
Abstract
Tenofovir (TFV) 1% gel has proven effective in preclinical and clinical studies in preventing sexual transmission of HIV-1. The impact of changing the current gel formulation to reduce its osmolality was evaluated using pharmacokinetic assessments and local tissue effects in the rabbit. Following vaginal administration of TFV 1% gel and reduced-glycerin TFV 1% gel, TFV was measured in plasma, vaginal tissues, vaginal fluids, and iliac lymph nodes. After a single dose, plasma C max and AUC0–4h were significantly higher in the TFV 1% gel group compared with the reduced-glycerin TFV 1% gel group. After 14 days of once-daily dosing, differences in these parameters were insignificant. Vaginal fluid concentrations were ∼100 μg/ml following the first dose and up to a mean of about 500 μg/ml after 14 once-daily doses. Mean (and median) cranial TFV tissue concentrations were generally in excess of 100 μg/g following a single dose and 14 once-daily doses of both gels; concentrations in the caudal vaginal tissues were comparatively lower, although in nearly all cases mean values exceeded 10 μg/g. Treatment of tissues with phosphatase to liberate TFV from its diphosphate and monophosphate metabolites increased recovery of TFV by 60–120%. Median TFV concentrations in iliac lymph nodes ranged from 44 ng/g to 196 ng/g; differences between iliac lymph node TFV concentrations following dosing of the two gels were insignificant. There were no differences observed in histological evaluation in the cranial vagina following 14 days of once-daily dosing of either gel. There was an apparent impact of TFV on rabbit vaginal epithelium (increased secretory depletion and increased cellular vacuolization) independent of formulation. These data indicate that the reduced-glycerin TFV 1% gel may be a suitable alternative to TFV 1% gel.
Introduction
T
Histological changes in ectocervical and colorectal tissues have been observed in vitro following exposure to TFV 1% gel. 8 TFV 1% gel and the matching placebo gel induced transient changes (reduced electrical resistance) in epithelial monolayer integrity and induced epithelial fracture in ectocervical and colorectal explants compared with tissues exposed to medium only. 8 The relevance of these findings to safety in vivo is unclear. TFV 1% gel administered vaginally is considered safe and well-tolerated in human clinical studies. 9,10 However, in a Phase I clinical study (RPM-02/MTN-006) involving rectal administration of TFV 1% gel, some adverse events were noted. 11 Lower gastrointestinal distress was reported in the TFV 1% gel arm, leading to potential safety and acceptability concerns.
Hyperosmotic gels have been found to impact vaginal and, in particular, rectal tissue integrity in vitro and in vivo. 12 –15 A possible explanation for the effect of the vaginal formulation of TFV applied rectally is the high osmolality of the TFV 1% gel. The vaginal TFV 1% gel was reformulated to reduce the osmolality. The reformulated gel, referred to as reduced-glycerin TFV 1% gel, was designed to have similar physical properties (i.e., rheological) compared with TFV 1% gel. The reduced-glycerin gel was assessed under in vitro conditions using Caco-2 epithelial monolayers and colorectal explants and was found to be better tolerated with no loss in anti-HIV-1 activity compared with TFV 1% gel. 16
In this work, the reduced-glycerin TFV 1% gel was evaluated relative to the TFV 1% gel using pharmacokinetics in rabbits dosed vaginally to determine if the two formulations performed in a similar manner in vivo. In addition to pharmacokinetics, the local tissue effects were assessed by histology to observe any differences exerted by the two gel formulations following 14 days of once-daily dosing.
Materials and Methods
Materials
TFV drug substance was obtained from Gilead Sciences (Foster City, CA). Excipients [purified water, HEC (205 XH PHARM), glycerin, citric acid, edetate disodium, methylparaben, and propylparaben] were either United States Pharmacopeia (USP) or National Formulary (NF) grade. TFV-d6 (internal standard) was obtained from Toronto Research, Inc. (North York, Canada). Phosphatase, Acid Type XA from sweet potato (P1435-500UN, 096K7351) was obtained from Sigma Chemical Co. (St. Louis, MO). Weck-Cel surgical spears were obtained from Medtronic Ophthalmics (Jacksonville, FL). Covaris glass tubes for sonication were obtained from Qsonica (Newtown, CT).
Formulations
The TFV 1% gel is composed of HEC, glycerin (20%), citric acid, edetate disodium, methylparaben, and propylparaben. The glycerin provides lubricating properties to the gel. Reduced-glycerin TFV 1% gel was prepared with 5% glycerin and a 10% increase in the HEC concentration to maintain a viscosity similar to that of TFV 1% gel. The reduced level of glycerin (5%) was the same as used in the preparation of combination gels containing TFV and UC781. 17 The balance of the glycerin removed in the reduced-glycerin TFV 1% gel was replaced with water. All other ingredients were unchanged. The gels were prepared at DPT Laboratories (San Antonio, TX). The osmolality of the reduced-glycerin gel was 850 mOsmol/kg.
Rabbit study
The pharmacokinetics of TFV following vaginal administration of TFV 1% gel and the reduced-glycerin TFV 1% gel were evaluated in female New Zealand White Hra (NZW) SPF rabbits weighing approximately 2.5 kg. The study was approved by the MPI Research Institutional Animal Care and Use Committee (IACUC). Performance of this study followed the protocol reported previously for assessment of UC781-only gels 18 with the exception that 1.0 ml of gel was administered intravaginally to the rabbits in this study. One set of rabbits (n=6 per group) was dosed once with each gel formulation and sacrificed 4 h postdose. Blood was collected predose and at 30 min and 1, 2, 3, and 4 h postdose. A second set of animals (n=6) was dosed once daily for 14 days with each gel formulation. On day 14, blood samples were taken before the final dose and at 30 min and 1, 2, 3, and 4 h postdose, followed by sacrifice 4 h after the final dose. Blood (1 ml) was collected from the jugular or other suitable vein and placed in tubes containing K3EDTA and stored on ice until centrifuged.
Vaginal fluids were collected by placing a Weck-Cel surgical spear into the vagina to absorb secretions from the caudal vagina. The spears were weighed before and after fluid collection. Vaginal fluids were collected by inserting the spear into the vagina toward the lateral wall for approximately 1 min. Following collection, the spears were placed in tubes, weighed, and stored on dry ice at −70° to −80°C until analysis.
Animals were euthanized by an overdose of Euthasol (approximately 1.0–2.0 ml/animal) administered via the marginal ear vein followed by auscultation, bilateral pneumothorax puncture, or exsanguination. Following sacrifice, iliac lymph nodes were identified and collected. As many lymph nodes as could be found were collected from each animal and placed together in polypropylene cryovials. The tissues were then snap frozen at −80°C and stored at −70° to −80°C until analysis.
Tissue samples were collected at the time of sacrifice. The cranial (abdominal region, or proximal to the site of the administered gel) and the caudal (urinary region, or distal to the site of the administered gel) of the vagina were separated and transferred into cryovials The tissues were then snap frozen at −80°C and stored at −70° to −80°C until analysis.
TFV bioanalysis in plasma
This bioanalytical method, and those described below, was fully validated according to the FDA Guidance for Industry: Bioanalytical Method Validation, May 2001. Acceptance criteria for all bioanalytical methods were developed and validated and results for each test are found in Table 1. Plasma samples (100 μl) were added to a 96-well plate followed by addition of 50 μl working internal standard TFV-d6 (50 ng/ml in methanol/water, 50:50). Then 0.5% formic acid (500 μl) was added to each plate well and the plate gently mixed by hand for ∼20 s. The samples were then transferred to preconditioned (addition of 800 μl methanol and 800 μl 0.5% formic acid, respectively, using minimal vacuum) solid phase extraction (SPE) plates (Oasis MCX 96-well plate, 30 μm, 10 mg) and drawn through using minimal vacuum (vacuum duration ∼5 min). Next, formic acid (0.5%, 800 μl) was added to each well and drawn through with vacuum until the bed surface appeared dry; the same process was repeated using 800 μl methanol. This step was followed by application of full vacuum for 2 min. Elution was performed with 600 μl methanol/NH4OH (95:5) and the samples were evaporated to dryness under a stream of N2 at a temperature of 50°C. The samples were reconstituted with 200 μl water. The plate was then capped and gently vortexed for 20 s.
Results for all tests meet the acceptance criterion/criteria.
TFV, tenofovir; IS, internal standard; ULOQ, upper limit of quantitation; RE, relative error; R 2, coefficient of determination; RSD, relative standard deviation; LLOQ, lower limit of quantitation; QC, quality control; NP, not performed.
TFV in samples prepared as described above was measured using an Agilent 1100 Series HPLC system coupled to an Applied Biosystems/MDS Sciex API 5000. MS/MS data were obtained in the positive polarity mode. The analytical column used was a Phenomenex Synergi Polar-RP 80A, 75×2 mm, 4 μm with a Phenomenex SecurityGuard Polar-RP, 4-mm×2-mm guard column. The column was held at ambient temperature. An isocratic mobile phase consisting of 0.1% acetic acid in water (98%) and 0.1% acetic acid in acetonitrile (2%) was used at a flow rate of 300 μl/min. The injection volume was 10 μl; the total run time was 4 min. The autosampler was held at a temperature of 5°C. Under these conditions, the retention time of TFV was 1.60 min and that of the internal standard TFV-d6 was 1.58 min. The lower limit of quantification (LLOQ) of this method was 1.0 ng/ml while the upper LOQ (ULOQ) was 5000 ng/ml.
TFV bioanalysis in vaginal fluids
The Weck-Cel spear samples were thawed to room temperature. The internal standard, TFV-d6 (50 μl, 20 μg/ml in methanol/water, 50:50), was then added to each tube. Then 1000 μl of methanol/water (50:50) was added to the tubes. The tubes were briefly vortexed at the highest setting and then placed into a multitube vortexer and vortexed for 5 min at the highest setting. Next, the tubes were centrifuged for about 5 min at 4500 rpm at a temperature of 5°C. Then 250 μl of the supernatant was transferred to a 96-well plate (1 ml). The samples were then injected onto the LC-MS/MS for analysis. The method used was that described above for analysis of TFV in rabbit plasma. The LLOQ was 5.0 ng/spear to 500 ng/spear for this method.
TFV bioanalysis in tissues
Frozen tissue was ground in a coffee grinder-type small blade homogenizer with dry ice to make a finely ground tissue sample. The sample was then placed in a freezer at −20°C overnight to allow the dry ice to sublime. The samples were transferred to a cryogenic tube for storage at −80°C. The ground tissue (100 mg) was diluted 10-fold with the extraction solvent (1.0 ml of acetonitrile/H2O, 1:1, v/v) in a 2-ml amber cryovial. The samples were then sonicated in an ice bath for 15 min. The samples (200 μl) were added to a 96-well extraction plate. Next, the working internal standard TFV-d6 (50 μl, 20 μg/ml in methanol/water, 50:50) was added. The plate was capped and vortexed for about 30 s. The plate was then centrifuged (∼4000 rpm) for approximately 5 min at a temperature of 4°C. The samples were subsequently analyzed by LC-MS/MS using the same equipment for analysis of TFV in plasma, except that the MS/MS was operated in the negative polarity mode. The analytical column used was a BioBasic AX 50×3.0 mm, 5 μm without a guard column. A gradient solvent system consisting of mobile phase A: acetonitrile/10 mM ammonium acetate in water, pH 6.0 (30:70) and mobile phase B: acetonitrile/1 mM ammonium acetate in water, pH 10.5 (30:70) was used. The gradient system consisted of steps starting at 95% A:5% B to 100% B over 2.1 min, after which 100% B was used until 8 min was reached. The flow rate was 400 μl/min; the injection volume was 5.0 μl and the column was held at ambient temperature. The autosampler was held at a temperature of 5°C. Under these conditions, retention times of TFV and the internal standard were 4.9 min. The LLOQ of this method was 2.0 ng/g and the ULOQ was 500 ng/g.
Total TFV bioanalysis in tissues
The processing method above measures the amount of free tenofovir in tissues. The amount of total TFV in tissues was measured following treatment with phosphatase to liberate TFV from its monophosphate and diphosphate esters. The working internal standard TFV-d6 (50 μl, 20 μg/ml in methanol/water) was added to the tissue samples obtained following sonication (described above). Freshly prepared phosphatase working solution (25 units/ml phosphatase in 50 mM ammonium acetate, pH 4.0; 50 μl) was added to 100 μl of sample solution and mixed by vortexing for ∼20 s in a 96-well plate. The plate was then covered with sheets of sealing film and incubated in a water bath at a temperature of 40°C for 40±5 min. Next, a 96-well filtration plate (Phenomenex Strata Impact Protein Precipitation 2-ml Square Well Filter Plate; PPT) was placed onto a 96-well sample processing manifold with a 96-well collection plate in position. Acetonitrile (600 μl) was added to all wells of the filtration plate. The samples were then transferred to the PPT filtration plate and allowed to stand for 5 min. Then vacuum was applied to the filter plate and the whole filtrate was collected. This filtrate was evaporated to dryness under a stream of N2 at a temperature of ∼50°C. The samples were then reconstituted with 200 μl water. The plate was capped and vortexed for 30 s. The samples were injected onto the LC-MS/MS for analysis. The method used was that described above for analysis of TFV in rabbit plasma. The LLOQ was 10.0 ng/g to 5000 ng/g for this method.
TFV bioanalysis in iliac lymph nodes
Lymph node samples (100–200 mg) were transferred from the polypropylene cryovials to the center of a Covaris TissueTube bag. A preweighed Covaris 13-mm×65-mm glass tube with cap was then attached to the 13-mm adaptor plug on the bag. The bag containing the tissue sample was immersed in a dry ice/acetone batch for at least 30 s. The frozen sample was then dry pulverized with a single hammering using a Covaris CryoPrep System (Covaris, Inc., Woburn, MA) at a setting of 4. The bag containing the pulverized sample was placed in the dry ice/acetone bath for about 15 s. The bag and glass tube were then flipped over into the dry ice/acetone bath to cool the glass tube. The powdered sample was transferred into the glass tube, followed by removal of the tube from the bag. The tube containing the sample was capped and weighed. For each 100 mg of sample, 1 ml of methanol/water (60:40) was added to the tube. The sample was then sonicated using a Covaris S-Series SonoLab sonicator. The bath temperature was set at 10°C. Sonication consisted of four treatments of 30 s each. Cycle 1: duty cycle=2%, intensity=10, cycles/burst=200; Cycle 2: cycle=10%, intensity=10, cycles/burst=500; Cycle 3: cycle=10%, intensity=10, cycles/burst=200; and Cycle 4: cycle=1%, intensity=10, cycles/burst=200. The lymph node homogenate was centrifuged at 4000 rpm at 5°C for 10 min; the supernatant was then transferred into new centrifuge tubes.
The samples were extracted using Microcon Centrifugal Filter Devices (Amicon Ultra–0.5 ml, 50K). Using a 96-well plate, the TFV-d6 internal standard [20 μl, 20 μg/ml in methanol/water (1:1)] was added to the samples. Then the entire contents of the samples were transferred into the sample reservoir of the filter device and capped. The filter device was then placed in an Eppendorf Centrifuge 5417C and counterbalanced with a similar device. The samples were centrifuged at 14,000×g for 20 min. Following removal of the assembly from the centrifuge, the sample reservoir was separated from the vial. Then 65 μl of each sample was transferred from the vial to a new 96-well plate. Sixty-five microliters of 1% formic acid in water was added to each sample and mixed well. The plate was then centrifuged at 4500 rpm for 5 min.
TFV extracted from isolated from iliac lymph nodes was analyzed using an Agilent 1100 Series HPLC system coupled to an Applied Biosystems/MDS Sciex API 5000. MS/MS data were obtained in the positive polarity mode. The analytical column used was a Agilent Zorbax XDB-C8, 75×4.6 mm, 3.5 μm. The column was held at ambient temperature (∼25°C). A gradient solvent system consisting of mobile phase A: 0.2% formic acid/5 mM ammonium acetate in water and mobile phase B: 0.2% formic acid in methanol was used. The gradient system consisted of steps starting at 80% A:20% B to 5% A:95% B over 2.1 min, after which the step returned to 80% A:20% B until 5.2 min was reached. The flow rate was 700 μl/min; the injection volume was 10.0 μl. The autosampler was held at a temperature of 5°C. Under these conditions, the retention time of TFV and the internal standard was 1.05 min. The LLOQ of this method was 20.0 ng/ml with an ULOQ of 10,000 ng/g.
Pharmacokinetic analysis
Plasma pharmacokinetic parameters were determined by noncompartmental methods using WinNonLin Professional, Model 200 for extravascular data (NCA Program, Version 5.2, Build 200701231637, Pharsight Corporation, Mountain View, CA). Values below the LLOQ were treated as 0 for analysis. All statistical comparisons were performed using two-tailed heteroscedastic t-tests.
Microscopic tissue examination
Microscopic examination of fixed hematoxylin- and eosin-stained paraffin sections was performed on the cranial vaginal tissue from rabbits at the day 14 necropsy. The slides were examined by a board-certified veterinary pathologist. A four-step grading system was used to define gradable lesions for comparison between dose groups.
Results
Plasma TFV concentrations over time following vaginal dosing of the two gels are shown in Fig. 1. Individual and mean plasma concentrations were higher in the TFV 1% gel group after a single dose and after 14 days of once-daily dosing compared with the reduced-glycerin TFV 1% gel formulation group. Plasma TFV concentrations were more variable in the TFV 1% gel group than in the reduced-glycerin TFV 1% gel group at days 1 and 14. The pharmacokinetic parameters measured are summarized in Table 2 and suggest there is lower systemic exposure of TFV from the reduced-glycerin gel formulation than the TFV 1% gel after single or repeated daily dosing. The difference between C max on day 1 between the two gels was statistically significant (p=0.001); likewise the difference in the AUC0–4h on day 1 between the two groups was statistically significant (p=0.001). TFV was absorbed more rapidly from the reduced-glycerin formulation compared with TFV 1% gel based on T max data on day 1 (0.58±0.20 h vs. 0.92±0.20 h, respectively; p=0.025). On day 14, there were no significant differences (i.e., p>0.05) between T max, C max, AUC0–4h, or AUCinf between the two gels.
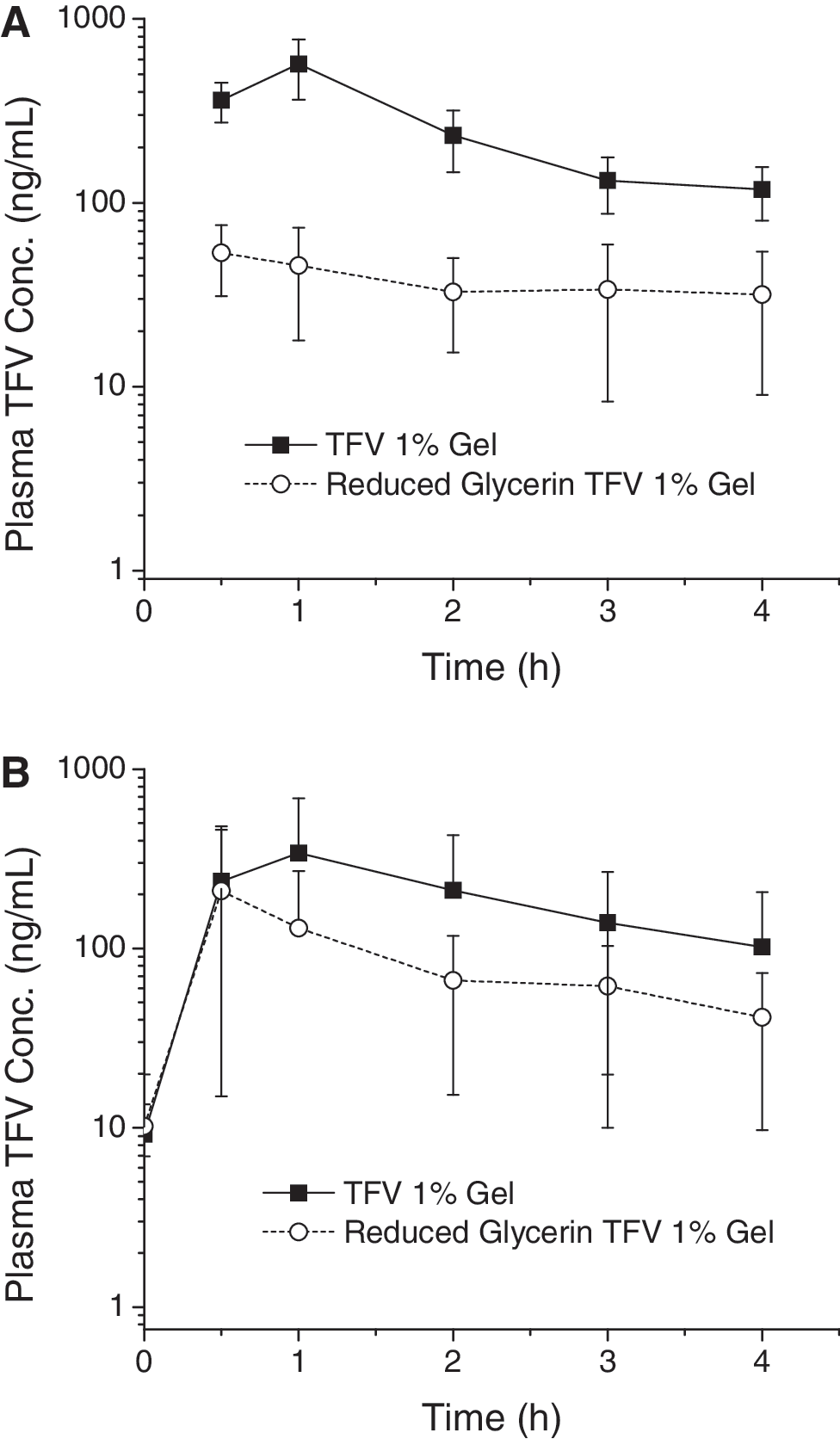
Plasma concentrations over time following vaginal administration of 1.0 ml of tenofovir (TFV) 1% gel or reduced‐glycerin TFV 1% gel to rabbits. Data are means±SD (n=6).
AUC0–4h, area under the concentration time curve from 1 to 4 h.
AUCinf, area under the concentration time curve calculated to infinity.
One animal had a value above the LLOQ at 4 h; datum shown is from this animal.
Five animals had values above the LLOQ at 4 h.
Data are means±SD (n=6) except where noted.
The TFV concentrations (μg/ml) in vaginal fluid collected 4 h postdose on day 1, predose on day 14, and 4 h postdose on day 14 are summarized in Table 3. None of the TFV concentrations in vaginal fluid was significantly different for the two gel formulations at any of the three time points tested.
Data are means±SD (n=6).
The concentration of TFV in vaginal tissues was measured following sacrifice 4 h after the first dose or 4 h after the final dose of 14 days of once-daily dosing. In addition to TFV, total TFV [that following treatment of tissue homogenates with phosphatase to hydrolyze any TFV-monophosphate (TFV-MP) and TFV-diphosphate (TFV-DP) formed] was measured. The data collected from both gels are shown in Fig. 2. Mean cranial vaginal tissue TFV and total TFV concentrations after a single dose and after 14 days of once-daily dosing of either gel formulation typically exceeded 100 μg/g tissue. Concentrations were lower in caudal vaginal tissue compared with those in the cranial vaginal tissue (where the dose was administered). In all cases, the amount of total TFV was greater than the amount of TFV. None of the differences in TFV or total TFV concentrations between gels or after a single dose or multiple doses was statistically significant (p>0.05).
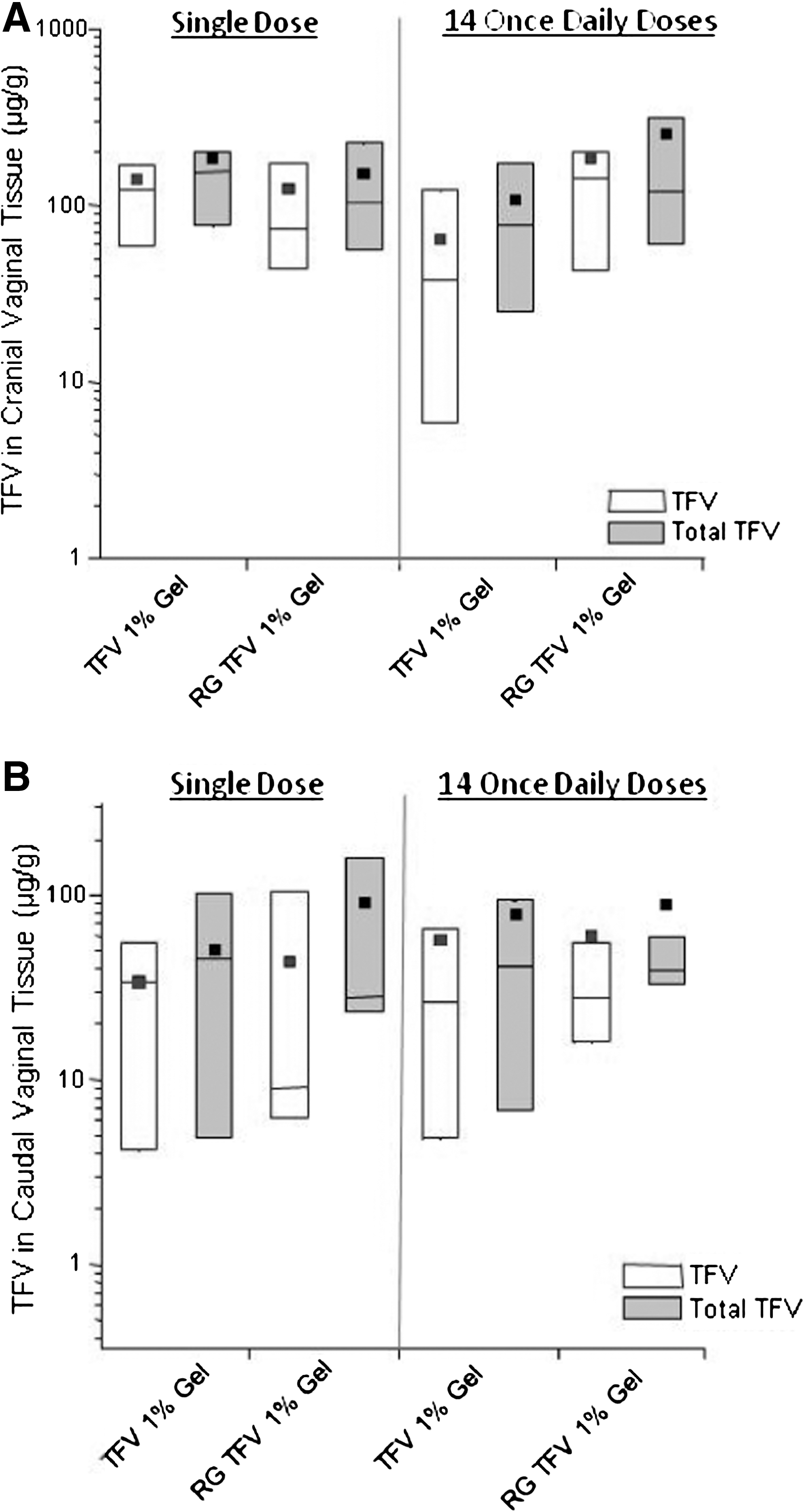
Box plots of vaginal tissue concentrations (TFV and total TFV) following a single dose or 14 once daily doses of TFV 1% gel or reduced‐glycerin 1% TFV gel (RG TFV 1% gel) in the cranial
The concentration of TFV in iliac lymph nodes was measured at the time of sacrifice (4 h postdose on day 1 or 4 h postfinal dose on day 14). Data collected at these times from both TFV gels are shown in Table 4. The differences at both time points and between gel formulations were statistically insignificant (p>0.05).
Data are means±SD (n=6).
There were no test article-related macroscopic observations noted on day 1 or day 14 following dosing of either gel. There were several test article-related microscopic observations present in the cranial vaginas of both groups on day 14. The incidence of test article-related observations is summarized in Table 5. Both gels led to observations of mucosal atrophy, secretory depletion, heterophil infiltration, and increased vacuolization. Of these observations, secretory depletion was the most pronounced, with three of six rabbits dosed with both TFV 1% gel and reduced-glycerin TFV 1% gel judged as severe. The incidence of mucosal atrophy, secretory depletion, heterophil infiltration, and increased vacuolation was similar following 14 days of administration of both gels; any qualitative differences were considered to be biologically insignificant.
In general, the lesion is easily identified but of limited severity. The lesion probably does not produce any functional impairment (11–20% of the tissue involved).
The lesion is prominent but there is significant potential for increased severity. Limited tissue or organ dysfunction is possible (21–40% of the tissue involved).
The degree of change is either as complete as considered possible or great enough in intensity or extent to expect significant tissue or organ dysfunction (41–100% of the tissue is involved).
The amount of change present barely exceeds what is considered to be within normal levels (10% or less of the tissue is involved).
Discussion
The reduced-glycerin TFV 1% gel was compared with the TFV 1% gel in rabbits to determine if the reduction in glycerin resulted in any changes in the pharmacokinetics of TFV. Following the first dose, the plasma pharmacokinetic parameters C max and AUC0–4h were significantly higher in the TFV 1% gel group compared with the reduced-glycerin TFV 1% gel group. Both parameters were higher in the TFV 1% gel group after 14 days of once-daily dosing, but these differences were insignificant. Likewise, T max was impacted by the reduction in glycerin content. These differences could be due to the change in gel osmolality or topical effects produced by glycerin associated with the different gel formulations; however, histological findings were similar in each group (see the discussion below). The variability in plasma pharmacokinetic parameters at day 14 was markedly higher in both groups than after a single dose. This variability has been observed in other rabbit pharmacokinetic studies involving vaginal administration of microbicide gels. 18,19 It is important to evaluate the reduced-glycerin formulation in women to determine if the differences observed in rabbits constitute a real difference. Changes in systemic levels of TFV should probably not impact efficacy since this will be controlled primarily through local tissue concentrations.
TFV concentrations in vaginal fluids were assessed using Weck-Cel surgical sponges. The sponge was placed on the lateral wall of the vagina approximately 1 cm into the vagina for about 1 min. The mean fluid concentrations at 4 h postsingle or 14 daily doses were roughly equivalent to the tissue concentrations in the cranial and caudal vagina. Prior to the last dose on day 14 (i.e., ∼24 h postdose on day 13), TFV levels in fluid were lower, with means of 4.5–19.4 μg/g. Urinary drainage in the rabbit occurs through the caudal vagina. It is likely that urine dilutes caudal vaginal fluid, which would explain the relatively low fluid concentrations at these longer time points postgel administration and the somewhat lower TFV tissue concentrations in the caudal vagina compared with the cranial vagina (see below).
TFV and total TFV vaginal tissue concentrations were measured in both the cranial and caudal vagina following a single dose and 14 days of once-daily dosing. The mean concentrations in the cranial vagina were ∼100–250 μg/g and were similar after a single dose and 14 days of once-daily dosing. The concentrations in the caudal vagina were lower but within an order of magnitude of those measured in the cranial vagina. These concentrations are in considerable excess of the IC50s required to inhibit HIV-1 infection of several cell types in vitro. 20 In the CAPRISA 004 clinical study, vaginal tissue concentrations were found to range from 1 to 10 μg/g tissue. 21 These human data were collected 24 h following a 4 ml dose of TFV 1% gel. The rabbit vaginal tissue concentration data were collected 4 h postdose of 1 ml of TFV 1% gel (and reduced-glycerin TFV 1% gel). Another study examining the human pharmacokinetics following single and multiple doses of TFV 1% gel gave TFV C max concentrations in vaginal tissues of 22 μg/ml 2 h following a single dose of gel and 2.7 μg/ml 4 h after multiple dosing. 22
Since TFV-DP is the active anabolite of TFV that inhibits viral replication, its intracellular concentration after topical application is of considerable interest. Efforts to develop a method that quantitatively measures TFV-DP in rabbit vaginal tissue proved difficult to validate, particularly because it is not possible to prepare standards wherein TFV-DP is located intracellularly. In this study, tissue samples were treated with phosphatase to hydrolyze phosphorylated compounds. During method validation, it was confirmed that this treatment completely converted TFV-DP and TFV-MP to TFV (total TFV). The concentrations of total TFV in tissues from the cranial and caudal vagina at day 1 or day 14 ranged from 60% to 120% higher than TFV, regardless of gel formulation. These data suggest that a substantial amount of TFV was converted to TFV-DP (and TFV-MP) in rabbit vaginal tissue.
The concentration of TFV in iliac lymph nodes was less than measured in vaginal tissues. To date, little is known about the concentration of TFV in the lymphatic drainage system in the vagina. The values reported herein were similar following a single dose or 14 once-daily doses of gel, with no differences noted between the two formulations. The concentration of TFV in local lymph nodes could be important because it is currently believed that infected Langerhans cells and dendritic cells migrate from the vaginal mucosa into the lymphatics. 23,24 Ideally, a microbicide would reach effective concentrations in the lymphatics to prevent incorporation of HIV-1 virions into infective lymphatic CD4+ T cells. 25 The data collected in rabbits indicate that TFV does reach the iliac lymph nodes. Whether similar transport of TFV occurs in humans and whether the resultant concentrations are therapeutically effective are unknown.
It is desirable to perform bioanalysis using one method to quantitate the TFV from different matrices. In the future, a single method for detection of TFV (and TFV-DP) from a variety of matrices will be pursued to minimize sample requirements and reduce costs.
The local effect of TFV 1% gel on the vaginal epithelium was investigated in rats and rabbits prior to initiating human clinical testing and the gel was found to be well tolerated. 9 Subsequent clinical studies have reinforced this finding. 4 The impact on rabbit vaginal epithelial tissues was investigated herein to assess the impact of the relative levels of glycerin in each formulation. The histological data indicated that the amount of glycerin did not impact rabbit vaginal tissues. Despite the foregoing, there were histological observations in both groups suggesting that, at least in the cranial rabbit vagina, TFV does impact the epithelial tissues (see Table 5) after 14 days of once-daily gel administration.
The mechanism of action of TFV requires phosphorylation to form the anabolite TFV-DP. This species is a competitive inhibitor of HIV-1 reverse transcriptase and terminates the growing DNA chain. 26 At the same time, TFV-DP can inhibit host DNA polymerases, thereby inhibiting DNA replication and potentially causing side effects. Another possible mechanism of action is incorporation of analogs into nuclear DNA, which may lead to other potentially negative effects. 27 Thus, one explanation for the observed effects of locally applied TFV to rabbit vaginal mucosa results from TFV's known mechanism of action on host and viral replication processes, namely the effect on endogenous DNA replication.
Conclusions
The reformulated TFV gel (reduced-glycerin TFV 1% gel) had generally similar pharmacokinetics when compared with TFV 1% gel. Most importantly, both gels led to tissue concentrations throughout the rabbit vagina. Based on differences in TFV and total TFV measured in vaginal tissues, there appear to be relatively large amounts of TFV-DP formed even 4 h after a single dose of either gel. TFV is transported into iliac lymph nodes within 4 h following a single dose regardless of gel formulation. The impact of reducing the glycerin content of the gel formulation on the vaginal epithelium as measured by histology was negligible; however systemic exposure to TFV (as measured by plasma concentrations) was lower for the reduced-glycerin TFV 1% gel. These data indicate that the reduced-glycerin formulation may be a suitable alternative to TFV 1% gel.
Footnotes
Acknowledgments
The support of Missy Peet and Devon Kyle of MPI Research in coordination of the rabbit study and sample bioanalysis is gratefully acknowledged. We also acknowledge the pharmacokinetic analysis of John Trang. The editorial assistance of Jennifer Hurlburt of CONRAD is gratefully acknowledged. This work was funded by the United States Agency for International Development (USAID) under Cooperative Agreement GPO-A-00-08-00005-00. The views expressed by the authors do not necessarily reflect those of USAID.
Author Disclosure Statement
No competing financial interests exist.