
Abstract
We analyzed antiretroviral drug susceptibility in HIV-infected adults failing first- and second-line antiretroviral treatment (ART) in Rakai, Uganda. Samples obtained from participants at baseline (pretreatment) and at the time of failure on first-line ART and second-line ART were analyzed using genotypic and phenotypic assays for antiretroviral drug resistance. Test results were obtained from 73 samples from 38 individuals (31 baseline samples, 36 first-line failure samples, and six second-line failure samples). Four (13%) of the 31 baseline samples had mutations associated with resistance to nucleoside or nonnucleoside reverse transcriptase inhibitors (NRTIs and NNRTIs, respectively). Among the 36 first-line failure samples, 31 (86%) had NNRTI resistance mutations and 29 (81%) had lamivudine resistance mutations; only eight (22%) had other NRTI resistance mutations. None of the six individuals failing a second-line protease inhibitor (PI)-based regimen had PI resistance mutations. Six (16%) of the participants had discordant genotypic and phenotypic test results. Genotypic resistance to drugs included in first-line ART regimens was detected prior to treatment and among participants failing first-line ART. PI resistance was not detected in individuals failing second-line ART. Surveillance for transmitted and acquired drug resistance remains a priority for scale-up of ART.
Introduction
A
Recent reports from Uganda and other countries in sub-Saharan Africa have reported increasing levels of acquired and transmitted drug resistance with 11.6% transmitted drug resistance reported from Kampala, highlighting the importance of ongoing monitoring and surveillance as the second decade of ART expansion approaches. 3;7 –9 Very little information is available on drug resistance in rural communities in sub-Sarahan Africa, and no data are available on drug resistance in rural Uganda. The goal of this study was to gain insight into the patterns and frequency of ART resistance in a rural treatment cohort in Rakai, Uganda. In a previous study we evaluated antiretroviral drug susceptibility in ART-naive individuals in the RHSP prior to the availability of ART. We found that some individuals had viruses with reduced phenotypic antiretroviral drug susceptibility or phenotypic hypersusceptibility that was not predicted by HIV genotyping. 10 In this study, we evaluated genotypic and phenotypic antiretroviral drug resistance in RHSP participants who failed first- or second-line ART regimens.
Materials and Methods
Source of samples used for analysis
Between June 2004 and September 2009, 1925 participants with a CD4 cell count ≤250 cells/mm3 or World Health Organization (WHO) stage IV disease were started on first-line ART. Treatment response was monitored every 6 months with CD4 cell counts and HIV viral load testing. CD4 cell counts were measured by FACSCalibur (Becton Dickenson, NJ) and HIV-1 viral loads were measured using the Roche Amplicor 1.5 Monitor assay (Roche Diagnostics, IN); these assays were performed at the study site in Rakai, Uganda. This laboratory participates in quality assurance programs through the College of American Pathologists (CAP, for CD4 cell counting and HIV viral load testing), the UK National External Quality Assessment Service (NEQAS) (for CD4 cell counting), and the Virology Quality Assurance Program (VQA) of the National Institutes of Health (for HIV viral load testing). We analyzed HIV drug resistance in individuals with virologic failure, defined as an HIV viral load >2000 copies/ml after a minimum of 6 months on first-line ART. Forty-one individuals were selected for analysis who met the following criteria for inclusion in the study: (1) they had stored samples collected prior to initiation of ART (baseline) and at the time of first-line ART failure, and (2) they started a second-line ART regimen (Fig. 1). Eight of these first line failures subsequently failed the second-line ART regimen after at least 6 months of therapy and six had resistance results available for analysis of second-line ART failures (Fig. 1).
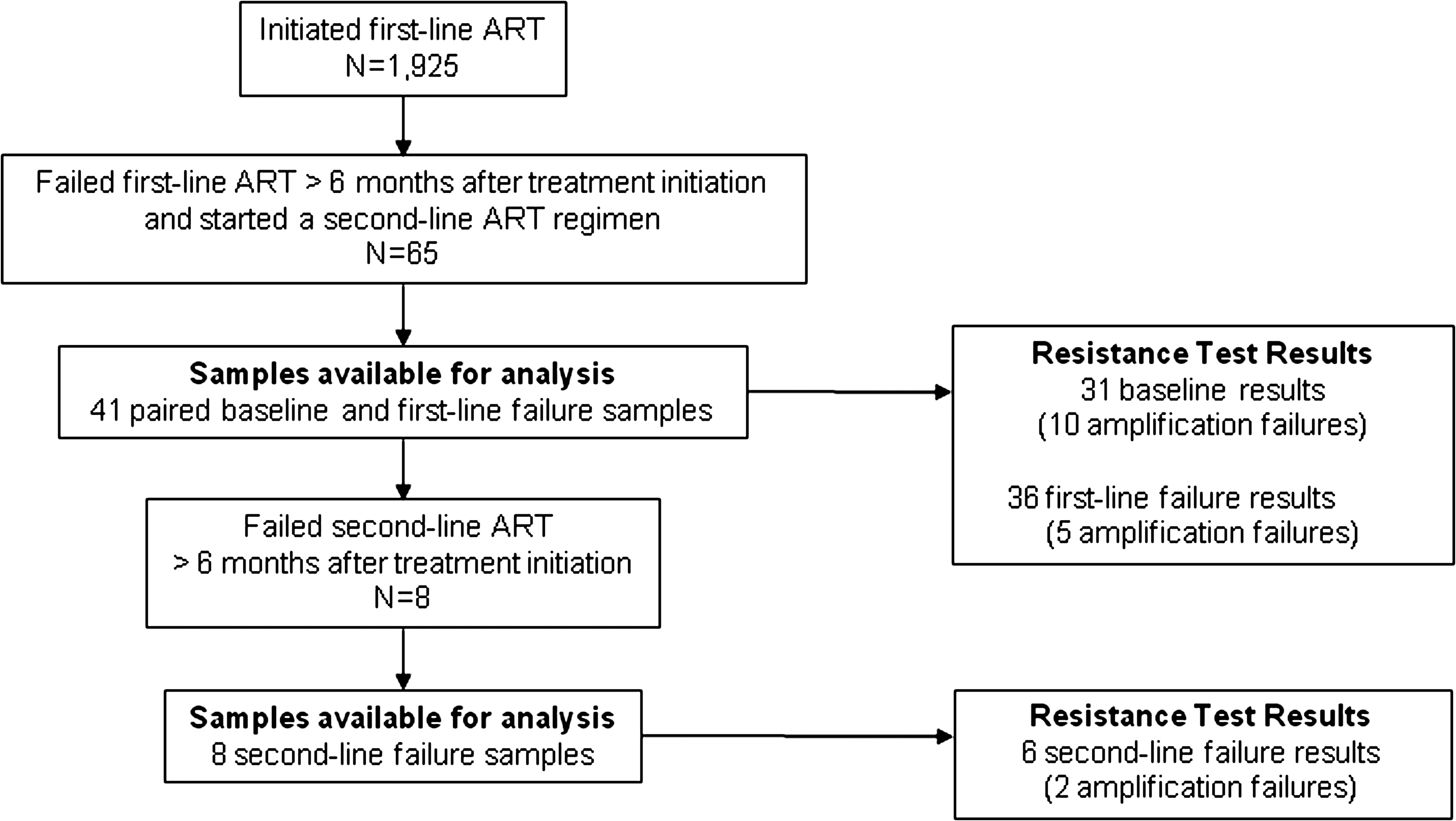
Selection of study participants. The figure shows the process used to select samples for analysis. N, number of individuals; ART, antiretroviral therapy.
HIV resistance testing
The GeneSeq HIV and PhenoSense HIV assays were performed at Monogram Biosciences (South San Francisco, CA; ordered as the PhenoSenseGT assay package). For both assays, the HIV pol region is amplified from a test sample and the amplified DNA is cloned into a test vector. In the GeneSeq HIV assay, vector pools are sequenced to determine the HIV genotype. In this study, genotypic resistance mutations were classified according to the 2010 International AIDS Society listing of major mutations. 11 In the PhenoSense HIV assay, recombinant virus generated from the vector pools is used to infect cells in the presence of varying concentrations of antiretroviral drugs. The amount of drug needed to inhibit viral replication of the test vector by 50% (IC50) is then compared to the IC50 of a reference strain; this ratio (IC50 test vector/IC50 reference) is referred to as the fold change in IC50. The fold change in IC50 is compared to defined clinical cutoff values (either a sole cutoff value, or if available, lower and upper cutoff values) to predict drug susceptibility. The lower clinical cutoff indicates the fold change IC50 that provides the best discrimination of reduced clinical response; the upper clinical cutoff indicates the fold change IC50 above which a clinical response is unlikely. 12 Samples are characterized as susceptible (fold change IC50>0.4 and < lower or sole cutoff value), partial susceptibility (fold change IC50>lower and < upper cutoff value), resistant (fold change IC50>upper cutoff value), or hypersusceptible (fold change IC50<0.4).
Phylogenetic analysis
Pol region HIV subtypes were determined based on phylogenetic analysis of pol sequences (protease and reverse transcriptase). Nucleotide sequences were compared to a set of reference sequences representing HIV-1 group M subtypes and circulating recombinant forms (CRFs), using the BLAST local similarity search algorithm. 13 Each subtype was represented by at least two reference sequences. Pol region sequences were also aligned using MegAlign v5.07 (Clustal W alignment method) and trees were generated to examine the clustering of sequences from the same individual (to rule-out sample mix-ups).
Informed consent
All participants in the RHSP HIV care program provided written informed consent for research-related use of samples and clinical data. The study was approved by the Western Institutional Review Board for Johns Hopkins University (Olympia, WA), the Science and Ethics Committee of the Uganda Virus Research Institute, and the Uganda National Council for Science and Technology.
GenBank accession numbers
GenBank accession numbers are JN652138–JN652210.
Results
Study cohort
By September 2009, 1925 participants in the RHSP had initiated first-line ART and were alive and in care after a minimum of 6 months of treatment. Sixty-five (3.4%) had failed first-line ART and started a second-line regimen. Forty-one of those individuals had paired baseline (pretreatment) and failure samples available for analysis (Fig. 1). Genotypic and phenotypic resistance test results were obtained for 38 (93%) of the 41 participants (31 baseline results, 36 first-line failure results, and six second-line failure results). The median time to failure was 420 days for the first-line regimen (36 participants, IQR 273 to 630 days) and 189 days for the second-line regimen (six participants, IQR 14 to 420 days; two of the participants never achieved virologic suppression, samples from those two individuals were collected 14 days after initiation of second-line ART). Phylogenetic analysis of HIV sequences obtained from HIV genotyping confirmed that sequences from the same individual grouped together (all bootstrap values were >90%), without evidence of sample mix-ups. Baseline characteristics of those 38 individuals are shown in Table 1. The most common first-line regimen was zidovudine (ZDV), lamivudine (3TC), and nevirapine (NVP).
The table shows baseline (pretreatment) characteristics of the 38 participants in the Rakai Health Sciences Program who had resistance test results. IQR, interquartile range; VL, viral load; ZDV, zidovudine; 3TC, lamivudine; d4T, stavudine; NVP, nevirapine; EFV, efavirenz. The recombinant subtypes were A/D (n=2). B/D (n=2), A/E (n=1), and C/D (n=1).
Resistance prior to ART
Four (13%) of 31 participants with HIV genotyping results at baseline had antiretroviral drug resistance mutations to either nucleoside or nonnucleoside reverse transcriptase inhibitors (NRTIs and NNRTIs, respectively, Table 2). One participant had mutations associated with resistance to both NRTIs [3TC, stavudine (d4T), and ZDV] and NNRTIs (dual-class resistance). Three additional participants had mutations associated with NNRTI resistance to NVP or efavirenz (EFV).
The table shows antiretroviral drug resistance mutations detected at baseline (pretreatment) and at the time of treatment failure. Mutations shown in bold text are included in the World Health Organization (WHO) consensus list of drug resistance mutations for epidemiologic surveillance. 19 NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor; TAMs, thymidine analogue mutations.
Resistance at the time of first-line ART failure
Genotypic resistance results were obtained from 36 participants who had evidence of virologic failure on their first-line regimen (HIV viral load >2000 copies/ml). Twenty-nine (81%) of those participants had resistance to 3TC; one of those participants also had 3TC resistance at baseline. Eight (22%) had resistance to either ZDV or d4T; one of those participants also had ZDV/d4T resistance at baseline. No participants were identified with multiple (three or more) thymidine analog mutations (TAMs). However, two (6%) of the participants who were on ZDV-based regimens (one on ZDV/3TC/NVP and one on ZDV/3TC/EFV) developed a K65R mutation that was not detected at baseline. Thirty-one (86%) of the 36 participants had at least one resistance mutation detected that was associated with NVP or EFV resistance; seven of those participants also the mutations detected at baseline. Protease inhibitor (PI) mutations were identified in two (6%) of the 36 participants, both of whom also had the mutations detected at baseline.
Resistance at the time of second-line ART failure
Eight (19.5%) of the 41 participants failed a second-line ART regimen after a minimum of 6 months of treatment and had a second failure sample available for analysis (for two participants, the only sample available for analysis was collected 14 days after initiation of the second-line ART regimen). Resistance test results were obtained for from six of these eight participants, all of whom were switched to a second-line regimen that included a PI and a combination of either tenofovir (TDF) plus emtricitabine (FTC) (n=4) or abacavir (ABC) plus didanosine (ddI) (n=2) (Table 2). Five (83%) of the six participants had genotypic evidence of resistance to 3TC or NNRTIs, and three (50%) had genotypic evidence of resistance to ZDV or d4T; none of the five participants had these mutations detected prior to initiation of first-line ART. None of the six participants had mutations associated with PI resistance and none had the K65R or L74V mutations associated with resistance to TDF, ABC, and other NRTIs.
Genotypic/phenotypic discordance
We compared the results from genotypic and phenotypic resistance assays (Table 3). Six (16%) of the participants (four at baseline and two at first-line ART failure) with results from both assays had discordant results (resistance predicted by either genotypic or phenotypic resistance assays, but not both). In five of the six participants, moderate phenotypic resistance to ddI was detected in the absence of ddI resistance mutations. One participant had a Y181C mutation detected with high-level NVP resistance, but did not have phenotypic resistance to ETR; intermediate-level NVP and ETR resistance has been associated with this mutation. Finally, one participant had phenotypic resistance to ZDV without any ZDV resistance mutations detected.
The table shows the phenotypic drug susceptibility and mutation patterns for samples with discordant phenotypic and genotypic test results (see text). Baseline, prior to antiretroviral therapy; ST, HIV subtype; ID, participant identification number; ABC, abacavir; ddI, didanosine; FTC, emtricitabine; 3TC, lamivudine; d4T, stavudine; TDF, tenofovir; ZDV, zidovudine; DLV, delavirdine; EFV, efavirenz; ETR, etravirine; NVP, nevirapine. Cut-off values are shown in the second row (see Materials and Methods). Bold text indicates reduced phenotypic susceptibility to antiretroviral drugs. Italic text indicates reduced phenotypic drug susceptibility that is not predicted by HIV genotyping.
Discussion
In this study, four (13%) of the 31 participants had evidence of resistance to the standard first-line ART used in Uganda prior to treatment initiation. We do not know whether this reflects infection with a resistant HIV strain (transmitted drug resistance) or acquired drug resistance [e.g., from unreported prior ART use or from prior exposure to drugs used for prevention of mother-to-child HIV transmission (PMTCT)]. Only one of the 31 participants was female, and that participant had no reported prior exposure to antiretroviral drugs for PMTCT.
The frequency of antiretroviral drug resistance prior to ART initiation detected in this study is consistent with recent reports of drug resistance among ART-naive individuals in Kampala, Uganda where a pooled prevalence of 11.6% was observed. 7 Regardless of the etiology, the presence of drug resistance among ART-naive individuals could compromise the success of current ART scale-up programs, particularly in settings where most programs monitor treatment response with only immunologic testing, which has been shown to be relatively insensitive for detecting treatment failure. 4,5
The frequency of resistance observed among 36 adults failing first-line ART is consistent with other reports documenting frequent resistance to NNRTIs and 3TC at treatment failure; this mostly reflects the low genetic barrier to resistance for these drugs. 3,14,15 The relatively low rate of TAMs observed in our study [eight of 36 participants (22%) at first-line treatment failure] is consistent with earlier reports from Uganda that suggest that early detection of virologic failure using viral load monitoring may reduce the risk of NRTI resistance due to the slow rate of accumulation of TAMs. 16,17 This study included genotypic results for only six individuals failing second-line ART. However, it is notable that none of the six individuals developed genotypic or phenotypic resistance to the PI used in the treatment regimen (lopinavir/ritonavir). The relatively short time to failure on these second-line regimens (median 189 days) and the lack of genotypic or phenotypic resistance to PIs suggest that these individuals may have had poor adherence to their second-line treatment regimen.
Six participants had discordant genotypic and phenotypic resistance test results (two with subtype A virus and four with subtype D, Table 3). This is consistent with our previous study of ART-naive adults in the RHSP, which also found discrepant genotypic and phenotypic test results in some individuals. 10 A previous study of subtype A viral clones with NNRTI resistance mutations isolated from Ugandan samples also found unexpected patterns of NNRTI susceptibility. 18 In that study, one clone with no NNRTI mutations had reduced susceptibility to NVP, delavirdine (DLV), and EFV, one clone with K103N had no reduced susceptibility to NNRTIs, and one clone with G190A had extreme hypersusceptibility to DLV. The unusual susceptibility patterns in those clones may have been related to the presence of specific amino acid substitutions in HIV reverse transcriptase (I13T, N136S, N265D). 18 In this study, six (16%) of 38 individuals had reduced phenotypic susceptibility to at least one drug that was not predicted by HIV genotyping (Table 3). In five cases, the fold change IC50 of the test sample was below the upper cutoff for the drug, indicating partial drug susceptibility. One of these five cases also had genotypic resistance (Y181C), but did not have the expected reduced phenotypic susceptibility to ETR. In the sixth case, phenotypic resistance to ZDV was observed in the absence of mutations associated with ZDV resistance. It is important to recognize that the cutoffs used in the PhenoSense assay were derived from ART studies in which most of the participants were likely to have had subtype B HIV infection. It is not known whether different clinical cutoffs for drug susceptibility are needed to predict treatment response in individuals with non-subtype B HIV infection. There are also limited data comparing the natural susceptibility of different HIV subtypes to antiretroviral drugs or the impact of specific resistance mutations on drug resistance in different HIV strains. Four (67%) of the six participants in our study who had discordant phenotypic/genotypic results had subtype D infection. However, this is consistent with the distribution of the subtypes included in this analysis; 63% of the participants analyzed had subtype D HIV infection. 10,18 The findings in this study and our previous reports suggest that HIV genotyping may not provide an accurate picture of antiretroviral drug susceptibility in some patients with non-subtype B HIV infection.
The study has some limitations. Some samples could not be analyzed due to amplification failure, most likely because of the low volume of plasma available for analysis. Although the rates of death and loss to follow-up in the RHSP ART program are relatively low (8.3% and 2.4%, respectively, unpublished data), the participants analyzed in this report may have had higher levels of adherence to their ART regimens than individuals who were lost to follow-up or died. This study included only individuals who began a second-line treatment regimen. This excluded individuals who failed their first-line regimen because of poor adherence. Because poor adherence to treatment regimens is associated with emergence of antiretroviral drug resistance, exclusion of those participants may have led to underestimation of the frequency of resistance in the RHSP population.
As the global community continues to strive toward universal access to HIV care and treatment, ongoing monitoring of the impact of ART programs and optimal monitoring strategies are important. The ideal strategy for identifying individuals failing ART remains a key research question, given the limited resources available for viral load monitoring and resistance testing. The emergence of drug resistance and the potential for transmitted drug resistance could hamper the progress made to date by ART programs. The frequency of antiretroviral drug resistance prior to ART initiation in the rural population described in this report highlights the importance of ongoing surveillance efforts to monitor the frequency and emergence of drug resistance.
Footnotes
Acknowledgments
We would like to acknowledge all the Rakai Health Sciences Program participants and staff for their dedication to research.
Source of funding: (1) The Division of Intramural Research, National Institute of Allergy and Infectious Diseases, (2) R01 Grant R01 HD050180 from the Eunice B. Shriver National Institute of Child Health Development (NICHD), National Institutes of Health (NIMH) and by the Division of Intramural Research, National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), (3) Contract HHSN261200800001E from the National Cancer Institute, NIH, (4) the HIV Prevention Trials Network (U01-AI068613 and UM1-AI068613) sponsored by the National Institute of Allergy and Infectious Diseases (NIAID), the National Institute on Drug Abuse (NIDA), the NIMH, and the Office of AIDS Research, NIH, through the Department of Health and Human Services (DHHS).
The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
Author Disclosure Statement
No competing financial interests exist.