanford University HIV drug resistance database, the activity of ETR may be compromised in about 21% of circulating HIV-1 strains, as previously reported in Bangui. 14 Such a prevalence of predicted ETR resistance appears much higher than rates (2.4–3.8%) previously reported in Western countries. 49,50 In the present series, primary resistance to ETR may reflect possible genetic specificity of HIV-1 non-B subtypes, 51 in addition to the long duration of viral replication under first-generation NNRTI drugs in Africa. However, at present ETR cannot be recommended in pediatric AIDS treatment, due to the lack of a pediatric formulation, and pharmacokinetic, efficacy, and safety data in children. Lopinavir boosted with ritonavir could still be used in a second-line regimen. Finally, two children had viruses harboring resistance mutations to all WHO-recommended NNRTIs and NRTIs. In these latter children, the second-line regimen would require antiretroviral drugs not yet available in Senegal.
In conclusion, a high prevalence of NRTI and NNRTI resistance mutations was observed in Senegalese children receiving NRTI- and NNRTI-based antiretroviral drug regimens recommended by the WHO and experiencing VF. This finding has important public health implications, and emphasizes the need to improve the distribution of antiretroviral drugs in order to prevent therapeutic interruption, to increase adherence in treated children, and to offer adequate HIV biological monitoring with early diagnosis of VF. Furthermore, it emphasizes the need to provide more options for second-line regimens in children under ART, especially in the context of resource-limited settings, where the availability of affordable antiretroviral drugs is limited.
Footnotes
Acknowledgments
We express our gratitude to the Senegalese Ministry of Health and the National AIDS and STIs Division. We also thank the Pr Annemie Vandamme for her assistance. The study was supported by the Senegal's National AIDS Program and the Chain project.
Author Disclosure Statement
No competing financial interests exist.