
Abstract
Il28B single nucleotide polymorphisms were found to influence interferon λ expression, resulting in changes in hepatitis C virus (HCV)-RNA serum levels as well as the HIV-RNA set point prior to combined antiretroviral therapy (cART). To date, there is limited information on the influence of this polymorphism on survival in HIV-infected, treatment-naïve, and antiretroviral-treated patients. Longitudinal data from 484 patients diagnosed with HIV infection (including 406 on cART) were analyzed to investigate the association between Il28B rs 1979860 variants and all-cause mortality. Kaplan–Meyer and Cox models were used to calculate the hazard ratio associated with IL28B genotypes predictive of a greater likelihood of survival for patients prior to the introduction of cART and for patients on cART. The IL28B genotype frequencies were 41.7% (n=202) for CC, 46.5% (n=225) for CT, and 11.7% (n=57) for TT patients. The CC variant was associated with higher mortality (46 cases, 22.8%) compared to other genotypes [n=31 (13.8%) and n=7 (12.3%) for CT and TT, respectively, p=0.02]. IL28 genotypes did not influence the survival probability prior to treatment initiation (HR 1.04, 95% CI: 0.84–1.24, p=0.68). In antiretroviral-treated patients, after adjustment for gender, baseline CD4 count, CDC category at HIV diagnosis, and age (multivariate HR 1.75, 95% CI: 1.20–2.30, p=0.047), the CC genotype was associated with a decreased probability of survival when compared to the non-CC genotype (univariate HR 1.8, 95% CI: 1.28–2.34, p=0.029). IL28B rs12979860 genotypes influence mortality risk in HIV-infected, antiretroviral-treated patients. The effect may be related to higher baseline plasma HIV viremia and possibly altered immune reconstitution associated with interferon λ expression.
Introduction
I
Recently, genetic variation of the IL28B, coding for the type III interferon λ, has been found to be of special interest as it was strongly predictive of sustained virological response to peginterferon–ribavirin therapy in patients with chronic hepatitis C. 6,7 Interferon λ was previously shown to induce expression of CC chemokine receptors, namely MIP-1α and MIP-1β, on macrophages and dendritic cells, stimulating intracellular synthesis of type I interferon and expression of virus restriction factors such as APOBEC3G/3F. 8 It was also found to protect mice from HSV-2 infection and reduce viral titer in case of such infection. 9
So far, several single nucleotide polymorphisms of IL28B have been studied in the context of spontaneous clearance of HCV infection and response to hepatitis C virus (HCV) treatment. A strong association was observed between favorable treatment response and higher rates of spontaneous HCV infection clearance and IL28B rs12979860 CC homozygotes. 6,7,10 –12 An association between initial treatment response was also noted in HIV-infected patients coinfected with chronic hepatitis C, and was consistently reported for HCV genotypes 1 and 4. 13 –16 This polymorphism was associated with better response even among prior nonresponders 17 but not with treatment response rates among HIV-positive patients acutely infected with HCV. 18 IL28B rs12979860 remains in linkage disequilibrium with IL28B rs8099917 for which a similar interferon treatment response and spontaneous clearance-modifying effects have been observed. 19 –21
As it was observed that variation in IL28B influences interferon λ expression and is associated with variation in HCV and HIV-RNA set point differences, 18,22 this study aimed to explore the relationship between IL28B polymorphisms and survival in HIV-infected patients on antiretroviral treatment and prior to therapy initiation.
Material and Methods
Patients
The Centre, consisting of the Department of Infectious Diseases and Hepatology, Pomeranian Medical University in Szczecin (in-treated patients) with the Clinic for Acquired Immunodeficiency, Regional Hospital in Szczecin (out-patients) is one of 15 specialist HIV reference centers in Poland. Antiretroviral drugs are dispensed free of charge to all patients qualified for treatment; patients are selected in accordance with national treatment guidelines 23 by an infectious diseases specialist, and remain under follow-up in the Centre. Untreated patients are routinely monitored every 6 months, while treated ones are monitored monthly with laboratory analyses, which typically include CD4 cell count (Becton-Dickinson, Warsaw, Poland) and HIV-RNA viral load (currently Cobas TaqMan HIV-1, Roche, Poland) carried out every 4 months. Additional analyses such as genotypic drug resistance or HLA B*5701 testing are performed as needed. Since 1996, 950 patients have been followed-up in the Centre; of these approximately 450 have been receiving antiretroviral treatment, with 310 patients on stable cART at the moment. Patients followed-up in the Centre are almost exclusively white, and only such individuals were analyzed.
For this study, data and genetic material collected from 507 patients to investigate the association between risk for all-cause mortality and CCR5 Δ32 deletion were used. 24 A range of lymphocyte CD4 metrics (namely baseline, nadir CD4 count, as well as a zenith value––the highest ever recorded number of the CD4 lymphocytes), baseline HIV-RNA serum levels, and clinical data were included in the analyses. HCV-positive status was assigned for individuals positive for anti-HCV antibody and/or with detectable HCV-RNA using commercial assays available in the local hospital laboratory. Ethical approval to perform this study was obtained in 2011 from the local bioethical committee of Pomeranian Medical University (approval number BN-001/34/04).
IL28B genotyping
IL28B (rs12979860) genotyping was carried out by polymerase chain reaction (PCR) using flanking primers (forward: 5′-gCAggCTCAgggTCAATCA; reverse: 5′-CC CC TAACC TCTgCACAgTC) and dual-labeled TaqMan probes (5′ YAK-TggTTCgCgCC + T + TC–Q and 5′ FAM-CTggTTCACgCC + T + TC–Q) with real-time fluorescence acquisition. In brief, human genomic DNA was extracted using commercial kits: the QIAamp DNA Blood Mini Kit (QIAgen, Hilden, Germany) for full blood samples or the Sherlock AX Kit (A&A biotechnology, Gdynia, Poland) for plasma samples. Each 20 μl PCR reaction contained 20 ng of genomic DNA, 900 nM of each primer, 300 nM of the probes, and 10 μl of TaqMan Genotyping Master Mix (Applied Biosystems, Foster City, CA). The amplification conditions on the StepOne instrument (Applied Biosystems, Foster City, CA) consisted of one AmpliTaq Gold activation cycle of 10 min at 95°C and 40 cycles of amplification (denaturation at 95°C for 15 s and annealing/extension at 60°C for 1 min with the signal acquisition step). For allele discrimination TaqMan Genotyper Software (Applied Biosystems, Foster City, CA) was used.
Statistical analyses
Hardy-Weinberg equilibrium for the analyzed genotypes was calculated automatically by StepOne instrument software. The association between nominal variables and IL28B genotypes was assessed using the χ2 test while for continuous variables the Mann–Whitney U test was implemented. For survival analysis the Kaplan-Meyer model with the log-rank test and the Cox proportional hazards regression model to calculate hazard ratio (HR) were used. For all analyses time from a positive HIV confirmation test (time 0) until either death, loss to follow-up, or termination of data collection (end of January 2010) was considered. Separate analyses were carried out for untreated individuals (beginning from the time of HIV diagnosis, with censoring at the time of cART initiation, death, or loss to follow-up) and treated individuals (starting from cART initiation, censored at the termination of data collection, death, or loss to follow-up). A patient was regarded as treated after 1 month of stable antiretroviral treatment. Deaths were coded according to the CDC case definition criteria and International Classification of Diseases, Tenth Revision. Analyses were performed for the entire cohort of HIV-infected patients and separately for HIV/HCV-coinfected and HIV-monoinfected individuals.
Pegylated interferon–ribavirin (PegIFN/RBV)-treated patients were assigned a “lost to follow-up” status in the analyzed dataset at the time of PegIFN/RBV treatment initiation, to remove the possible influence of this treatment on survival. Individuals were followed up for a median of the 15.3 [interquartile range (IQR) 24.3–92.6] months prior to cART initiation and 57.3 (IQR 24.3–92.6) months following therapy initiation.
Results
Genotype and allele frequencies
Genotyping was successful for 484 of the 507 patients (95.5%) of which 254 were HCV/HIV coinfected. All allele and genotype distributions were in accordance with Hardy–Weinberg equilibrium. The IL28B CC genotype was observed at a prevalence of 41.7% (n=202), CT at a prevalence of 46.5% (n=225), and TT at a prevalence of 11.7% (n=57). The overall frequency of the T allele was 35.0%. The genotype and allele distributions did not differ significantly between the subgroups with HIV/HCV coinfection [CC 41.7% (n=106), CT 46.1% (n=117), TT 12.2% (n=31), T allele frequency of 35.2%] and HIV-monoinfected individuals [41.7% (n=96), CT 47.0% (n=108), TT 11.3% (n=26) with a T allele frequency of 34.8%].
Baseline patient characteristics
At baseline, when analyzed for the carriers of the CC genotype versus non-CC and TT genotype versus non-TT (Table 1), genotype frequencies were comparable with respect to gender (the overall cohort was 30.5% female) as well as transmission route (calculated as injection drug use versus sexual transmissions) and HIV clinical infection status at diagnosis (clinically asymptomatic versus symptomatic). It must be noted, however, that the individuals with the TT homozygote were slightly younger at the time of HIV diagnosis and at the time of cART initiation when compared to C allele carriers (p=0.07) with a significantly higher pretreatment HIV plasma viral load (p=0.03) (Fig. 1a). Additionally, in TT homozygous individuals the zenith CD4 count tended to be slightly higher (p=0.09, Fig. 2a) compared to non-TT carriers, despite a slightly lower CD4 count nadir associated with the T allele. No significant differences were observed for baseline HIV plasma viral load and zenith CD4 count when CC genotypes were compared to T allele carriers (Figs. 1b and 2b).


Sample size is 406 patients.
Availible for 277 patients.
Calculated for 406 patients.
Data for individuals homozygous for the major (CC) versus non-CC allele and minor (TT) versus non-TT are shown.
HCV, hepatitis C virus; cART, combined antiretroviral therapy; IQR, interquartile range.
Association of the IL28B genotypes with survival
In the analyzed cohort a total of 84 deaths were recorded in the follow-up period; 46 (22.8%) among individuals with the IL28B CC genotype, 31 (13.8%) among individuals with the IL28B CT genotype, and 7 (12.3%) among TT individuals (p=0.02). Fifty-five deaths were assumed to be AIDS related. The observed distribution of the IL28B genotype in the group with AIDS-related death was as follows: CC 28 (13.9%), CT 21 (9.3%), TT 6 (10.5%), (p=0.33). Of the 484 patients analyzed in this study 406 individuals received antiretroviral treatment for a period of more than 1 month. The remaining patients were either lost to follow-up, died within the first month of treatment, or have never been qualified for the therapy. Kaplan–Meyer (Fig. 3) and univariate Cox analyses were calculated for all three genotypes separately; no association between the IL28B genotype and survival was observed either for the antiretroviral treatment-naive individuals (univariate HR 0.98, 95% CI: 0.84–1.13, p=0.84 for the Cox model and p=0.99 for the log-rank test) or following therapy initiation (univariate HR 1.08, 95% CI: 0.72–1.46, p=0.64 for the Cox model and p=0.11 for the log-rank test). However, carriage of the IL 28B CC genotype was associated with decreased survival on antiretroviral therapy when compared to the non-CC genotype (univariate HR 1.8, 95% CI: 1.28–2.34, p=0.029 for the Cox model and p=0.028 for the log-rank test), despite a similar survival probability prior to treatment initiation (univariate HR 1.04, 95% CI: 0.84–1.24, p=0.68 for the Cox model and p=0.68 for the log-rank test) (Fig. 4). The association between the IL28B CC genotype and decreased survival probability for the antiretroviral-treated individuals remained significant after adjustment for gender, baseline CD4 count, CDC category at HIV diagnosis (asymptomatic vs. symptomatic), and age (multivariate HR 1.75, 95% CI: 1.20–2.30, p=0.047), as presented on Fig. 5.
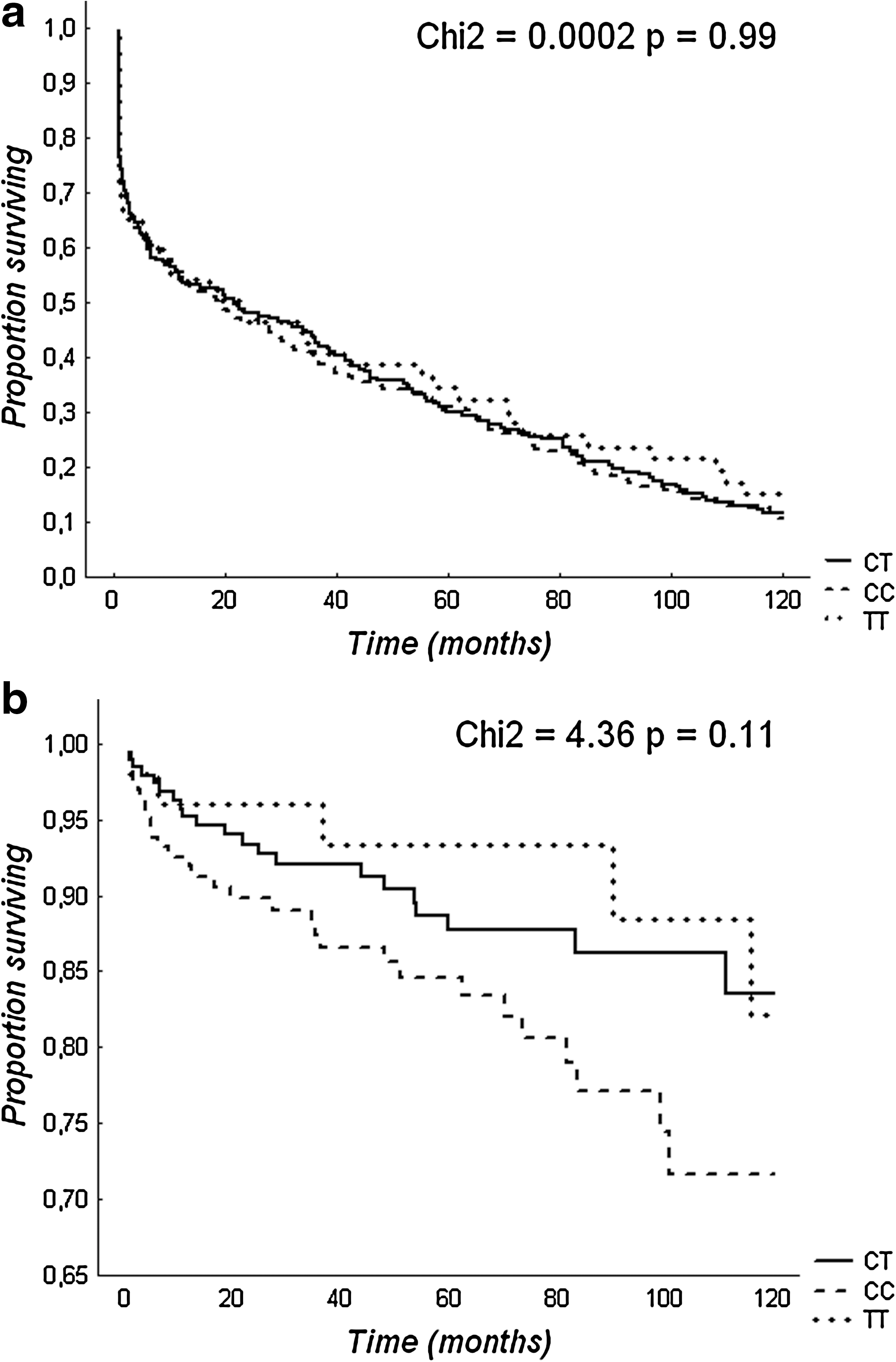
Kaplan–Meier plots comparing the influence of the IL28B genotypes on survival from HIV diagnosis to initiation of antiretroviral therapy

Kaplan–Meier plots comparing the influence of the IL28B genotypes on survival from HIV diagnosis to initiation of antiretroviral therapy

Multivariate Cox hazards for the factors associated with all-cause mortality.
When the cohort was divided into the HCV and non-HCV group we observed a weak association (borderline statistical significance) between the IL28B non-CC genotype and improved survival in univariate analysis for the HCV group (HR: 1.93, 95% CI: 1.20–2.67, p=0.078). No statistically significant associations between survival and CC versus non-CC genotype was found either for antiretroviral treatment-naive patients with or without a history of HCV infection or for non-HCV antiretroviral-treated patients. Finally, when IL28B TT homozygotes versus non-TT genotype carriers (CT + CC) were analyzed no significant associations with survival were observed (data not shown).
Discussion
This study examining the frequencies of IL28B rs12979860 variants in a cohort of HIV-infected white patients including both monoinfected and HCV-coinfected individuals is the first one to describe the influence of this variation on survival in antiretroviral-treated individuals. The novel finding presented in this report is the association with the rs12979860 CC genotype and higher all-cause mortality after introduction of antiretroviral treatment; this association was not observed prior to cART initiation and may be related to an altered immune response. In multivariate analysis, the association proved significant when adjusted for gender, clinical infection status at diagnosis, baseline lymphocyte CD4 count <100 cells/μl, and age.
The observed allele and genotype frequencies are consistent with the previously reported data for IL28B rs12979860 variant distribution available for white populations. 11,25,26 In our study no significant differences in allelic frequency between HIV-monoinfected and HIV/HCV-coinfected groups were observed. The effect of the IL28B genotypes on survival was examined separately prior to the initiation of antiretroviral treatment and while on cART. The IL28B variants did not confer survival advantage prior to treatment initiation; however, an association between increased survival and non-CC genotype was found in antiretroviral-treated individuals.
After dividing the entire analyzed cohort into HIV-monoinfected and HIV/HCV-coinfected patients, the moderate beneficial effect on survival among non-CC was observed but only among the coinfected subjects. The loss of statistical significance in the HIV monoinfected group might be associated with sample size. Of note, TT genotype carriers were slightly younger both at the time of HIV diagnosis and at the time of antiretroviral treatment initiation, which might have had an influence on mortality rate; however, no significant differences in age were observed when survival analysis was performed for the IL28B CC versus non-CC genotype carriers.
To date, only one study investigated the association between likelihood of acquiring HIV infection, HIV-associated disease progression, and IL28B variants in HIV-infected patients. 27 None of the genotypes was found to influence the susceptibility to infection or the outcome of human immunodeficiency infection defined as time to AIDS or death. However, in the cited study, only overall effect on survival was investigated without a separate analysis of untreated and antiretroviral-treated patients in a group of mixed ethnicity (68% of whites). Similar to our study, a significant effect of the IL28B genotypes was seen only in antiretroviral-treated individuals and joint analysis of the treated and untreated subjects might not reveal the influence of this variation. In another study, 28 performed on a much smaller group (29 seronegative individuals at risk for HIV infection and 68 HIV-positive patients), no significant protective role of the IL28B polymorphism on HIV infection and immune deficiency progression was found and it may be hypothesized that IL28B gene variants do not influence the progression of HIV infection, which is in line with our finding of no significant association among untreated subjects.
An additional finding observed in this study is related to the difference in pre-cART HIV viral load between IL28B TT homozygotes and C allele carriers as TT homozygous individuals presented with notably lower pretreatment HIV-RNA levels. This phenomenon is somewhat consistent with an observation by Nettermann et al. who found that mean HCV-RNA serum levels are significantly higher among individuals with chronic HIV/HCV coinfection and non-CC genotype. 18 In our study this association follows the autosomal recessive trait model, similar to the association between HCV-RNA and TT homozygosity found by Labarga et al. 29
Ge et al. hypothesized that genetic variation of the IL28B influences regulation of interferon-stimulated gene expression alerting both the interferon–ribavirin treatment response of HCV and HCV viral load. 10 An association between decreased survival rates in IL28B CC homozygotes and lower pretreatment HIV-RNA levels among the TT genotype observed in our study seems to be in line with this hypothesis and published data describing the lower expression of interferon-stimulated genes (ISGs) among interferon–ribavirin treatment responsive IL28B CC variant carriers. 30 A similar result was presented by Honda et al. for the IL28B rs8099917 variants in the study; they reported that the minor IL28B GT/GG genotype, which remains in linkage disequilibrium with IL28B rs12979860 variants, is associated with higher expression (up-regulation) of interferon-stimulated genes and HCV treatment nonresponse. 22 An association between altered liver ISGs expression and HCV treatment response was also confirmed by Dill et al. 31 Interestingly, in our study the highest recorded lymphocyte CD4 count was slightly higher among IL 28B TT homozygotes compared to CC /CT carriers. This observation might indicate that T allele carriers might have a better ability to control HIV infection and restore immune function and have a positive association with a naturally higher expression of interferon λ levels. It is possible that the variation in interferon λ expression influences HIV replication resulting in higher pretreatment HIV viral loads and better CD4-related immune response in TT homozygotes but lower cART efficacy with a survival disadvantage in IL28B CC carriers.
A limitation of this study is related to the fact that there was no ability to control for antiretroviral treatment adherence, as in the analysis of the longitudinal data no such record was available. The study was performed in a local cohort of white patients; it will be necessary to confirm the effect on larger groups as well as in other ethnicities. To obtain a better statistical association for HIV/HCV-coinfected and HIV-monoinfected groups analyzed separately, larger patient numbers might be required for future studies.
In summary, IL28B rs12979860 variation with an associated modification of the mortality risk in antiretroviral-treated HIV patients is a novel finding and its significance is yet to be determined. Results of this study require further analysis in the context of various therapeutic regimens but may be of particular significance in explaining differences in the antiretroviral treatment response among HIV-infected patients. It may be important from the perspective of long-term, lifelong antiretroviral treatment and may help to identify subjects with potentially worse treatment outcomes requiring closer follow-up and possibly more intensive therapeutic interventions.
To conclude, the effect of interferon λ and IL28B genetic variation influencing its expression in HIV infection is still not elucidated; however, our results indicate that the differences in interferon λ levels might be associated with the response to antiretroviral treatment. It can be hypothesized that interferon λ may be a novel target for the investigation of immune-modulating therapies in HIV patients.
Footnotes
Acknowledgments
The study is supported by the Polish Ministry of Science project IUVENTUS PLUS (project number IP2010 030570). The authors would like to express their gratitude to Mrs. Anna Staniszewska and the stuff of the Clinic for Acquired Immunodeficiency, Regional Hospital, Szczecin, Poland for their help with data collection.
The study was presented (oral presentation) at the 13th European AIDS Conference/EACS, October 12–15, 2011, Belgrade, Serbia under the title “IL28B Gene Polymorphisms and All-Cause Mortality In HIV-Infected Patients.”
Author Disclosure Statement
No competing financial interests exist.