
Abstract
Some individuals remain HIV seronegative despite repeated unprotected exposure to the virus. Recent observations led to a concept that acquired immunity plays a role in protection or at least in altered susceptibility to HIV-1 infection in highly exposed seronegative (ESN) individuals. Our aim was to study HIV-specific cellular immune responses induced in parenterally and/or heterosexually ESN individuals. Nine seronegative injection drug users (IDUs), 10 seronegative individuals, and nine of their HIV-positive sexual and/or IDU partners from the cohort of IDUs were included in the study. The discordant couples had unprotected sex, and some of seronegative partners also had parenteral exposure. Cell-mediated responses were measured in peripheral blood mononuclear cells (PBMCs) by ex vivo interferon (IFN)-γ-ELISpot and ICS combining IFN-γ, tumor necrosis factor (TNF)-α, and interleukin (IL)-2 after stimulation with four consensus peptide pools (Nef, Gag, RT, Env, subtype A-EE). Thirteen out of 19 (68%) seronegative study subjects had strong Nef peptide pool-specific ELISpot responses, three (16%) subjects responded against the Gag peptide pool, and one subject had an RT peptide pool response. Nef peptide pool responses in ESN were as high as in seropositive subjects. The multiple HIV-specific cytokine production in both CD4+ and CD8+ T cells was shown for several ESN subjects. The functional profiles of the immune responses were different between seronegative and HIV-positive study groups. Whether the observed cellular responses have any protective role against HIV needs to be further investigated.
Introduction
I
Early immunologic studies reported HIV-specific T cell responses in seronegative partners of HIV-infected patients. 7,8 The importance of adaptive immune response induced by HIV exposure is discussed in many studies. HIV-specific CD4+ and CD8+ T cell responses were demonstrated in different ESN groups including commercial sex workers, 9,10 discordant couples, 3,4,11 –13 men who have sex with men (MSM), 14 –16 injection drug users, 17,18 healthcare workers, 19 and healthy neonates born to HIV-infected mothers who did not receive antivirals. 20 High expression levels of beta-chemokines, as well as HIV-specific interferon (IFN)-γ or interleukin (IL)-2-secreting T cells have been recognized in different cohorts of ESN individuals. 21
The objective of this study was to investigate HIV-specific cellular immune responses induced in parenterally and/or heterosexually ESN individuals. We measured cell-mediated responses in PBMCs by IFN-γ ELISpot and intracellular cytokine staining (ICS) combining IFN-γ, tumor necrosis factor (TNF)-α, and IL-2 after stimulation with four consensus peptide pools (Nef, Gag, RT, and Env).
Materials and Methods
Study participants
Nine seronegative injection drug users (IDUs), 10 seronegative non-IDUs, and nine of their HIV-positive sexual and/or IDU partners from the ongoing projects of the Biomedical Center 22,23 were included in the study. The participants were tested for HIV and interviewed regarding drug use and sexual practices.
Seronegative participants were eligible for enrollment if they reported at least 10 unprotected sexual contacts with HIV-positive partner in the preceding 12 months, or the occasion of shared injection paraphernalia within the last 3 months.
HIV-1 testing involved two HIV-1 antibodies enzyme immunological assays (EIA) (Vironostika HIV-1, Uni-Form-II plus-0; Biomerieux, Netherlands and Genscreeen HIV-1/2; Bio-Rad, France). Positive HIV-1 EIA tests were confirmed by Western blot (HIV-1 WB Type-1, Bio-Rad, France). Additionally the HIV RNA reverse transcriptase polymerase chain reaction (RT-PCR) tests were performed in the pools of serum samples (Amplicor HIV-1 Monitor test, Roche). The level of exposure to HIV in ESN subjects was evaluated during each visit if applicable (Table 1).
The number of unprotected sexual contacts with an HIV-positive partner within a year.
(+) the occasion of shared injection paraphernalia within the past 3 months.
IDU, intravenous drug use; wt, wild type; n/a, not analyzed.
All experiments were conducted with each participant's informed consent. Ethical approval was obtained from the Biomedical Center ethics review committees.
Sample collection and preparation
PBMCs were isolated from 10 ml of blood collected in EDTA anticoagulant by density gradient centrifugation (Ficoll-Hypaque, Sigma). After washing twice with DPBS (Gibco), the PBMCs were resuspended in freezing medium consisted of 90% fetal bovine serum (FBS) (Millipore) and 10% DMSO (Sigma), frozen slowly at −70°C, and stored in liquid nitrogen. One day before use, cells were thawed, washed twice with R10 (RPMI 1640 containing 100 U/ml penicillin, 100 μg/ml streptomycin, 2 mM
CCR5 genotype analysis
To determine whether volunteers inherited the 32-bp deletion within the transmembrane region of CCR5, DNA was isolated from PBMCs and amplified by PCR with primers and conditions previously described. 24,25 The amplicons were subjected to agarose gel electrophoresis, and the size was assessed for the presence of a 32-bp deletion.
Peptide pools
A panel of 451 overlapping peptides spanning HIV-1 subtype A-EE Env, Gag, RT, and Nef proteins 26 was synthesized in the State Research Institute of Highly Pure Biopreparations (St. Petersburg, Russia). The peptides were 15 aa long overlapping by 11 aa and were represented in four different gene-specific pools. Peptides were dissolved at a concentration of 55.6 mg/ml in 100% DMSO (Sigma-Aldrich). Pools of peptides were reconstituted in 90% PBS/10% DMSO; the concentration of each individual peptide in the pools was 100 μg/ml. A cytomegalovirus, Epstein–Barr virus, and influenza virus (CEF) peptide pool (C.T.L.) was dissolved in DMSO and subsequently diluted 1:50 in 90% PBS/10% DMSO to reach a final individual peptide concentration of 20 μg/ml.
IFN-γ ELISpot assays
Ninety-six-well membrane-bottom plates precoated with anti-IFN-γ monoclonal antibodies (1-D1K, Mabtech) were preincubated with R10 for 2 h at room temperature. Pools of HIV-1 peptides (final concentration of each peptide is 1 μg/ml) were than added to appropriate wells followed by PBMCs (l–2×l05 cells/well). PHA (Sigma), CEF-pool, and R10 were added to separate wells as positive and negative controls, respectively. All antigens were tested in triplicate.
After overnight (20–24 h) incubation at 37°C in 5% CO2, the plates were washed four times with 1× PBS (Gibco) containing 0.05% Tween 20 (Sigma) and incubated for 3 h with biotinylated anti-IFN-γ monoclonal antibody (mAb) (7-B6-1, Mabtech). After washing, the plates were incubated for 1 h with streptavidine-alkaline phosphatase conjugate (Mabtech), followed by conjugation with AEC substrate (Vector Laboratories). After the development of the spots, the plates' contents were discarded, and the plates were washed with tap water and air dried. Numbers of spot-forming units (SFU) were counted using the ImmunoSpot Series 5 Core ELISPOT Analyzer (C.T.L.).
A positive T cell response in ELISpots was defined by the distribution-free resampling (DFR) (2×) method described by Moodie and co-authors. 27,28 Peptide pools with adjusted one-sided p values of ≤0.05 were considered as positive. In addition to statistical significance, the mean background-subtracted response for the peptide pool had to be ≥50 SFU/106 PBMCs for the peptide pool to be considered positive.
Intracellular cytokine staining
Production of the intracellular IFN-γ, TNF-α, and IL-2 by CD3+CD4+ and CD3+CD8+ cells was examined in response to HIV peptide pools using multiparameter flow cytometry. PBMCs (l×l06 cells) were stimulated in 96-well round-bottom cultural plates with HIV peptide pools (final concentration 2 μg/ml) in the presence of anti-CD28 mAb, anti-CD49 (eBioscience), brefeldin A (Sigma), and monensin (Sigma). PMA (Sigma) and R10 were used as positive and negative controls, respectively. After incubation for 5.5 h at 37°C in 5% CO2, cells were washed, fixed, and permeabilized by fixation and permeabilization solutions (eBioscience), and stained with fluorochrome-conjugated mAbs for surface markers (antiCD4-PE-Cy5/antiCD3-PE-Cy5 or antiCD8-PE-Cy5/antiCD3-PE-Cy5, eBioscience) and intracellular antigens (anti-lFN-γ-FITC, anti-IL-2-PE, anti-TNF-α-biotin, eBioscience). After incubation, the plates were stained with streptavidin-TxRed (eBioscience). Then the cells were fixed in 1% formalin (Sigma), run on the Epics XL flow cytometer (Beckman Coulter), and the data were analyzed with WinList32 software. ICS gating strategy is presented at Fig. 1. Results were reported as percent of IFN-γ-, TNF-α-, or IL-2-producing CD3+CD4+ or CD3+CD8+ cells, respectively. T cells simultaneously expressing IFN-γ/TNF-α, IFN-γ/IL-2, TNF-α/IL-2, or IFN-γ/TNF-α/IL-2 were determined in a similar way.

Intracellular cytokine staining (ICS) gating strategy. The gate matching the pool of lymphocytes was chosen at the FS/SS diagram
A positive T cell response required the acquisition of 50,000 CD3+ lymphocytes, and the frequency of cytokine-producing T cells in antigen-stimulated cells had to be at least twice that of nonstimulated cells. 29,30
Statistical analysis
ELISpot data analysis was made using the DFR (2x) method (
Results
Sociodemographic and biomedical characteristics of the study population
Nine seronegative IDUs, 10 seronegative non-IDUs, and nine of their HIV-positive sexual and/or IDU partners from the cohort of IDUs were included in the study. Table 1 summarizes the sociodemographic and biomedical characteristics of 28 enrolled individuals. Seven out of 19 (37%) ESN individuals were female. All discordant couples had unprotected sex, and some of seronegative partners also had parenteral exposure. Eight (42%) ESN individuals had on average above 100 unprotected sexual contacts per year and six (31%) had sexual risk between 10 and 60. Six (31%) had an experience of shared injection paraphernalia within the last 3 months. Although 2 (10%) individuals reported no risk behavior they were also enrolled because of possible underestimation of their reported risks.
All ESNs were negative by ELISA and Western blot, as well as negative for HIV-1 RNA by RT PCR. Repeat ELISA was conducted for some patients (Table 1) after enrollment and confirmed that they were still seronegative.
HIV-1-specific T cell responses by ELISpot assay
The summarized ELISpot data are presented at Fig. 2 and Table 2. Thirteen out of 19 (68%) seronegative study subjects had strong Nef peptide pool-specific cellular immune responses, three out of 19 (16%) subjects responded against the Gag peptide pool, and one subject had an RT peptide pool response. The median (range) of SFU per 106 PBMCs in ESN subjects was 76.7 (21–615) in Nef, 11.7 (0–235) in Gag, 4.24 (0–31) in RT, and 1 (0–30) in Env. In the case of the Nef pool the median (range) of SFU per 106 for six subjects who demonstrated negative response was 38 (21–95) and for 13 subjects who demonstrated a positive response was 87 (50–615). For seropositive partners the medians of the counts were 428 (63–4382), 645 (166–5172), 386 (50–2609), and 222 (11–2418) in Nef, Gag, RT, and Env, respectively. Spot counts were not significantly different (p>0.05, Dunn's multiple comparison test) between the groups of ESN and seropositive subjects for the Nef response, but were significantly higher in seropositive subjects than in ESN for responses against peptides of three other proteins (Fig. 2).
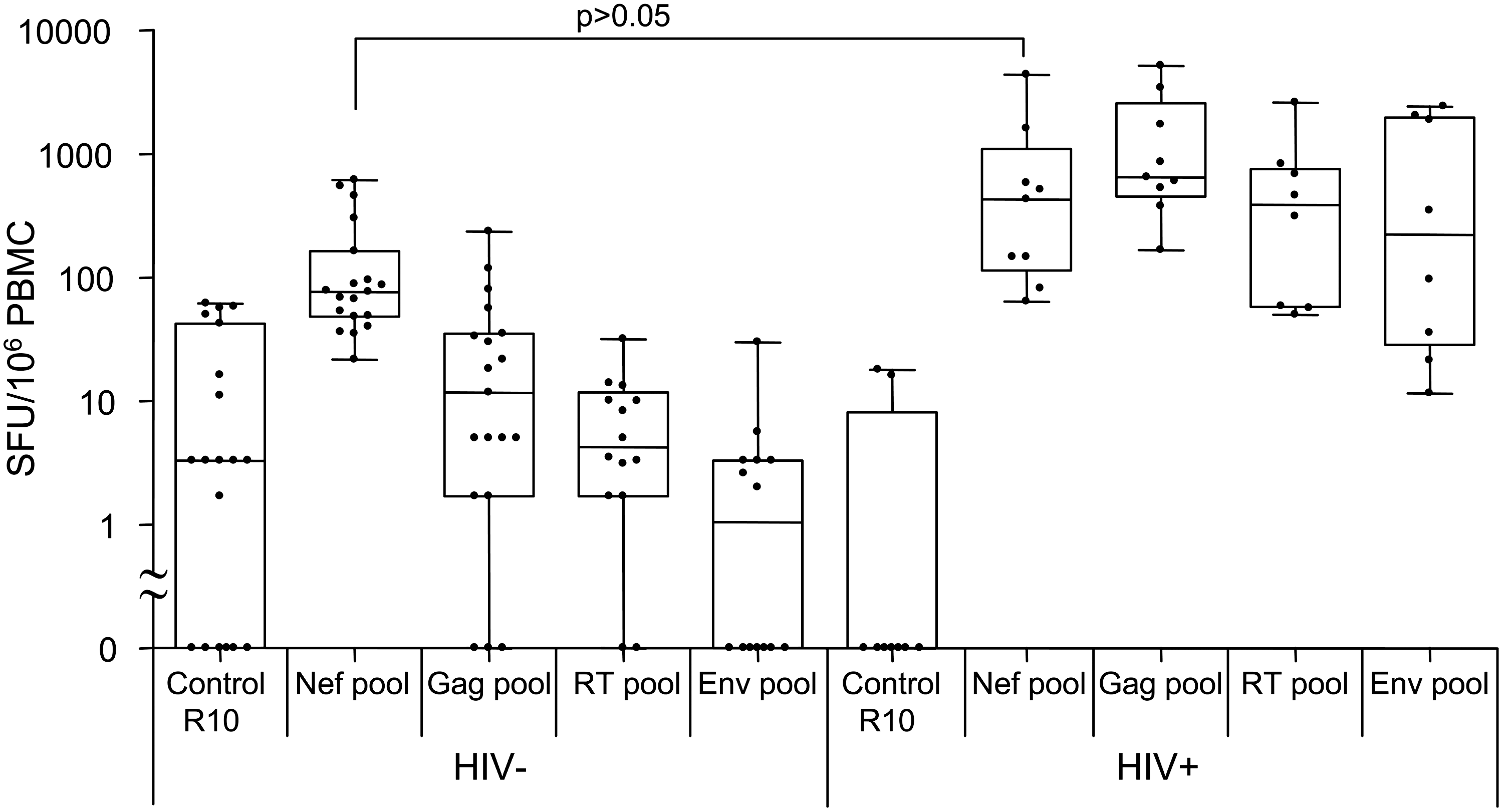
IFN-γ ELISpot results. Peripheral blood mononuclear cells (PBMCs) of the exposed seronegative (ESN) and HIV-positive donors were stimulated with Nef, Gag, RT, and Env peptide pools. The number of spot-forming units (SFU) per 106 PBMCs was calculated.
(+) p≤0.05 in the DFR(2×) method; (−) p>0.05 in the DFR(2×) method.
n/a, not analyzed.
Multiple cytokine production by CD4+ and CD8+ cells by ICS assay
Identification of several cytokine (IFN-γ, TNF-α, IL-2) production and determination of HIV-specific CD4+ and CD8+ producing T cells were performed by ICS in nine seronegative (Table 3) samples and in five HIV-positive samples, where the cells were available. We observed that CD3+CD8+ lymphocytes of the seronegative patients responded to stimulation with Nef-pool by IFN-γ expression in one subject out of nine, by TNF-α expression in five subjects, and by IL-2 in two subjects; to stimulation with Gag-pool by IFN-γ expression in two out of five subjects, by TNF-α expression in three subjects, and by IL-2 in one subject. CD3+CD4+ lymphocytes were found to express IFN-γ in four subjects, TNF-α in eight subjects, and IL-2 in five subjects after stimulation with Nef-pool; and to express IFN-γ in three subjects, TNF-α in two subjects, and IL-2 in one subjects after stimulation with Gag-pool (Fig. 3 and Table 3).
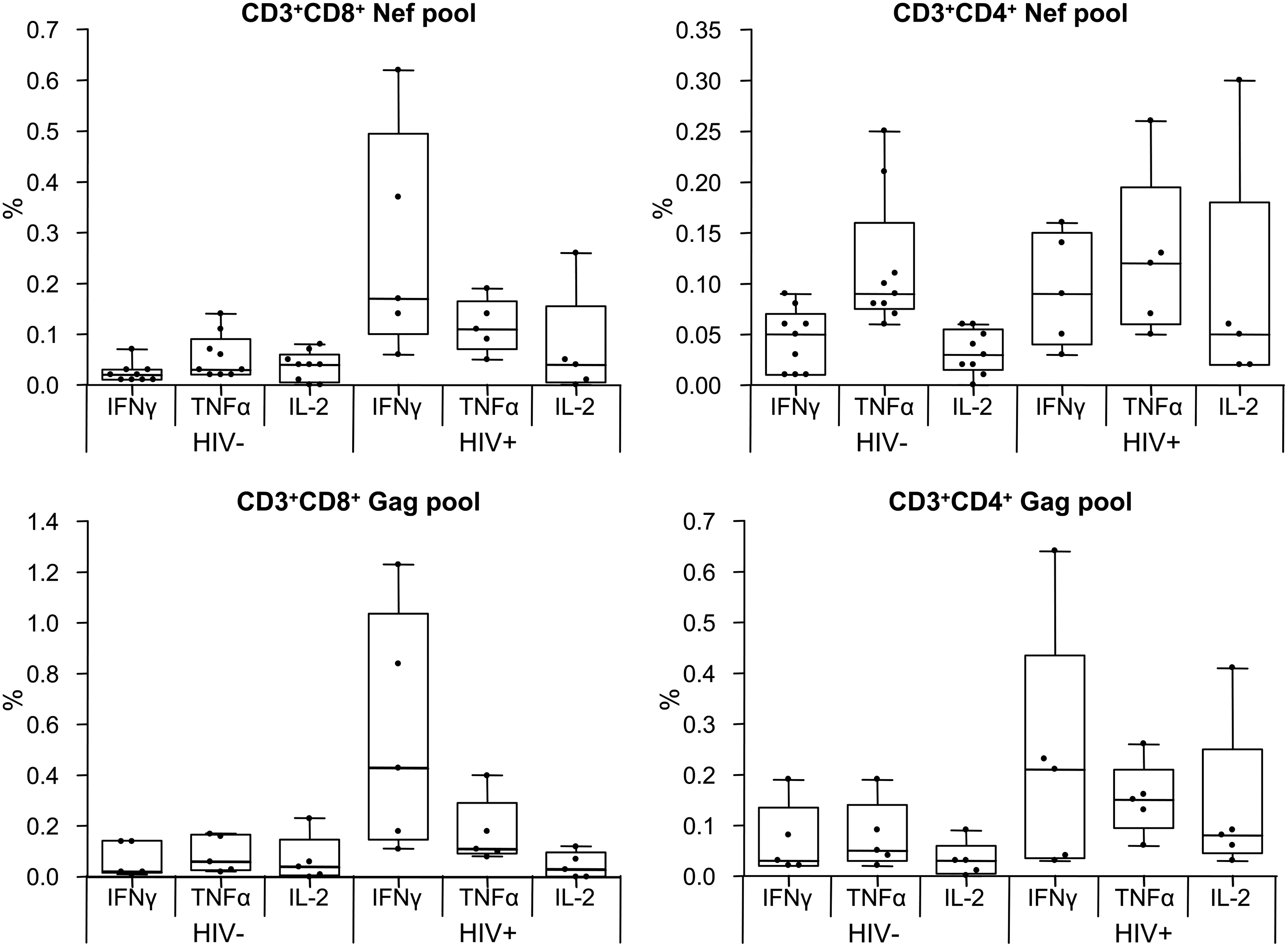
ICS results. PBMCs were stimulated with Nef and Gag peptide pools and stained with fluorochrome-conjugated monoclonal antibodies (mAbs) for surface markers (CD3, CD4, CD8) and intracellular antigens (IFN-γ, TNF-α, IL-2). Results are presented as percent of IFN-γ-, TNF-α-, or IL-2-producing CD3+CD4+ or CD3+CD8+ cells.
(+) 50,000 or more CD3+ lymphocytes were analyzed, and the frequency of cytokine-producing T cells in antigen-stimulated cells was at least twice that of nonstimulated cells.
IFN, interferon; TNF, tumor necrosis factor; IL, interleukin; n/a, not analyzed.
The functional profiles of the immune responses were different between the ESN group and the HIV-positive group (Fig. 4). Thus, it was shown, that CD3+CD8+ and CD3+CD4+ lymphocytes of the ESN subjects responded preferably with TNF-α expression. At the same time the CD3+CD8+ lymphocytes of the HIV-positive subjects preferably expressed IFN-γ. In the ESN group the CD8 response to Nef-pool was found to be more multifunctional than to Gag-pool, and the CD4 response was found to be more multifunctional to Gag-pool than to Nef-pool; in the HIV-positive group the multifunctionality of the response did not depend on peptide pools for both T cell populations.
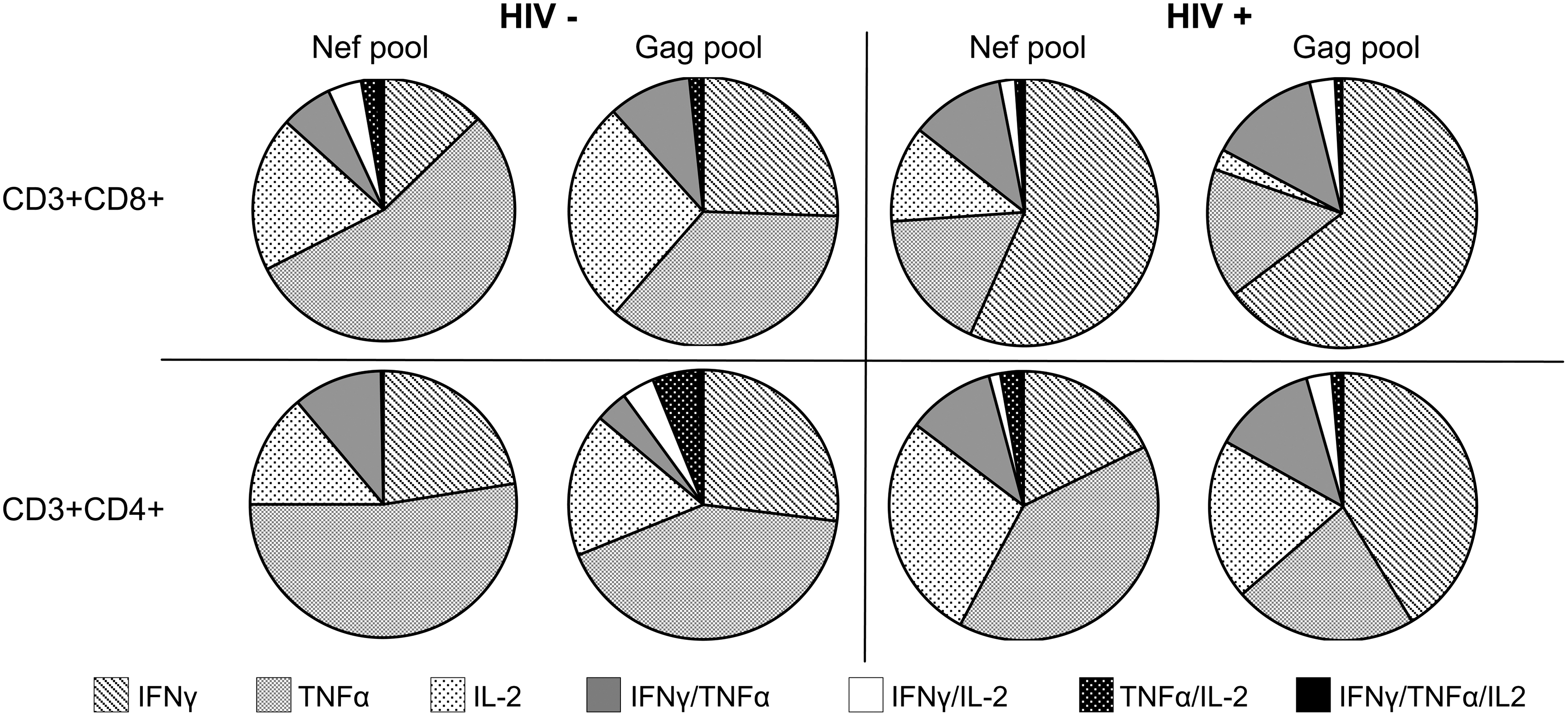
ICS results. The functional profiles of CD3+CD8+ and CD3+CD4+ immune responses induced in ESN and HIV-positive individuals after stimulation with Nef and Gag peptide pools.
Discussion
Individuals who remain uninfected despite repeated exposure to HIV are of great interest. In light of the progressive spread of the HIV epidemic and the lack of an effective vaccine it is increasingly important to evaluate potential determinants of this protection.
In our study we observed T cell immune responses in seronegative individuals exposed sexually and parenterally. Since it was shown previously that both types of exposure induced T cell responses with similar magnitude and breadth, 18 we did not divide the patients into different groups according to types of exposure risk. Some patients had both types of risks. Only two patients were found to be heterozygous for the CCR5Δ32 mutation (Table 1); the rest had the wild-type allele. So we could exclude the influence of this deletion on the susceptibility to HIV infection in our study group.
We observed a high rate (65%) of HIV-specific T cell immune responses in ESN patients. The blood samples of 21 nonexposed seronegative individuals were analyzed later and they demonstrated no HIV-specific T cell immune responses. 31 The majority of ESN patients had the responses in IFN-γ ELISpot against Nef. For some patients (if the cells were available) we also performed ICS and observed a multiple cytokine production against Nef and Gag peptides, and more often the immune response was mediated by CD3+CD4+ cells. It is noteworthy that 100% of the study subjects demonstrated TNF-α production by CD4+ cells after stimulation with the Nef peptide pool. In three cases we did not detect IFN-γ production in ICS, though we detected it in ELISpot; this corresponds to previous findings that the ELISpot assay is more sensitive than the flow-based assay. 32 Additionally, in spite of a lack of HIV antibodies in commercial ELISA tests, we observed in some individuals antibodies against Nef in ELISA using recombinant Nef protein, though in low titers (data not shown).
Our observations correspond to the results of the previous studies, 4,13,15 –17,30 in which ESNs were found to have T cell immune responses against Nef, but we show for the first time the high frequency of such a response. Early immunologic studies 8 demonstrated the reactivity of the CTL precursors against Nef in all six studied (100%) uninfected heterosexual contacts of HIV-infected patients. Recently Ritchie and co-authors failed to detect any response in ex vivo ELISpot in highly exposed seronegative individuals, but after additional culture of the PBMCs demonstrated T cell immune responses in 61% of patients. 30
It is noteworthy that in most cases with ELISpot measured T cell response against Nef it was absent against other proteins. Nef is a protein, which presents in HIV virions in a minor amount (comparing to Gag and Env). 33 It is expressed in a latent phase of the infection from fully spliced mRNA, when the expression of other proteins is almost absent. Some authors assumed that this response could be triggered by translation of unintegrated HIV-DNA. 16 Hence, based on our results, we could suggest that the observed immune responses were induced by the transient infection of the host cells with HIV. Concerning the fact that these patients remained HIV negative, we could assume that the infected cells were cleared by the immune response. It means that this response may be protective. We could also suppose that initially infected cells formed “latent reservoirs” in patients, which were targeted by the observed Nef-specific immune response. Probably this could be a more universal principle of HIV pathogenesis. We could make a similar suggestion analyzing the results of other investigators who demonstrated early escape mutations in the Nef gene in the acute phase of infection. 34 On the other hand, the observed immune responses could be caused by an alternative pathogen circulating among IDUs in St. Petersburg, Russia, whose immunological determinants overlap the HIV-1 Nef epitopes. This hypothesis is supported by the earlier findings that T lymphocytes of donors noninfected and unexposed to HIV-1 contain Nef-specific cytotoxic T lymphocyte precursors at high frequency. 35,36
In both cases observed cellular responses may be protective at least against some HIV variants, and it can work as a barrier for viral infection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.