
Abstract
Eleven protease mutations have been associated with reduced susceptibility to darunavir. In this study of 87 HIV-1-infected patients experiencing virological failure to second-line regimens containing protease inhibitors boosted with ritonavir (viral load >1,000 HIV RNA copies/ml), we observed a low prevalence (3%) of ≥3 darunavir resistance-associated mutations, indicating that this drug may be a good option for third-line antiretroviral therapy in southern India.
T
The YRG Centre for AIDS Research and Education (CARE) is a nonprofit medical and research institution in Chennai, India, that provides medical care to >15,000 HIV-infected individuals. All patients were treated according to WHO treatment guidelines. Patients were seen every 3 months or as clinically indicated. CD4 cell count monitoring was performed every 3–6 months, but routine viral load monitoring was not standard of care. For this cross-sectional study, 87 HIV-1-infected patients experiencing virological failure of second-line regimens containing PIs boosted with ritonavir (r) (viral load >1000 HIV RNA copies/ml) were studied. Overall, these individuals represented a minority of patients who entered second-line therapy. Genotyping was performed using a validated home-brew assay, as previously described.
7
Sequences were aligned (Clustal X) to an Indian subtype C reference (C.IN.AF067155) and examined for HIV-1 subtype in REGA v2.
8
The sequence data were analyzed using the Stanford HIV Drug resistance database available at
For the study population, the majority (98%) of sequences were HIV-1 subtype C and 2% were subtype A. The most common first-line regimens included zidovudine, lamivudine, and nevirapine (38%) followed by stavudine, lamivudine, and nevirapine (33%) and zidovudine, lamivudine, and efavirenz (8%). The median time until switching of regimens was 25 months (interquartile range, 13–50 months). The median PI exposure was 13 months (1–37 months), the median CD4 cell counts were 146 (8–472; IQR), and 55% of patients were exposed to atazanavir/r, 40% to indinavir/r, 5% to lopinavir/r, and none to DRV; 87% of patients demonstrated PI RAMs and 95% demonstrated RAMs to nucleoside reverse transcriptase inhibitors. Major PI RAMs were M46I (53%), I54V (46%), V82A (45%), L90M (39%), and others <20%. Major DRV RAMs were L76V (9%) and I84V (8%) followed by I54L (1%) and I50L (1%). Among minor DRV RAMs, L33F (9%), T74P (9%), L89V (2%), V11I (2%), and V32I (1%) were observed. Overall, 29 patients (33%) had any DRV RAM, of which 24 had one DRV RAM, two patients had two DRV RAMs, and one patient had ≥3 DRV RAMs (Figs. 1 and 2). An estimated sensitivity to DRV/r remained for at least 96% of patients exposed to previous PIs.

Frequency of 1, 2, and >3 darunavir (DRV) resistance-associated mutations.
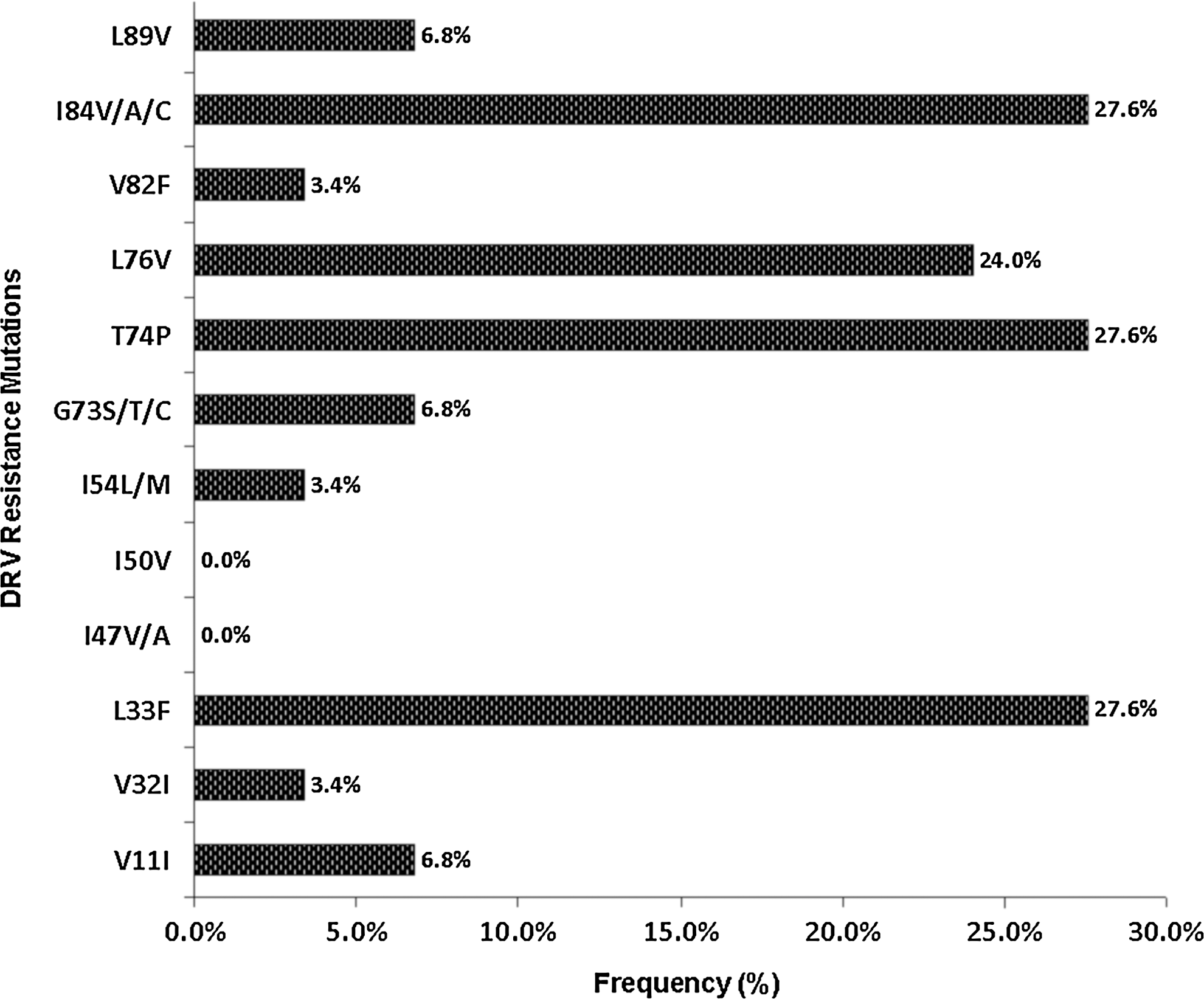
Frequency of individual DRV drug resistance mutations.
New agents with favorable cross-resistance profiles and activity against existing drug-resistant strains are a priority for clinical development. The distinct pattern of viral resistance selected by individual drugs is an important element for the design of ideal combination therapies. Ten of the 19 mutations associated with decreased DRV susceptibility were previously reported to be selected in vivo by DRV or to decrease the virological response to DRV salvage therapy: V32I, L33F, I47V, I50V, I54LM, T74P, L76V, I84V, and L89V. 11 Two additional mutations (L10F and V82F) have also been shown to decrease DRV susceptibility. 12 The RAM, V82F, which has the potential for PI cross-resistance, was found to be very minimal in this study (3.4%). Although V82F has not been reported to develop in viruses from patients receiving DRV/r, it has a major effect on DRV/r susceptibility in multivariate analyses of RAMs present in DRV/r resistant virus isolates. Additionally, I84A demonstrated reduced susceptibility to DRV in the VircoLab analysis, 13 and L33F was the predominant accessory mutation reported to be associated with a decreased virological response to DRV/r in the POWER and DUET studies. 14
In studies conducted in well-resourced settings and in modeled cost-effectiveness analysis, DRV/r has been demonstrated to be cost-effective compared to other PI/r in heavily pretreated patients. DRV/r has outperformed atazanavir/r, saquinavir, fosamprenavir/r, and lopinavir/r when used for salvage therapy in patients previously treated with multiple PIs. 6,15,16 The limitations of this study include the fact that it was cross-sectional and was designed to study the pattern of PI resistance mutations among viremic patients on second-line therapy. Moreover, those patients who failed second-line therapy were a minority of all patients who started second-line therapy, so prospective studies will be required to determine the actual number of patients who would need a third-line therapy in this setting. Although it has not been directly compared to tipranavir/r, it is likely to be more active in the majority of PI-experienced patients. 13 Furthermore, preliminary data suggest that DRV/r may also be more efficacious than lopinavir/r in PI-experienced patients who remain naive to lopinavir/r. 17 Based on these reports and our generated data, we have concluded that DRV may be a good option for third-line ART in southern India.
Footnotes
Acknowledgments
We are most grateful to the clinical and laboratory staff at YRG Centre for AIDS Research and Education, VHS, Chennai, India, for their facilitation of the study. We would like to thank the Fogarty AIDS International Training and Research Program (AITRP), Brown University, Rhode Island, for financial support, thus providing us with an opportunity to present the poster at the XVIII International AIDS Conference, 18–23, 2010. Work by D.M. Smith was supported by grants from the National Institutes of Health: AI69432, AI100665, MH62512, MH83552, MH097520, DA034978, AI36214, AI047745, AI74621, AI080353, and the James B. Pendleton Charitable Trust. Dr. Kantor was supported by the National Institute of Allergy and Infectious Diseases at the National Institutes of Health, Grant RO1AI66922
Author Disclosure Statement
No competing financial interests exist.