
Abstract
The long-term impact of pegylated-interferon plus ribavirin (Peg-IFN-RBV) treatment outcome on CD4 T cell course in patients coinfected with human immunodeficiency virus (HIV) and hepatitis C virus (HCV) is unknown. The aim of this study was to investigate the impact of HCV-RNA clearance by standard anti-HCV therapy on long-term CD4 cells recovery in HIV/HCV patients on successful combined antiretroviral therapy (cART). We retrospectively enrolled HIV/HCV-coinfected patients on stable cART, treated with Peg-IFN-RBV between 2005 and 2009. CD4+ T cell counts were registered at baseline (pre-Peg-IFN-RBV), after 6, 12, and 24 months of follow-up from therapy discontinuation. Multiple linear regression analysis was performed to identify independent predictors of CD4+ T cell change following the anti-HCV treatment outcome. Of the 116 patients enrolled, 54 (46.6%) reached a sustained virological response (SVR) and 62 (53.4%) did not. Throughout a median follow-up of 24 months, the SVR group showed a mean annual increase in CD4+ T cell from baseline of 84 cells/μl at 1 year and of a further 38 cells/μl within the second year (p=0.01, 0.001, respectively). A nonsignificant mean increase of 77 cells/μl occurred in the non-SVR group within month 24 (p=0.06). Variables associated with greater CD4 gains were higher nadir and lower pre-interferon CD4 counts, and lower body mass index (BMI). The achievement of SVR was not significantly associated with the change in CD4+ count. The clearance of HCV replication did not affect the CD4+ changes after Peg-IFN-RBV therapy in coinfected patients on efficient cART. Liver fibrosis and higher BMI were negative determinants of immune recovery.
The effect of HCV coinfection on CD4 T cell recovery after the introduction of an effective combined antiretroviral therapy (cART) remains controversial. 1 –9 Recently, the Eurosida cohort study group showed that HCV viremia did not influence the CD4 recovery in HIV-infected patients on cART with persistently suppressed HIV replication. 10 Regardless of data concerning the CD4 cell course during and after pegylated interferon plus ribavirin (Peg-IFN-RBV) in HIV/HCV-coinfected patients that demonstrated a CD4 cell count fall within week 24 of treatment and their return to baseline values 24 weeks after therapy suspension, 11,12 the CD4 cell evolution on longer observation periods is unknown. As the extended effect of HCV viral clearance on the CD4 T cell course in HIV/HCV-coinfected sustained responders has never been evaluated, we aimed to assess the impact of Peg-IFN plus RBV-based HCV treatment outcome (sustained virological response versus nonsustained virologic response) on the long-term CD4 cell change in HIV/HCV-coinfected patients on long-lasting cART and stable HIV viral suppression.
This retrospective study enrolled HIV/HCV-coinfected patients treated with Peg-IFN-RBV (pegylated interferon α-2a 180 μg/kg/week or pegylated interferon α-2b 1.5 μg/kg/week plus ribavirin 1000–1200 mg/day according to body weight) between 2005 and 2009. The treatment period for Peg-IFN-RBV was 48 weeks for genotype 1 and 24 weeks otherwise. Eligible patients were HIV-infected subjects on stable cART with plasma HIV-RNA <50 cp/ml for at least 12 months, positive HCV-RNA (COBAS AmpliPrep, Roche Diagnostics, Indianapolis, IN), and elevated serum transaminases. Pre-IFN (within 3 months) measurements of plasma HCV-RNA (Versant HCV-RNA 3.0, bDNA; Siemens Medical Solutions, Berkeley, CA), HCV genotype, plasma HIV-RNA, CD4 cell count and percentage (CD4%), serum aminotransferases, and platelet count were registered. We also calculated in all the patients the Fib-4 index [age (years)×aspartate aminotransferase (AST; IU/liter)]/[platelet count (109/liter)×ALT (IU/liter)1/2], 13 a model for the noninvasive assessment of liver fibrosis in HCV-infected patients.
CD4 cell count and HIV-RNA measurement should be available at least every 6 months until the end of follow-up and any change of cART was registered. Sustained virological response (SVR) was defined by HCV-RNA PCR undetectability 6 months after IFN discontinuation; non-SVR was defined by HCV active replication at the same time, independently of the reason (primary nonresponse, relapse, therapy discontinuation). CD4 T cell modification was calculated as the mean change in CD4+ T cell counts from pre-IFN-treatment values and was evaluated after 6 (anti-HCV definition of response), 12, and 24 months following IFN-based therapy discontinuation; plasma HIV-RNA was registered at the same time points.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethic Committee.
Changes from baseline in CD4 counts and percentage (CD4%) were analyzed using a linear regression model for repeated measurements. The analysis was performed using PROC MIXED (SAS 9.2) to reduce the impact of missing data. Tests were two-sided and a p value less than 0.05 was considered statistically significant.
Multivariate linear regression analysis was performed to evaluate predictor factors for CD4 absolute count and CD4% changes during 24 months of follow-up. The parameters analyzed were age, body mass index (BMI), injecting drug use as transmission category for HIV infection, pre-IFN CD4+ cell count, nadir of CD4 T cell, duration of the exposure to cART, and current cART, Fib-4 fibrosis index.
Baseline patients characteristics are summarized in Table 1. One hundred and sixteen patients met the inclusion criteria. Overall, 54 patients (46.6%) reached an SVR and 62 (53.4%) did not. No significant differences emerged between sustained responders and non-SVR with respect to gender, intravenous drug addiction as a route of HIV transmission, cART regimen, and clinical or laboratory characteristics, except for higher ALT values at baseline in the former group and older age and higher percentage of genotype 1 infection in the latter. The Fib-4 index was consistent with bridging fibrosis/cirrhosis (index >3.25) in 20 patients (17.24%): 7/54 (12.96%) in the SVR group and 13/62 (20.96%) in the non-SVR group (data not shown).
Characteristics of the Patients
The highest value of HIV-RNA reached by the patients in their clinical history.
Baseline values, measurements within 12 weeks before the initiation of interferon-based therapy. Values are expressed as mean (±standard deviation) for continuous variables and number of patients (%) for categorical variables. Continuous data were analyzed using the Wilcoxon nonparametric test and categorical variables by Fisher's exact test.
SVR, sustained virological responders; BMI, body mass index; IVDU, intravenous drug users (mode of HIV transmission); cART, combined antiretroviral therapy; PI, protease inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitor; AST, aspartate aminotransferase; ALT, alanine aminotransferase; IU, international units; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Throughout a median follow-up of 24 months (range 6–60 months), six patients showed a detectable HIV viral load (three in the SVR group and three in the non-SVR group), and 27 changed antiretroviral regimen because of intolerance or for therapy simplification (12 patients in the SVR group and 15 in the non-SVR). None of the patients developed a new AIDS-defining event or died during the follow-up period. The effect of SVR versus non-SVR on the CD4 counts and percentage over time was not statistically significant (Fig. 1).
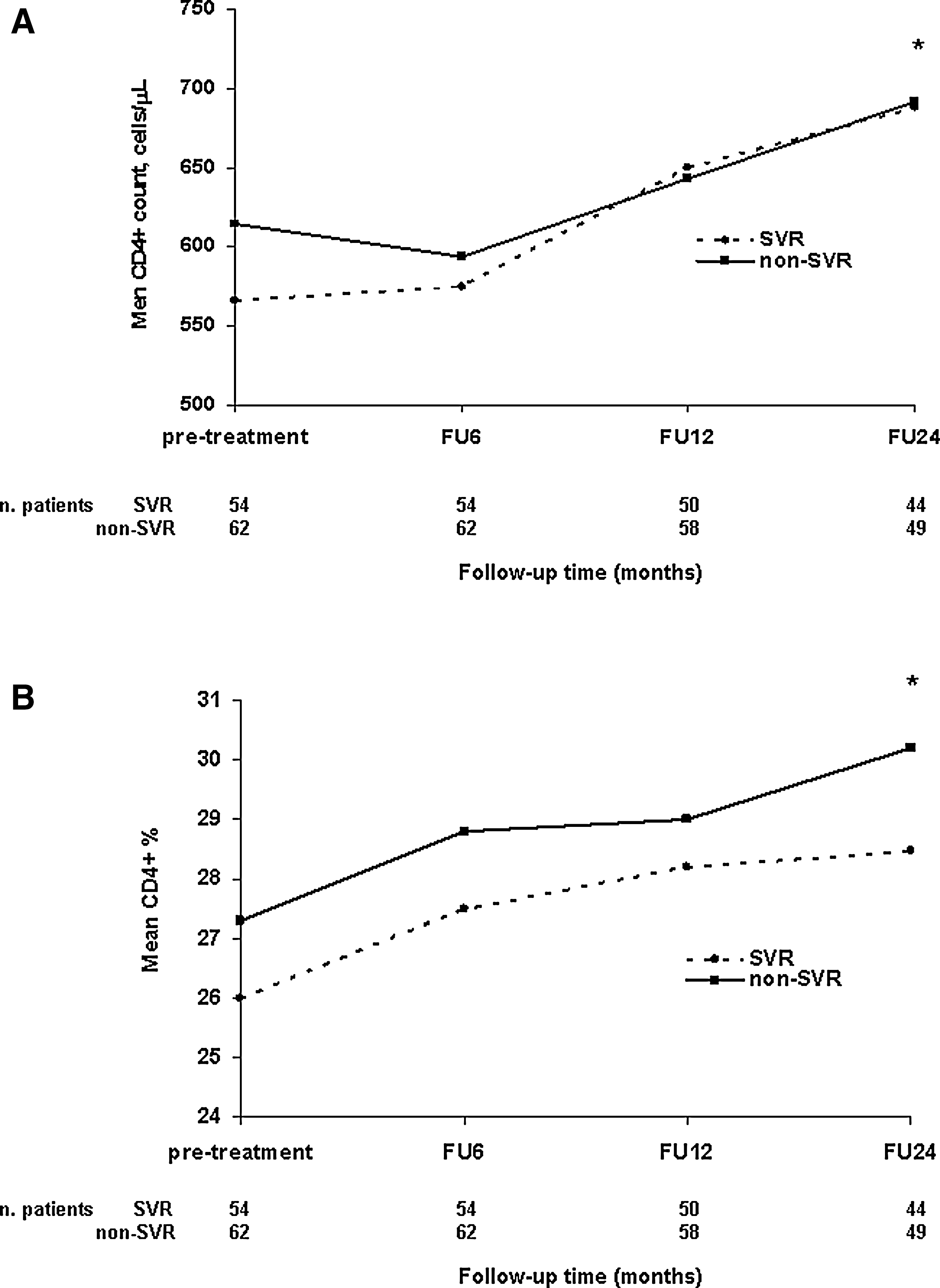
After the interferon-induced expected decline of the CD4 counts, no difference in CD4 cell recovery was observed between the two groups (p=NS). Nevertheless, a statistically significant increase from baseline in CD4+ T cell counts was observed in the SVR group at months 12 and 24 with a mean annual increase (±SD) of 84 cells/μl (±220 cells/μl) at 1 year and of a further 38 cells/μl (±212 cells/μl) within the second year (p=0.01, 0.001, respectively). A nonsignificant mean increase of 77 cells/μl (±229 cells/μl) occurred in the non-SVR group within month 24 (p=0.06). CD4% yielded similar results, showing a significant increase from baseline in both study groups at month 24 (p=0.001).
Linear regression analysis evaluating the mean changes from baseline in CD4 cell counts and percentage at the three different follow-up time points is reported in Table 2. The achievement of SVR after Peg-IFN-RBV therapy of HCV infection was not significantly associated with the change in CD4+ T-lymphocyte count during 24 months of follow-up. A higher nadir CD4 T-lymphocyte count heightened the likelihood of a CD4 increase within 24 months after IFN suspension (β-coefficient 0.48; p=0.0005). Conversely, lower pre-interferon CD4 counts were the strongest factor associated with greater CD4 gains throughout the study period (β-coefficient −0.41; p<0.0001).
Multivariate Linear Regression Analysis Indicating the Differences in Mean Changes from Baseline CD4+ Cell Counts and CD4+ Percentage over 24 Months of Follow-up According to Different Variables
β, beta coefficient; SE, standard error of β; FU, follow-up; IVDU, intravenous drug user; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; cART, combined antiretroviral therapy; BMI, body mass index; SVR, sustained virological responders; NR, nonresponders; vs., versus.
When the Fib-4 index was used as a linear variable, higher degrees of the Fib-4 index were associated with smaller increases in absolute CD4 counts [β-coefficient −34.46, p=0.003; data not shown), but not in CD4%. Nevertheless, significant fibrosis as defined by a Fib-4 index >3.25 (F3-F4 of the Ishak classification) was not related to the change in CD4+ T-lymphocytes count (β-coefficient −56.13; p=0.18). In addition, the risk of a smaller increase in CD4 counts was significantly higher in subjects with higher BMI (β-coefficient −20.75; p=0.0008). Finally, antiretroviral regimen received and HCV genotype were assessed and no associations with CD4 recovery were identified.
Recently, Potter et al. found that CD4 increase is negatively affected by the ongoing HCV replication in coinfected patients initiating cART, when chronically HCV-RNA-positive subjects were compared with spontaneous clearers. 14
We evaluated in HIV/HCV patients on successful cART if HCV-RNA clearance, following standard anti-HCV therapy, might influence the long-term CD4 cell recovery. The study population was well balanced for all possible variables and showed that over a mean follow-up of 24 months the clearance or the persistence of HCV replication did not influence the CD4 cell course.
Although the change in CD4 was not statistically different between sustained responders and non-SVR, the long-term CD4 counts following the end of therapy showed an increase in both study groups, which was statistically significant only in patients with SVR. This finding needs further investigations, as it cannot be ruled out that on a larger cohort the impact of SVR on CD4+ gain might be significant.
A possible explanation could be the persistent immune activation and CD4 T cell apoptosis associated with HCV infection. 15 This activation was shown to decrease in response to IFN-RBV until 24 weeks after treatment interruption, independently of treatment outcome. 16 A longer persistence of interferon-related reduced T cell activation might be responsible for the ongoing increase in CD4 cell count regardless of the success of HCV eradication.
We found that lower nadir of CD4+ cell count as well as higher pre-interferon values negatively affected the CD4+ increase after Peg-IFN-RBV treatment.
Although cirrhosis has been found to be associated with low CD4+ T cell counts as the consequence of splenic sequestration, 17 we could not find an association between CD4+ changes and Fib-4 index >3.25, probably because of the small number of patients with advanced fibrosis/cirrhosis in the whole cohort. However, since the Fib-4 index values increase gradually with the fibrosis stage, 18 its use as a continuous variable, regardless of its poor diagnostic accuracy, suggested that increasing fibrosis was associated with a smaller rise in CD4 counts.
In addition, a higher BMI showed a negative effect on CD4+ rise during the follow-up, in agreement with a previous report showing that body weight was associated with smaller increases in CD4 after the initiation of cART. 19 Finally, although in a recent report from the MASTER cohort subjects infected with genotype 3 showed an impaired late immune recovery after cART initiation, 20 in our study genotype 3 was not shown to influence the CD4 course when compared with other genotypes. This is possibly due to the longer exposure to cART in our cohort (11 years), which could have further reduced the influence of HCV coinfection on CD4 gain.
Our study has several limitations such as the relative small number of patients studied and the lack of information about CD8+ T cell counts, liver histology, and adherence to cART. Nevertheless, the use of the Fib-4 index as a surrogate marker of liver fibrosis and the persistence of HIV suppression throughout the study period in all but six patients made it possible to partly overcome these biases.
In conclusion, HCV clearance does not seem to influence the long-term course of CD4+ in patients on long-lasting, efficient cART. As suggested by our data and considering the conflicting results existing on the impact of HCV-RNA on immune restoration in HIV-infected patients on cART with persistently suppressed HIV replication, 7,10,14 other HCV-related factors, such as the degree of liver fibrosis, should be taken into account in further analyses.
Footnotes
Acknowledgments
This work was supported by FIRST (Fondo Interno per la Ricerca Scientifica e Tecnologica) 2009, Università di Milano. The statistical analysis work was supported by “Fondazione Romeo ed Enrica Invernizzi.”
Author Disclosure Statement
No competing financial interests exist.