
Abstract
HIV genetic diversity may have an impact on viral pathogenesis, transmission, response to treatment, and vaccine development. Public health surveillance that monitors the frequency and variety of HIV subtypes in a particular region or patient group is vital to successfully control the pandemic. We present the first comprehensive report on HIV diversity in Ireland. This study comprised all new HIV-1 diagnoses that were confirmed in the National Virus Reference Laboratory, University College Dublin, from January 2004 to December 2008. HIV 1 protease and reverse transcriptase sequences were generated using the Siemens Trugene HIV 1 Genotyping System. Subtypes were determined using web-based genotyping tools. There were 1579 new diagnoses [615 (39%) female and 964 (61%) male], of which 1060 had HIV-1 RNA specimens available for sequencing. Of sequenced samples, HIV-1 subtype B accounted for 50% overall, decreasing from 55.1% in 2004 to 49.5% in 2008. In addition, subtype B accounted for more than 80% of Irish-born individuals and more than 90% of Irish-born injection drug users and men who have sex with men. Subtype C was the second most prevalent in the overall cohort, accounting for 25%, although it accounted for only 6.1% of Irish-born individuals, with no evidence of in country transmission. The prevalence of non-subtype B HIV-1 infection in Ireland is increasing. However, these appear primarily to be imported infections not yet circulating within traditional Irish risk groups. Enhanced HIV-1 molecular epidemiology surveillance is required to monitor the spread of HIV-1, to inform future public health policy, and to ultimately control the HIV-1 epidemic in Ireland.
Introduction
The different HIV-1 subtypes and circulating recombinant forms (CRF) are distributed globally in a nonuniform manner. 1 For this reason, it is important to monitor the global spread of HIV subtypes and CRF in a timely manner, and while the World Health Organization (WHO) addresses this task through a large global network of research laboratories that specialize in the characterization of HIV samples from diverse geographic regions, each country also bears a responsibility to monitor the epidemic within its own boundaries.
In Ireland during 2008, there were 405 newly diagnosed HIV infections reported to the Irish Health Protection Surveillance Centre (HPSC), 2 bringing the total number of HIV infections reported in Ireland to the end of December 2008 to 5243. Of the 405 newly diagnosed cases, completed (voluntary) enhanced surveillance forms were received for 322 (79.5%) individuals: the mode of acquisition of infection (where available) was heterosexual transmission (HT) in 178 individuals, sex between men (MSM) in 97, injection drug use in 36, and vertical (mother to child transmission, MTCT) in 7. Of the newly diagnosed cases where geographic origin (place of birth) was known 123 were born in Ireland, 121 in sub-Saharan Africa, 28 in Western Europe, and 17 in central Europe. While demographic data are important and useful from an epidemiological and public health perspective, equally important, if not more so, is the information provided by the virus itself, e.g., subtype, origin of infection, and probable mode of acquisition. However, at present, virological data are not collected as part of the enhanced surveillance program.
The primary aim therefore of this study was to characterize for the first time the molecular epidemiology of HIV-1 in Ireland as reflected in newly diagnosed HIV-1-infected individuals over a 5-year period (2004–2008). Further to this aim, a phylogenetic analysis was performed on the collected data to determine whether MSM and IDU in Ireland constitute a single HIV-1 subtype B epidemic, and whether any of the non-B subtypes of HIV has become endemic in the Irish-born HIV-infected population.
Materials and Methods
Study duration and design
The study focuses on patients diagnosed with HIV infection in Ireland from January 2004 to December 2008 inclusive. Data collection for the first three and a half years of the period studied was retrospective, with data for the final one and a half years being gathered prospectively.
Data collection
Study data were collated in the National Virus Reference Laboratory (NVRL) University College Dublin (UCD), the primary center in Ireland for the serological diagnosis and/or confirmation of HIV-1 infection. In addition, the NVRL performs 85–90% of HIV-1 RNA (viral load) testing for Ireland and all HIV-1 genotypic antiretroviral resistance testing (GART) for HIV-1-infected individuals. All analysis was performed on GART data that were anonymized following linkage with limited demographic data, i.e., ethnicity and mode of acquisition of infection.
Patient selection
Subjects eligible for inclusion in the study comprised all patients newly diagnosed with HIV infection in Ireland from January 2004 through December 2008. The date of diagnosis for each patient was taken as the first date upon which a blood sample from that patient (plasma or serum) tested positive for either HIV-specific antibody or HIV 1 RNA in the NVRL. One caveat to these criteria is that the infection had to be subsequently confirmed on further testing of a subsequent sample taken on a different date. Newly diagnosed patients were identified primarily through the six public HIV/infectious disease (ID) services provided around the country, although some patients would first be diagnosed elsewhere: (1) national antenatal screening program (in place since 1999), (2) specialist health clinics targeting particular at-risk groups, e.g., MSM, for HIV infection, (3) drug treatment centers offer screening for HIV infection to their clients, (4) all those presenting to donate blood, and (5) some patients will be diagnosed by their own primary care physician when presenting for a routine health check or on account of a high-risk exposure.
HIV-1 branched DNA testing
HIV-1 (RNA) viral load measurement was performed using the Siemens VERSANT HIV-1 RNA 3.0 Assay (bDNA) as per the manufacturer's instructions.
Genotypic antiretroviral resistance testing
HIV-1 genotypic resistance testing was performed using the Siemens TRUGENE HIV-1 Genotyping Kit and the OpenGene DNA Sequencing System as per the manufacturer's instructions.
GART-based HIV subtyping
HIV subtyping was performed by submitting GART sequences to three well-established online web-based genotyping tools: three tools were chosen to ensure consensus. These were the Stanford University HIV Drug Resistance database (
Phylogenetic analysis
Phylogenetic analysis was performed using the sequences of the protease (nucleotide position 2267–2548) and reverse transcriptase (nucleotide position 2666–3279) regions of the HIV pol gene obtained from the GART as described above. Concatenated sequences were aligned with WHO HIV reference sequences using Bioedit v7.0.9. Neighbor-joining trees were constructed and analyzed using PAUP* v4.0b10 and Figtree v1.2, respectively. Bootstrapping resampling was carried out for 1000 replicates of the data set. Protease and reverse transcriptase sequences were submitted separately to GenBank (accession numbers JN622218–JN623041).
Statistical analysis
Differences in mean HIV-1 viral load data were analyzed using the Student's t-test, while significance in changes in proportions over time was determined using the chi-squared test. Both applications were performed in Microsoft EXCEL.
Results
New diagnoses 2004 to 2008
Over the course of the 5-year study period, there were 1579 new diagnoses identified, 615 (39%) female (F) and 964 (61%) male (M). The yearly totals were 305 (132F/173M=43.3%/56.7%) in 2004, 298 (123/175=41.3/58.7) in 2005, 321 (124/197=38.6/61.4) in 2006, 297 (113/184=38/62) in 2007, and 358 (123/235=34.4/65.6) in 2008. These data include one diagnosis of HIV-2 infection in 2005. The mean age at diagnosis for the entire cohort (N=1579) was 33.9 years, although the mean age for females (31 years) was 4.8 years less than that for males (35.8).
HIV viral load
HIV viral load was available for 1384 (85.2%) new diagnoses. Mean HIV viral loads (MVL) were compared by gender, by mode of acquisition of infection, and by subtype. The overall MVL for females [4.77 log10copies/ml (l cm)] was significantly lower than that for males (5.05 l m) (p<0.001) (Table 1). However, this was the result of a significant MVL gender difference for subtypes C (p<0.001) and CRF02_AG (p=0.02) only: no gender difference was observed for subtypes A (p=0.59), B (p=0.45), G (p=0.32), or CRF01_AE (p=0.89).
HIV Viral Load Analysis
MVL, mean viral load; LCM, log copies per ml; ANS, antenatal screening.
There was no difference in MVL between those individuals who had acquired HIV through injection drug use (IDU) (5.14 l cm) or through male homosexual encounters (MSM) (5.12l cm) (p=0.64) (Table 1). However, MVL in the heterosexually transmitted (HT) HIV group was significantly lower (4.92l cm) than that of IDU and MSM (both p values <0.001). Of note, within the HT group, males had an MVL (5.09l cm) that was no different in magnitude from that of IDU (p=0.32) and MSM (p=0.56). Conversely, HT-infected females had a significantly lower MVL (4.73l cm) than IDU, MSM, and HT-infected males (p<0.001) (attributable in the main to subtype C and CRF02_AG virus infections). Furthermore, in HT-infected females diagnosed through antenatal screening (N=63), MVL was lower still at 4.45l cm. This gender difference in MVL was not evident in IDU-infected individuals (p=0.74), the majority of whom were infected with subtype B virus.
HIV-1 subtype B had the highest MVL of those measured at 5.16l cm (N=523) followed by CRF02_AG at 5.1 (N=56), CRF01_AE at 4.94 (N=28), subtype G at 4.85 (N=34), C at 4.76 (N=258), and A at 4.74 (N=31). No other subtype was sufficiently represented to generate meaningful data. MVL for subtypes A (p=0.004), C (p<0.001), and G (p=0.012) were significantly lower than subtype B, but there was no significant difference between the MVL for subtype B and that of CRF02_AG (p=0.4) or CRF01_AE (p=0.07) (Table 1). On analysis of subtype MVL data by gender, significant differences existed within males (p=0.002) and females (p<0.001) between subtype B and subtype C only. In males, there was a trend toward a significant difference between subtype B and G (p=0.06), and in females, between subtype B and A (p=0.07). There were insufficient numbers of IDU and MSM infected with non-B subtypes to examine subtype-specific MVL associations in these cohorts.
HIV sequence data
Of the 1579 new diagnoses, sequencing of the reverse transcriptase (RT) and protease (PR) regions of the HIV RNA pol gene (for the purpose of genotypic antiretroviral resistance testing or GART) was performed on 1060 (67.1%) specimens, comprising 392 (37%) females and 668 (63%) males. Of those 519 patients for whom RNA sequences were not available, 195 (37.5%) had no specimen taken for viral load testing, 150 (28.9%) had viral loads of <1000 copies per ml, and were therefore not sequenced, and 174 (33.5%) were viremic >1000 copies per ml, but GART was not requested. Of note, retrospective requests for GART, which fell outside the study period, were not included in the study.
The absolute number (and percentage) of newly diagnosed individuals from whom HIV RNA was sequenced ranged over the 5-year study period from 158 (of 305, or 51.8%) in 2004, to 199 (of 298, or 66.8%) in 2005, 225 (of 321, or 70%) in 2006, 203 (of 297, or 68.4%) in 2007, and 275 (of 358, or 76.8%) in 2008. Of 1060 sequenced samples, HIV subtype B accounted for 548 (51.7%). However, the prevalence of subtype B as a proportion of all newly diagnosed infections decreased from 87/158 (55.1%) in 2004 to 136/275 (49.5%) in 2008. Subtype C was the second most prevalent subtype in the study cohort, accounting for 273 (25.8%) of the 1060 individuals from whom HIV was sequenced, followed by 59 CRF02_AG (5.6%), 36 subtype G (3.4%), 35 CRF01_AE (3.3%), 33 subtype A [3.1% (32 A1 and 1 A2)], 15 CRF06_CPX (1.4%), 11 subtype D (1%), 7 subtype F [0.6% (all F1)], 4 CRF14_BG (0.4%), and 1 each of CRF18_CPX and subtype H; 37 sequences were unassigned. It is evident that the majority of HIV diversity seen in the total patient cohort is in fact attributable to newly diagnosed females: subtype B accounted for 446 of 668 (66.8%) new diagnoses in males, compared with just 102 of 392 (26%) in females. In contrast, subtype C accounted for 96 of 668 (14.4%) new diagnoses in males, compared with 177 of 392 (45.2%) in females.
HIV subtype diversity by patient ethnicity and mode of acquisition of infection
HIV subtypes have a characteristic global distribution. 3 Thus, non-subtype B infections in Ireland may reflect (1) imported infections through immigration of non-Irish-born individuals infected overseas, (2) overseas acquisition of HIV by Irish-born individuals, or (3) existing (as yet undocumented) endemicity within Irish-born HIV-infected cohorts. To determine which of these is most probable, subtype data were correlated with patient ethnicity (PE). PE data, as reflected by country (or region) of birth, were available for 887 individuals. The majority of non-subtype B infections (311 of 420, or 74%) diagnosed over the study period occurred in individuals born outside of Ireland, and therefore were most probably imported; in contrast, 378 of 467 (80.9%) of individuals diagnosed with HIV subtype B infection were born in Ireland. This is in keeping with the traditional image of Western Europe as a region in which subtype B predominates. 3
HIV is mainly transmitted through IDU, HT, and MSM sex, vertically from MTCT, or (now rarely) via infected blood transfusion (BT). 4 In the present study, the probable mode of HIV acquisition was available for 887 individuals. However, for 23 patients, the mode of acquisition of HIV (MOA) could not be definitively ascertained (more than one risk factor), and 22 were infected via MTCT (N=18) or BT (N=4). For clarity, therefore, the remainder of this analysis will focus on the three main risk groups (HT, IDU, and MSM: N=842) (Table 2a and b).
Irish Born Newly Diagnosed HIV Infections in Ireland 2004–2008 by Year of Diagnosis, Gender, Infecting Subtype, and Mode of Acquisition of Infection (N=430)
HT, heterosexual transmission; IDU, injection drug use; MSM, men who have sex with men.
Non-Irish-Born Newly Diagnosed HIV Infections in Ireland 2004–2008 by Year of Diagnosis, Gender, Infecting Subtype, and Mode of Acquisition of Infection (N=412)
The composition of newly diagnosed HIV-1 in Ireland has changed significantly over the study period (p=0.025): there has been a significant decrease in the proportion of IDU-related infections (p=0.015) and there has been an increase in MSM transmission, although this did not attain significance (p=0.07). Conversely, there has been no significant change in the proportion of HT infections over the study period (p=0.47). Different HIV subtypes predominate in the different mode of acquisition cohorts (Fig. 1): 186 of 197 (94.4%) infections in IDU and 195 of 216 (90.3%) infections in MSM are caused by HIV subtype B; indeed, no other subtype is responsible for more than five infections in total [CRF01_AE caused 5 of 216 (2.3%) infections in MSM]. In contrast, in the HT group, a far greater diversity is observed.
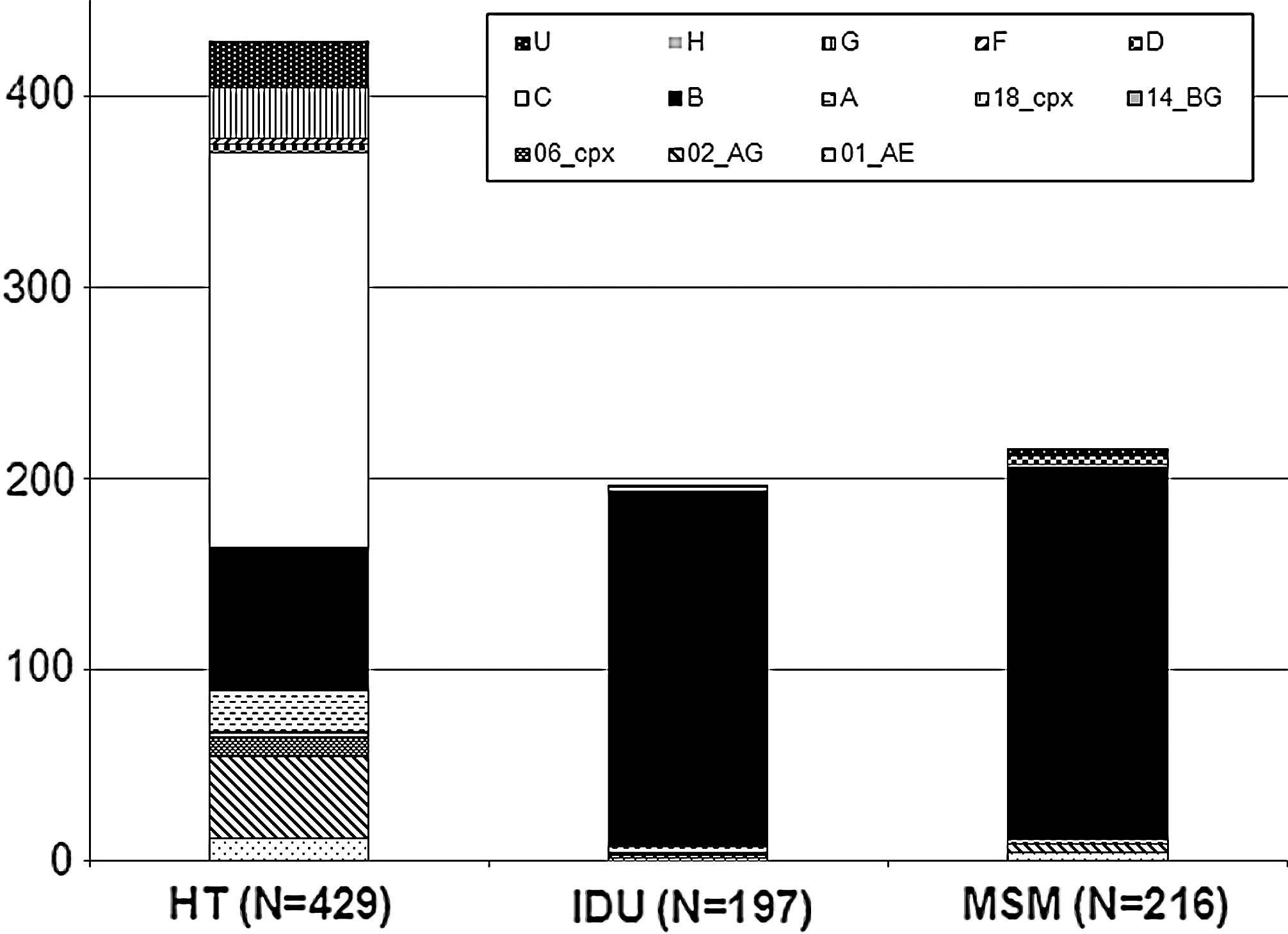
Of these 842 individuals, 430 (102F: 328M) were Irish born: 101 HT, 181 IDU, and 148 MSM. Taking MOA in conjunction with PE, the proportion of IDU in Irish-born individuals decreased significantly (p=0.005) over the course of the study period; there was a trend toward an increased proportion of MSM (p=0.07), with no change in the proportion of new diagnoses attributed to HT infection (p=0.52). In Irish-born HIV-infected individuals, 178 of 181 (98.3%) IDU and 139 of 148 (93.9%) MSM infections were caused by subtype B, suggesting non-B subtypes are not yet established in Irish-born MSM and IDU (Table 2a).
The non-Irish born cohort (N=412) was evenly divided between females (N=203) and males (N=209), comprising predominantly HT infections [N=328 (79.6%)] with 68 MSM and 16 IDU. In contrast to the Irish-born cohort, subtype C accounts for the majority of infections in the non-Irish-born cohort, with 199 (48.3%): this is followed by subtype B with 77 (18.7%), CRF02_AG with 40 (9.7%), subtype G with 24 (5.8%), and subtype A with 23 (5.6%) infections (Table 2b). This subtype prevalence is similar in both males and females in the HT groups. Conversely, the majority of infections in non-Irish-born MSM (46 of 68, or 67.6%) and IDU (9 of 16, or 56.3%) are subtype B, raising the possibility that these individuals may have acquired HIV in Ireland or other Western communities.
Phylogenetic analysis of newly diagnosed HIV-1 infections in Ireland 2004–2008
It has been demonstrated that pol gene sequences obtained during routine clinical practice can be used for the reconstruction of transmission events, and the phylogenetic surveillance of HIV-1 genetic diversity. 5,6 To assess the usefulness of the sequences obtained from our cohort, the following questions were addressed: (1) Do MSM and IDU in Ireland constitute a single HIV-1 subtype B epidemic; and (2) Has any of the non-B subtypes of HIV become endemic in the Irish-born newly diagnosed HIV-infected population? (For the purpose of this study, endemicity has been defined as a prevalence of >2.5%, as per Taylor and colleagues. 1 )
1. Of 165 of 183 IDU sequences clustered in the yellow-shaded region of the subtype B tree (Fig. 2a), only three sequences were from MSM. In contrast, the nonshaded portion of the tree comprises predominantly MSM (N=191, colored in red), small numbers of heterosexually transmitted infections, and IDU (N=18). These data suggest IDU and MSM may constitute separate HIV-1(B) subepidemics. This may be the result of a single virus introduced into Ireland in the 1980s evolving at different rates in separate cohorts or, alternatively, two separate subtype B viruses may have been imported into the different risk groups in Ireland at the outset.
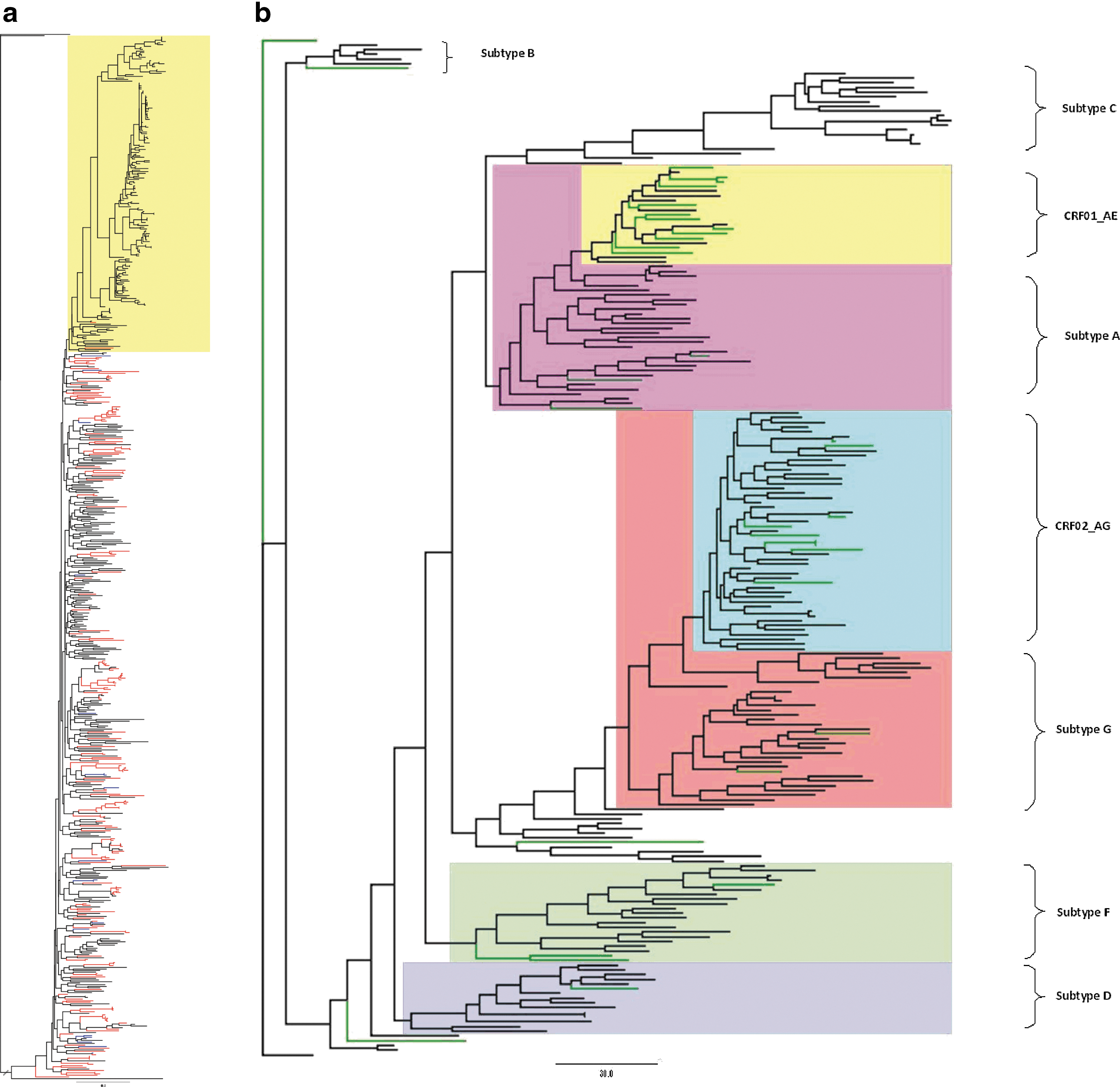
2. The non-B, non-C tree suggests that in-country transmission of CRF01_AE [prevalence of 3.1% (14/445) over the study period] may be occurring (Fig. 2b). Of these 14 individuals, sequences from 12 were suitable for phylogenetic analysis: 2 female and 10 male. The two females and six males were infected through HT: three were MSM and one was IDU. Four patients were diagnosed in 2008, one in 2007, three in 2006 and 2005, and one in 2004: further epidemiological analysis was not feasible within the context of this study. In contrast, there was no phylogenetic evidence for in-country transmission of subtype C (data not shown), despite a prevalence of 6.1% (27/445) in Irish-born individuals over the study period. However, as sequence data were available for only 1060 (67.1%) of the present cohort, and PE data were available for only 887 of these, in-country transmission of subtype C cannot be definitively excluded on the basis of these results. Indeed, these inconclusive data argue for the inclusion of HIV subtype data in the national enhanced surveillance program.
Discussion
According to the WHO/UNAIDS Global HIV-1 survey of 2004, 88% (range 39–92%) of HIV-1 infections in Western Europe were caused by subtype B, with the remainder caused by subtypes A, C, G, and CRF01_AG. 7 This was in marked contrast to Eastern Europe, where 79% of infections were caused by subtype A, and only 15% by subtype B. In combination, both of these WHO regions probably account for only 5% of the global HIV-1 pandemic, yet neither accurately reflects the same molecular epidemiology, which sees subtype C accounting for some 50% of infections worldwide, with the greatest diversity and prevalence of recombinants seen in central Africa. It is this feature of the HIV-1 pandemic––its capacity for regional variation––that mandates each country to perform surveillance within its own borders, assuming it possesses that capacity. However, to date, no such program has been undertaken in Ireland. The 1060 subtyped specimens presented here constitute 67% of 1579 new diagnoses made within the study period, and some 33% of all HIV diagnoses (N=3186) made in Ireland from 2000 (when HIV case based reporting was introduced) through December 2008. These data should be used to inform public health policy and HIV infection prevention strategies in Ireland.
The gender breakdown in the present study was 60% male and 40% female with an increase in the proportion of males to 62% and 65% in 2007 and 2008, respectively. This recent increase is predominantly attributable to an increase in the number of MSM infections. The mean age for females in the present study was almost 5 years younger than that for males. It is probable that the reason for this difference in age profile lies in the inclusion of HIV antibody testing in the antenatal screening program, which obviously preferentially identifies infections in women. Screening strategies targeting other risk groups, e.g., young heterosexual men, MSM, and nonpregnant women, are therefore indicated.
Viral load
MVL in the HT acquisition group was significantly lower when compared with IDU and MSM. However, this difference was due almost entirely to (subtype C and CRF02_AG) HT-infected females, who also had a significantly lower MVL than their respective (C and CRF02_AG) HT-infected male counterparts. While lower HIV viral loads have been previously reported in women, in the context of the present study, this finding probably reflects the diagnosis of healthier women as a result of the national antenatal screening program. That said, as CD4 data were not available for this study, we cannot be certain this is the case.
Overall MVL for subtypes A, C, and G was significantly lower than subtype B, while there was no significant difference between subtype B and CRF02_AG, or CRF01_AE. Only the difference between subtype B and subtype C remained significant when measured in males and females separately. However, it should be noted that the numbers available for this analysis in non-B, non-C subtypes were small. While previous studies of subtypes A, C, and D have detected no significant intersubtype differences in viral load, 8,9 a finding in keeping with the data presented here, more recent reports do suggest higher viral loads in subtype D infection when compared with subtype A. 10 Also in contrast to the present data, CRF01_AE has previously been reported to be associated with higher viral loads than subtype B. 11,12 Of note, there was no change in the overall MVL by year over the 5-year study period. As the study focused on newly diagnosed ART-naive individuals, this is not surprising, and indeed provides some independent validation of the patient selection methodology.
Mode of acquisition of HIV
There was no significant change in the proportion of HT infections over the study period: conversely, the proportion of IDU infections significantly decreased. However, of greater concern is that fact that the number of infections in MSM both in absolute terms and as a proportion of all infections increased over the study period. These data indicate that although HIV in Ireland is no longer confined solely to the traditional Irish HIV risk groups (IDU and MSM) it is in MSM that the greatest number (relatively) of new infections is being seen. These findings are in keeping with previous reports from other jurisdictions. 13,14
HIV-1 subtype diversity
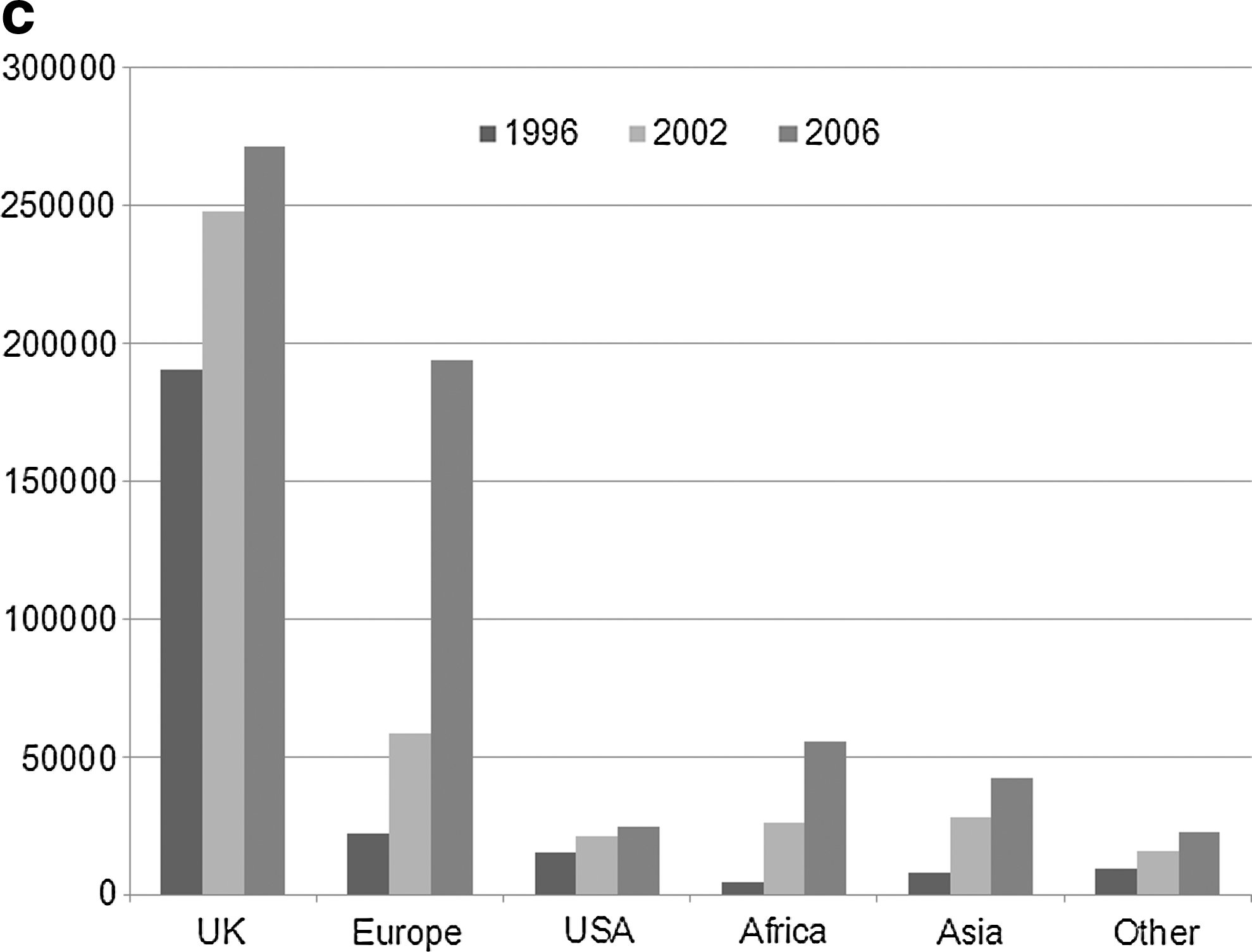
The prevalence of non-B HIV-1 infection in Ireland is increasing (Table 2). However, a more relevant question is whether non-B subtypes have become endemic in Irish-born individuals. Convincingly, the data demonstrated that this is not yet the case, with subtype B still accounting for 84.9% of HIV infections in Irish-born individuals, 94.4% of infections in IDU, and 90.3% of infections in MSM. In fact, the number of new infections in these three groups each year as a result of any other subtype is in single digits, suggesting the majority of non-B infections are acquired through exposure to individuals originating in endemic areas; whether transmission is occurring in Ireland or overseas, however, cannot be ascertained based on the available data. Nevertheless, as 50% of all new infections in Ireland are now non-B subtypes or CRFs, ongoing surveillance is recommended to determine whether this situation changes in the years ahead, as non-B subtypes have a demonstrated capacity to supplant subtype B infections. 15 The increase in non-B infections may be explained by reviewing Irish immigration patterns for the decade from 1996 to 2006 (Fig. 2c).
Phylogenetic analysis of newly diagnosed HIV-1 infections in Ireland 2004-2008
To date there has been no comprehensive study of the dynamics of HIV-1 transmission in Ireland: the available surveillance information identifies who is infected but not how or where. Thus, though not comprehensive, the sequence data presented here constitute the first step in combining virological data with demographic data to characterize the true nature of HIV-1 in Ireland. These data suggest the two primary traditional risk groups for HIV infection in Ireland may constitute separate subepidemics (Fig. 2a). Determining why this should be the case in a country with such a small HIV-infected population requires further study. It may be the result of a single virus introduced into Ireland in the 1980s evolving at different rates in predominantly separate cohorts; alternatively, separate subtype B viruses may have been imported into the different risk groups in Ireland at the outset; or there may be specific (host or viral) characteristics that make one virus strain particularly successful in a particular transmission group. It is also possible that there was a far greater degree of cross-infection between these two risk groups in previous decades than is evident in the virus sequences studied in the present cohort.
While it has been generally accepted that HIV-1 subtypes are different, the reason this should be the case, and the clinical significance of this has not been entirely clarified. 16 Nevertheless, there is a significant body of evidence now to suggest that viral subtypes differ with respect to coreceptor usage, transmissibility, disease progression, response to antiretroviral therapy, and development of antiretroviral drug resistance. 17 –30 Consequently, both national and regional genotypic surveillance––of the type presented here––is necessary to monitor the evolution of the global HIV pandemic. Though there are limitations to the present study, as evidenced primarily by the shortfall between the total number of new diagnoses and those that were sequenced, it still represents the first comprehensive attempt to describe the molecular epidemiology of HIV in Ireland, albeit for a single 5-year period. Nevertheless, the demographic composition of the subcohort (N=1060) accurately reflects that of the total cohort (N=1575), in respect to male:female prevalence rates [63:37(%) and 61:39(%), respectively], mean ages (34 and 33.9 years, respectively), and probable MOA for HIV [IDU (32 versus 33%), HT (both 42%), and MSM (26 versus 25%)].
Conclusions
The number of newly diagnosed HIV-1 infections in Ireland each year has increased from 2004 to 2008 with the majority in persons that were not born in Ireland. Furthermore, some 50% of newly diagnosed individuals in Ireland are now infected with non-B subtypes. That said, the majority of Irish-born individuals, IDU, and MSM are infected with HIV-1 subtype B. Consequently, it appears that non-B subtypes of HIV-1 are not yet circulating in Irish-born individuals. Irish-born IDU and MSM, despite both being predominantly infected with subtype B virus, appear to constitute two separate subepidemics with minimal evidence for cross-infection. Enhanced surveillance data gathered from persons newly diagnosed with HIV-1 infection should include HIV-1 RNA level (viral load) and HIV-1 subtype to inform national public health policy to definitively track and ultimately reduce or eradicate the transmission and spread of HIV-1 within Ireland.
Sequence Data
GenBank accession numbers are JN622218–JN623041.
Footnotes
Acknowledgments
The authors would like to thank Mary Codd and the Dublin HIV Cohort for the provision of additional demographic data.
Author Disclosure Statement
No competing financial interests exist.