
Abstract
HIV-1 genetic diversity of recently seroconverting (<12 months) Thai repeated blood donors attending the National Blood Centre, Thai Red Cross Society (NBC, TRCS) from September 2007 until March 2008 was assessed. Ten HIV-1 recent seroconvertors (10/239,134 donations) were identified during the study period. The estimated median time to seroconversion was 67.3 days (range: 45.5–102.0 days), and viral load ranged from 307 to 341,805 copies HIV-1 RNA/ml. MHAbce, a real-time-based PCR genotyping assay, identified six CRF01_AE, two CRF01_AE/B recombinants, one subtype B, and one CRF01_AE/B dual infection. Nine samples were further characterized by full genome sequencing, identifying CRF01_AE (N=6), unique CRF01_AE/B recombinants (N=2), and subtype B (N=1). One recombinant contained 13 breakpoints located in gag, pol, vif, vpr, env, and nef while the other recombinant contained 10 breakpoints located in pol, vif, env, and nef. This study found two unique CRF01B recombinants circulating in 10 recent HIV-1-positive subjects from a blood donor population in Thailand.
Introduction
C
In the HIV-1 pandemic to date, numerous viral strains have been documented and categorized into nine different subtypes (A, B, C, D, F, G, H, J, and K) and 51 circulating recombinant forms (CRFs). 5,6 In high-risk populations, high HIV-1 prevalence with multiple subtype distribution and the emergence of new recombinant strains are usually observed. 1,5 Low-risk populations with presumably lower HIV-1 prevalence demonstrate less genetic diversity compared to high-risk populations within the same geographic region. 7 Blood donors are considered low-risk populations due to prescreening and refusal of donors who report high-risk behavior. The WHO Global Database on Blood Safety 2004–2005 reported diverse HIV-1 prevalence in blood donations according to the human development index (HDI): 0–0.72% in 43 high HDI countries, 0–6% in 65 medium HDI countries, and 0.04–11.00% in 21 low HDI countries. 8 Despite the increase in global blood safety policy regulations, new HIV-1 infections due to blood transfusion are still present in some areas: 12% in Saudi Arabia, 9 6.2% in Egypt, 10 and 0.2% in sub-Saharan Africa. 11
Thailand, a medium HDI country centrally located in Southeast Asia, is the only country in Asia reporting a national HIV-1 prevalence as high as 1% in 2009. 1,12,13 CRF01_AE and subtype B (Thai and U.S. variants) 14,15 are the predominant HIV-1 strains circulating in Thailand. The intermixing between these strains has generated novel CRFs, including CRF15_01B, CRF33_01B, CRF34_01B, CRF48_01B, and CRF51_01B and unique recombinant forms (URFs) that have been identified in high-risk groups such as sex workers, men having sex with men, and injecting drug users within the past decades. 14 –23 Thailand adheres to the WHO blood safety protocol and achieved nationwide blood-borne disease screening of blood donations in 2009. 8 In addition, HIV-1 infection due to blood transfusion was reported to be 0.02% from 1984 to 2011 with 0% observed within the past 5 years. 24 The trend of HIV-1 seroincidence in repeat blood donors declined from 0.3% in a 1996 cohort study 25 to 0.13% in 2009. 26 Nonetheless, the magnitude of HIV-1 molecular diversity and the subtypes/CRF distribution in the Thai blood donor population have not been well characterized.
In this study, we evaluated the HIV-1 circulating strains in a major blood donor population at the NBC, TRCS, a blood bank located in Bangkok. The HIV-1 sequences derived from these recent seroconverters indicated the genetic complexity of circulating HIV-1 strains in this low-risk Thai blood donor population.
Materials and Methods
Study samples
Nonpaid blood donations with consent were collected at the NBC, TRCS. Individuals with HIV-1 risk behaviors were screened out during predonation counseling. Blood donations were labeled with identification numbers assigned to individual donors without any personal identifying information, excluding age and gender. Blood donations were identified as HIV-1-seronegative donations following negative results from anti-HIV-1 ELISA Vironostika (bioMerieux, Marcy l'Etoile, France), Prism (Abbott, Abbott Park, IL), and Determine (Abbott, Abbott Park, IL), and also negative results from HIV-1 nucleic acid-based tests by Procleix Assays (Novartis, Emeryville, CA) and Cobas TaqScreen MPX (Roche, Basel, Switzerland). HIV-1-seropositive donations were identified when test results from anti-HIV-1 ELISA Vironostika, Prism, and Determine were positive. This study identified HIV-1-positive donors from September 2007 to March 2008 who had a previous HIV-1-seronegative blood donation within the previous 12 months. Plasma was separated from whole blood of subjects testing HIV-1 seropositive within 24 hr of blood collection. The study was approved by the Institutional Review Board (IRB) from Chulalongkorn University, Bangkok, Thailand and was determined nonhuman subjects research by the IRB from Walter Reed Army Institute of Research (WRAIR).
Specimen characterization
Viral load in HIV-1-seropositive samples was measured by an automated, high-throughput m2000 system (Abbott Park, IL). The multiregion hybridization assay (MHA)bce, a real-time-based assay designed for subtypes B, C, and CRF_01AE, was used for subtype prescreening on the HIV-1-seropositive samples as previously described. 20,27 Briefly, RNA was extracted from plasma samples using the QIAamp Viral RNA Mini Kit (QIAGEN, Valencia, CA). One sample, MERLBDTRC1 (Table 1), with a viral load of 307 HIV-1 RNA copies/ml, was extracted using NucliSens (bioMerieux, Marcy l'Etoile, France) to concentrate RNA prior to conducting the MHAbce procedure. The extracted RNA was then reverse transcribed and PCR amplified by the QIAGEN OneStep RT-PCR kit (QIAGEN, Valencia, CA). Fluorescence intensity from probes in the real-time PCR-based assay was analyzed using SDS v2.1 software (Applied Biosystems, Foster City, CA). HIV-1-seropositive and HIV-1-seronegative samples were processed throughout the RNA extraction and amplification procedures for quality control.
Negative results from Vironostika, Prism, Determine, Procleix, and Cobas TaqScreen MPX.
Positive results from Vironostika, Prism, and Determine.
Estimated seroconversion time: the median time between the last HIV-1-seronegative donation and the first HIV-1-seropositive donation.
Sequencing, phylogenetic analysis, and drug resistance profile analysis
All samples with the exception of MERLBDTRC1 were further characterized by nearly full-length sequencing as described previously. 16 HIV-1 full-and half-length genome cDNA were generated from extracted RNA using the ThermoScript RT-PCR System (Invitrogen, Carlsbad, CA) with uninef-7 and JL68R, respectively (Table 2). The cDNA was subjected to nested PCR at the near end-point dilution using primers MSF12B/UNINEF7′ and nested with GAG763 /TATANEF to retrieve the HIV-1 full-length genome. Briefly, nested PCR reactions were performed with serial dilutions of each cDNA template. The PCR products obtained from the lowest dilution of cDNA template were selected for further analysis by sequencing. The 5′ end half-length HIV-1 DNA was amplified using primers MSF12B/JL68R and nested with GAG763/TAT-B′. The 3′ end half-length HIV-1 DNA was amplified using primers POLJV2 /UNINEF7 and nested with POLK3 /TATANEF. The PCR amplifications were conducted with either the Expand Long Template or Expand Long Range dNTPack (Roche, Indianapolis, IN) following the same conditions of the near end-point dilution procedure as previously described for near full-length and half-length HIV-1 genome amplification. 28,29
PCR products were purified and sequenced with Big Dye terminators using an ABI 3130XL capillary sequencer (Applied Biosystems Inc., Foster City, CA), as described. 30 Sequencher 4.7 (Gene Codes Corp., Ann Arbor, MI) was used to analyze, edit, and assemble sequences. 30 A multiple alignment of the new sequences with the following reference sequences was constructed: A_ A173, A_ MSA4072, B_US_ SF2, B_US_MN, B_US_5018, B_TH_C3198, B_TH_M081, C_93IN905, C_97TZ05, D_NDK, D_ELI, 01_TH_CM240, 01_TH_CM244, 01_TH_TH253, 01_CN_CNGX2F, F_FIN9363, F_VI850, G_G6165, G_HH8793, H_VI991, H_056, J_SE9280, J_SE9173, K_EQTB11, K_MP535, 15_OUR1331, 15_OUR1332, 33_05MYKL031, 33_05MYKL045, 34_OUR1969P, and 34_OUR2478P. 5 Phylogenetic analysis was performed using SEQBOOT, DNADIST, NEIGHBOR, and CONSENSE modules of the MacGDE v.2.4 software and DIVEIN. 31 Each sequence and each segment was analyzed by building a phylogenetic tree using the neighbor-joining method, 32 and the stability of the nodes was assessed by bootstrap analysis. 33 Bootstrap values of 70% or greater were used to confirm the subtype assignment. Maximum likelihood trees were also constructed and genetic distances were analyzed by DIVEIN. 31 Breakpoints for the recombinant sequences were analyzed by the jumping hidden Markov model (JpHMM) tool 34 and precisely mapped by visual inspections, comparing them with six B subtypes (B_MN, B_LAI, B_OYI, B_RF, B_SF2, B_RL42) and six CRF01_AE (01_CF402, 01_CM240, 01_TH253, 01_97CNGX, 01_90CF402, 01_90CF11697). Sequence characteristics and drug resistance profiles were generated using the Stanford University Drug Resistance Database 35 and HIV Sequence Database, 5 respectively.
Results
From September 2007 to March 2008, NBC, TRCS collected 290,360 blood donations, which included 51,226 new blood donations and 239,134 repeated donations. The frequency of HIV-1-positive blood donations was 0.09% (272/290,360 donations) for total blood donations, 0.32% (164/51,226 donations) for new blood donations, and 0.04% (108/239,134 donations) for repeat blood donors. Repeat blood donors had a lower HIV-1 prevalence than new blood donors (p<0.001). Ten donations from the repeat blood donors were considered recent seroconvertors with 0.004% HIV-1 prevalence (10/239,134 donations) during the study period.
Demographic characteristics including age, sex, sample collection dates of last HIV-1-negative donations and the first HIV-1-positive donations, estimated duration of seroconversions, and viral load are presented in Table 1. The recent seroconvertors were seven males and three females with a median age of 33 years (range: 22–54). The estimated median time to seroconversion (median time between the HIV-1 seronegative and seropositive blood donation) was 67.3 days (range: 45.5–102.0 days). The median viral load of the donors was 90,725 copies HIV-1 RNA/ml (range: 307–561,022). There was no correlation between the estimated time from infection and the plasma viral load (Spearman rank correlation, r 2 =−0.073, p=0.838), although the sample size is limited.
Plasma samples from the 10 subjects were prescreened by MHAbce v.2 and their subtype results showed nine HIV-1 single infections and one CRF01_AE/B dual infection (Table 3). The dual infection CRF01_AE/B was identified from dual probe reactivities detected in subject MERLBDTRC1, from which the plasma RNA was concentrated 10-fold to approximately 3070 copies HIV-1 RNA/ml prior to performing the MHAbce. This viral strain had both subtype B and CRF01_AE probe reactivity in the int region while only subtype B probes reacted throughout the other regions.
Unique mutations are defined by unusual mutations (have not followed the general polymorphic or observed in a particular location).
MHAbce detected dual probe activities of CRF01_AE and B subtypes and is defined as CRF01_AE/B dual infection.
Viral load is below the detection limit for molecular analysis by full-length sequencing.
The genome contains insertions of subtype B in the majority of the CRF01_AE subtype and is defined as CRF01_AE/B recombinant.
X: stop codon indicating truncated proteins (position of proteins).
None of these minor mutations is included in the recommended mutations for drug resistance surveillance.
L10V: L10I/V is found in 5–10% of naive individuals. L10I/V/F/R/Y is also associated with resistance to most protease inhibitors, atazanavir, fosamprenavir, indinavir, lopinavir, nelfinavir, and saquinavir when present with other mutations.
V151I
V179D shows reduction in the susceptibility of each nonnucleoside reverse transcriptase inhibitor (delavirdine, efavirenz, etravirine, nevirapine) by about 2-fold.
The subtypes obtained by full-length sequencing were in concordance with subtypes identified by MHAbce: 6/9 CRF01_AE, 2/9 CRF01_AE/B recombinant, and 1/9 subtype B (Table 3). Phylogenetic analysis revealed that MERLBDTRC 2, 4, 5, 7, 8, and 9 were clustered closely to those CRF01_AE strains previously identified in Thailand and China at 96% bootstrap values (Fig. 1). The mean value of genetic distance of the full-length genomes among these six strains was approximately 7.8% (range: 6.3–9.0%). MERLBDTRC10 clustered with subtype B reference strains at a bootstrap value of 100%. The majority of the genome of MERLBDTRC10 was identified as U.S. HIV-1 subtype B by visual inspection with a small insertion of subtype D genetic material in the gag region from HXB2 numbering sequence 1869 to 1985. Neither drug resistance profiles nor unique mutations in the genome were shared among the HIV-1 strains in the 10 blood donors (Table 3). Minor drug resistance mutations, which are not on the list of recommended mutations for drug resistance surveillance, were found in three subjects: L10V in pr of MERLBDTRC 4, V151I in int of MERLBDTRC 6, and L10V in pr & V179D in rt of MERLBDTRC 8. The possible APOBEC 3G/F-mediated hypermutation 36 was observed in MERLBDTRC 7, which resulted in a premature stop codon (W71X) at pol 226 and nonsynonymous D186N mutation in the rt region of MERLBDTRC 9 (Table 3).
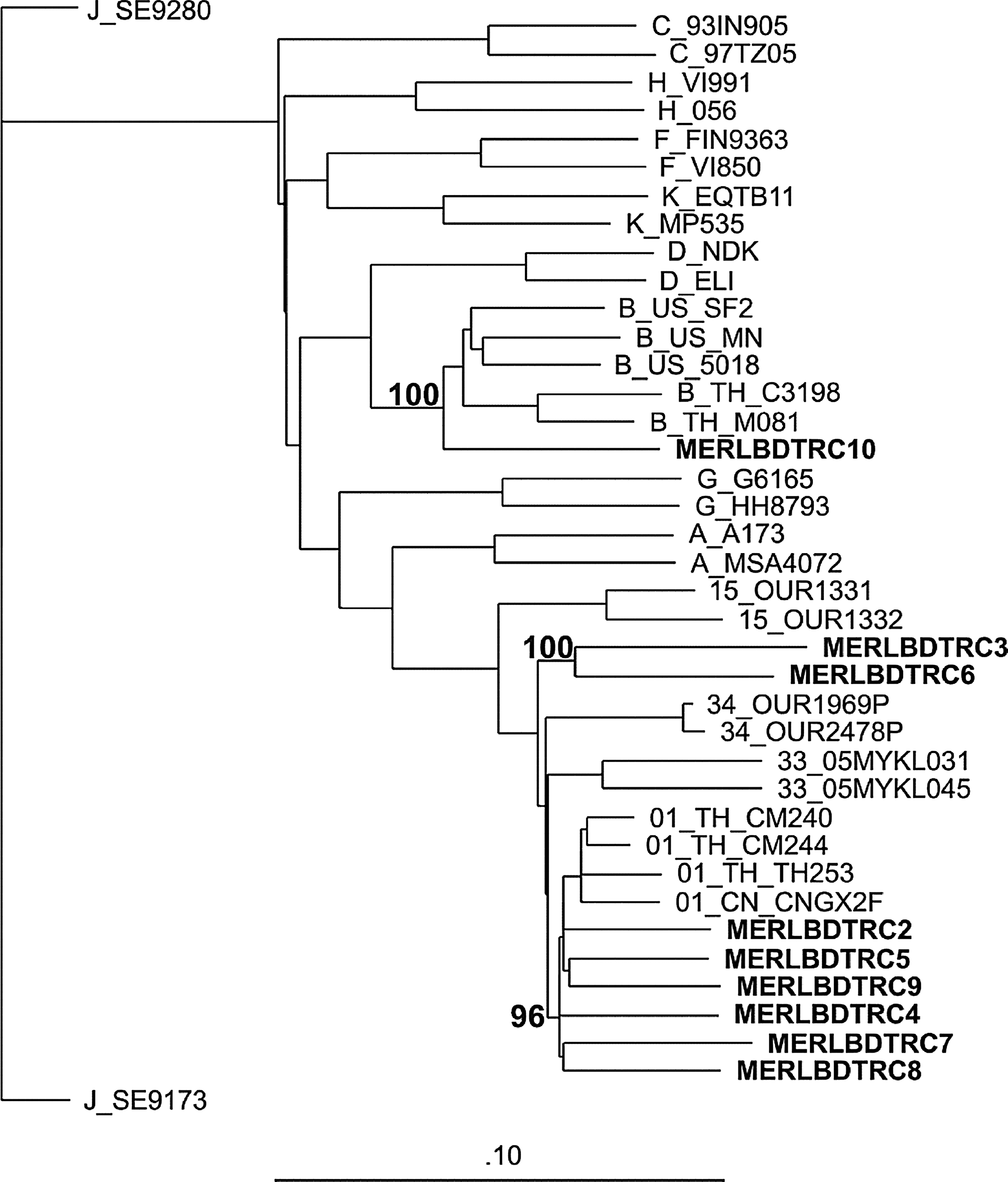
Phylogenetic analysis of MERLBDTRC 2-10. A neighbor-joining tree was constructed. Bootstrap values were placed at the nodes of the tree and the scale bar indicates 10% genetic distance.
MERLBDTRC 3 and MERLBDTRC 6 clustered together with a bootstrap value of 100% but separated from CRF01_AE, CRF15_01B, CRF33_01B, and CRF34_01B. Visual inspection and phylogenetic analysis of two sequence alignments with CRF01_AE and subtype B references suggested that these two samples were CRF01_AE/B recombinants (Figs. 1 and 2). Their genomic subtype structures were different in their breakpoints as seen in Fig. 2A. MERLBDTRC 3 contained 13 breakpoints located at gag, pol, vif, vpr, env, and nef. MERLBDTRC 6 contained 10 breakpoints located at pol, vif, env, and nef.
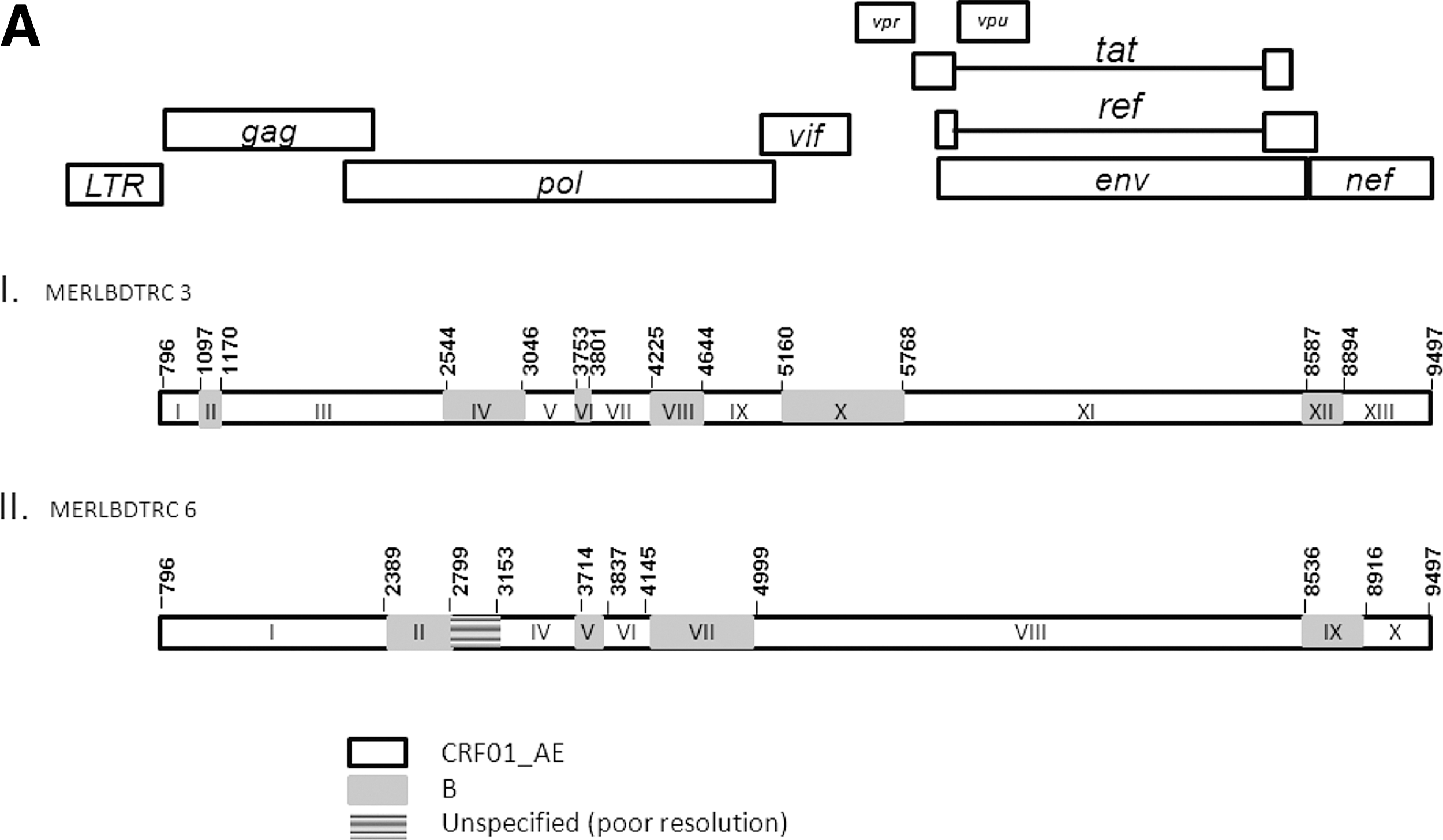
Phylogenetic analysis of MERLBDTRC 3 and 6.
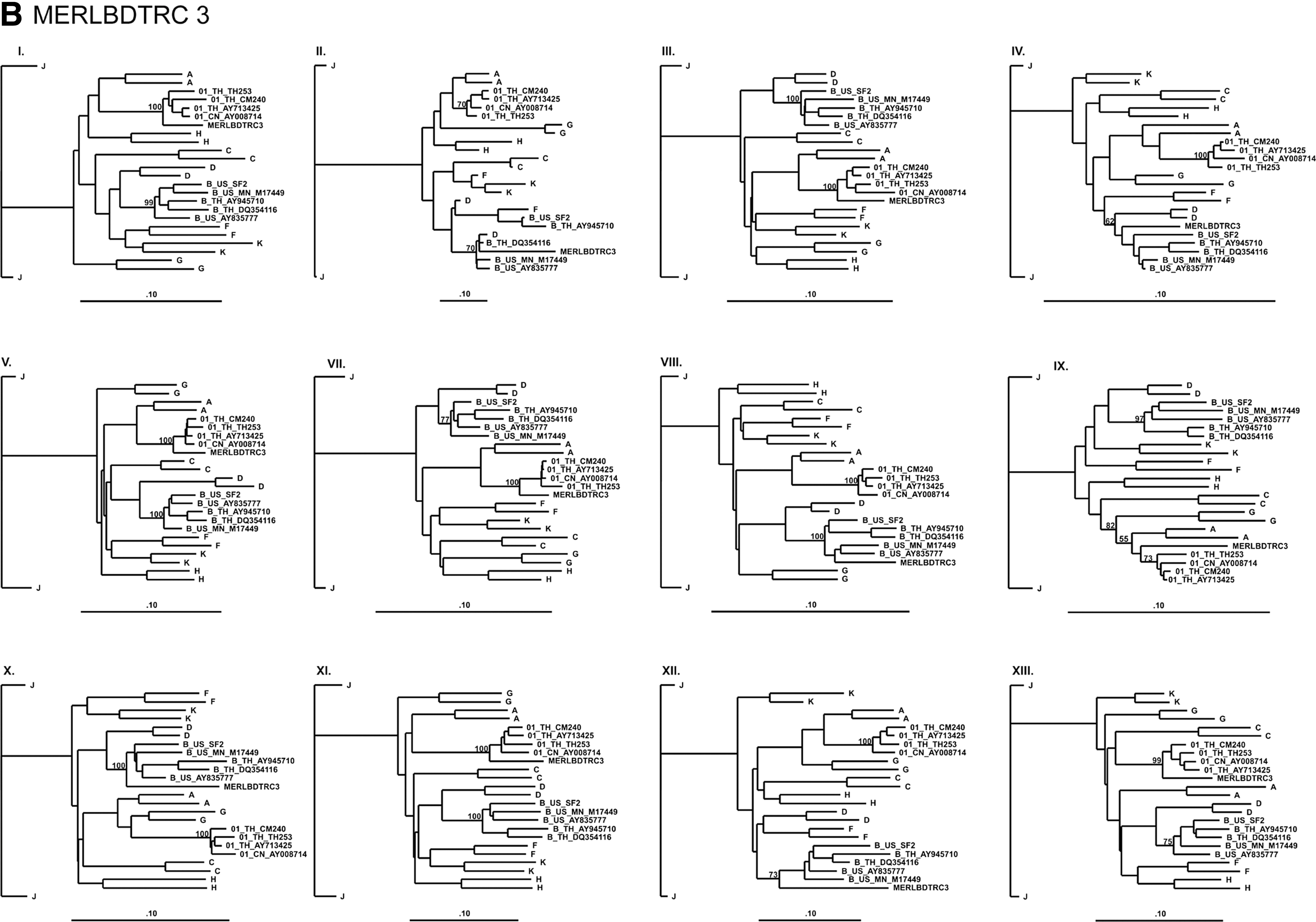

Phylogenetic analysis of the subregional trees in Fig. 2B and C further confirmed subtype shifts in two recombinant HIV-1 strains. Some problematic regions in the genomic structure of MERLBDTRC 3 and 6 were identified as “poor-resolution” (Fig. 2A.II and C.III) or the sequences were too short (Fig. 2B.IV, B.VI, and C.V) to provide sufficient data for the analysis. In comparison to the CRF01_AE/B recombinants in the published HIV Sequence Database, 5 the patterns of recombination between CRF01_AE and subtype B in MERLBDTRC 3 and 6 suggest that they are newly identified unique recombinant forms (URFs).
Discussion
Our preliminary assessment on blood donations collected from September 2007 to March 2008 at the NBC, TRCS revealed a low prevalence of HIV-1 in total blood donations and repeated blood donors, which are approximately 15-fold and 35-fold lower, respectively, than the 1.4% HIV-1 prevalence reported for the Thai general population in 2007. 37 Compared to a developed or high HDI country from 2004 to 2008, the frequency of HIV-1 seroconversion at the NBC, TRCS, Bangkok, was 0.1% or 36-fold higher than the frequency of HIV-1 seroconversion observed in blood donations collected nationwide by the American Red Cross. 38 Nonetheless, the prevalence of HIV-1 in Thai blood donors in 2007 was 0.27%, slightly higher than the 0.23% HIV-1 prevalence in the regional WHO Southeast Asian blood donors. 39 Furthermore, Thailand demonstrated the largest reduction (5-fold) in HIV-1 prevalence in blood donors compared to the general population when compared with Myanmar (1-fold), Indonesia (3.7-fold), and eight other countries (1- to 2.5-fold) in Southeast Asia. 39,40 Lastly, no HIV-1-infected cases via blood transfusion were reported nationwide in 2007 and 2008. 41
The NBC, TRCS has successfully applied the WHO safety blood protocols and closely monitored HIV-1 and other blood-borne diseases including syphilis, HBV, and HCV since 2000. The low frequency of HIV-1 seroconversion (0.2%) in the blood donor population at the NBC, TRCS suggested successful implementation of the WHO blood safety policy. In addition, the strategy of collecting blood from nonpaid volunteers as well as the honor system for prescreening high-risk factors by questionnaire could have contributed to the lower HIV-1 prevalence in blood donations compared to that in the general population. This observation also reflects the high standard of the NBC, TRCS as one of the WHO collaborating Centers for Southeast Asia regional quality control, blood transfusion services. 40
The HIV-1 subtype distribution in Thailand is predominantly CRF01_AE, followed by non-CRF01_AE subtypes consisting of subtype B, CRF_01, and B recombinants and dual infection with CRF01_AE and subtype B as reported from an antenatal community study, 20 a vaccine trial cohort, 21 and high-risk populations. 16,17,27 With the caveats imposed by a small sample size, the subtype diversity of HIV-1 found in repetitive blood donors at the NBC, TRCS may suggest dynamic interactions across risk groups and a possible bridging between high- and low-risk populations. These findings suggest dynamic interactions across risk groups in Thailand as our study identified two recombinant forms between CRF01_AE and B along with pure subtypes despite a small size of 10 blood donors. Similar observations of diverse HIV-1 subtype distribution in blood donor populations with low HIV-1 prevalence have also been reported in Cameroonian and Tanzanian blood donors. 7,42 In addition, the two newly identified CRF_01B recombinant forms contain unique recombination patterns with high numbers of breakpoints, and they differ from other recombination forms reported in the HIV Sequence Database. 5 These HIV-1 recombinants were identified in 22- and 29-year-old males. On-going recombination between CRF01_AE and subtype B has been reported in other countries in Southeast Asia such as Malaysia, 18,43 Singapore, 44 and China. 45
Minor mutations possibly associated with resistance to protease inhibitors, reverse transcriptase inhibitors, and integrase inhibitors were detected in this cohort (Table 3). They were identified as polymorphisms that were occasionally found in antiretroviral-naive patients and also in high-risk cohorts. Although most minor mutations have not been shown to have a direct association with drug resistance in clinical settings, some minor mutations have the potential to confer drug resistance when combined with other mutations. 46 Therefore, monitoring the existence of these minor mutations provides genetic background that may lead to information on drug resistance that may improve future antiretroviral treatment.
The diversity of HIV-1 circulating strains in our study provides insight concerning HIV-1 in the Thai blood donor population. The emergence of novel HIV-1 strains identified in this low-risk cohort and the continuing diversification of the Thai epidemic emphasize the importance of HIV-1 molecular surveillance in the design and testing of preventive HIV-1 vaccines and in providing a basis for sound public health policy.
GenBank Accession Numbers
The nine sequences, MERLBDTRC2 to MERLBDTRC10, have been submitted to GenBank under accession numbers JN860761 to JN860769, respectively.
Footnotes
Acknowledgments
We would like to thank LTC Viseth Ngauy, Dr. Joseph Chiu, Ms. Rapee Trichavaroj, the molecular laboratory, and the Department of Retrovirology, AFRIMS, for support and advice on the study. We would like to extend our thanks to Dr. Gustavo Kijak, Dr. Morgane Rolland, Mr. Eric Sanders-Buell, and the Division of Molecular Virology and Pathogenesis, MHRP, Rockville, Maryland for technical support and assistance. In addition, we would like to thank Dr. Soisaang Phikulsod, director of NBC, TRCS, Blood Testing section, Registration and Statistic section at the National Blood Centre, Thai Red Cross Society, for database information.
This work was supported by funding provided by the Military Infectious Diseases Research Program (MIDRP) through a cooperative agreement (W81XWH-07-2-0067) between the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., and the U.S. Department of Defense (DOD). The views and opinions expressed herein do not necessarily reflect those of the U.S. Army or the Department of Defense.
In addition, part of this work was supported by the Higher Education Research Promotion and National Research University Project of Thailand (HR1161A5), Office of the Higher Education Commission.
Author Disclosure Statement
No competing financial interests exist.