
Abstract
The tuberculin skin test for diagnosing latent tuberculosis (TB) has some limitations for HIV-infected patients, especially in BCG vaccinated countries. The objective of this study was to identify the incidence rate of new TB cases among HIV-infected patients in an intermediate TB-endemic area and to examine its correlation with the ELISPOT assay. We prospectively followed up 124 patients with HIV-1 infection to monitor development of active TB disease after performing an ELISPOT assay (T-SPOT. TB test, Oxford Immunotec, Ltd., Abingdon, UK). A total of 120 patients were followed for a median of 947 days; four patients with active TB at enrollment were excluded. Eleven patients developed active TB during 238 person-years, giving a high incidence rate of 4621/100,000 person-years. Patients with positive ELISPOT responses had a higher TB incidence rate than those with negative ELISPOT responses; however this was not statistically significant [20% (6/30) vs. 6.02% (5/83), p=0.052]. A Cox regression analysis showed that the independent risk factors associated with progression of TB were low CD4+ T cell counts, previous history of TB treatment, and positive ELISPOT results. Advanced HIV-infected patients who showed a positive TB ELISPOT assay had a higher rate of progression to TB in the intermediate TB-endemic area.
Introduction
Even today, tuberculosis (TB) is a serious health problem in developing countries. In Korea, the prevalence of tuberculosis was estimated to be 110 per 100,000 populations at the end of 2008. 1 The recent development of enzyme-linked immunospot assays (ELISPOT, Oxford Immunotec, Abingdon, UK) has made it possible to detect an interferon gamma (IFN-γ) response to TB-specific antigens, early secretory antigen target-6 (ESAT-6) and culture filtrate protein-10 (CFP-10). 2
Some studies have shown the clinical utility of ELISPOT assays among HIV-infected individuals in low income countries, where bacillus Calmette-Guérin (BCG) vaccination is uncommon. 3,4 However, its usefulness has not yet been well studied for HIV-infected patients living in intermediate TB-burden countries, where routine BCG vaccination programs during infancy are installed. Furthermore, longitudinal studies have not been reported on the proportion of TB cases among HIV-infected patients with positive ELISPOT results, or TB cases that developed during follow-up periods. There is yet no consensus about the diagnosis or treatment of latent TB in patient with HIV infection in Korea. The situation is more complicated by the fact that more than 80% of the population is vaccinated with BCG routinely, and consequently, the tuberculin skin test (TST) for the diagnosis of latent TB has limitations. 5
The objective of this study was to evaluate the usefulness of an ELISPOT assay for measuring TB antigen-specific immune responsiveness in patients with HIV infection in an intermediate TB-endemic area. We actively followed up the HIV infected patients and identified the incidence rate of new TB cases, determining whether the patients who responded positively to the ELISPOT assay showed a higher incidence rate of new TB cases than those who responded negatively to the assay.
Materials and Methods
Study design
This is a prospective observational cohort study. This study was approved by the institutional review board of the hospital. Participants provided written informed consent. We enrolled patients receiving HIV/AIDS care at Seoul St. Mary's Hospital, Uijeongbu St. Mary's Hospital, and St. Vincent Hospital from June 2007 to December 2009. We followed up the patients at the outpatient clinic at least once every 3 months, and observed them for the development of active TB disease during the follow-up periods.
Subject selection
Nonpregnant HIV/AIDS adults aged >18 years who were neither currently receiving antituberculosis treatment nor had evidence of active TB were eligible.
At the time of enrollment, the following data were collected from all the patients: history, BCG vaccination scar or documented vaccination history, demographic characteristics, physical examination, chest x-ray, baseline laboratory testing that included CD4+ T cell count and HIV viral load, and ELISPOT assay. At baseline, we excluded active TB cases by performing initial evaluations including clinical symptom assessments, physical examinations, and chest radiography. We followed up the patients at the outpatient clinic, and if the patients had at least one of the following symptoms or signs—cough, sputum, weight loss, night sweating, fever, and/or any suspicious finding on clinical examination, we performed a chest x-ray and/or other imaging studies, sputum study including acid-fast bacillus smear and culture, polymerase chain reaction (PCR) for Mycobacterium tuberculosis, or biopsy depending on the doctor's opinion. According to the results, we divided the subjects into patients with active TB (TB progressor) and those without TB (TB nonprogressor). The study investigators who had no knowledge of the results of the ELISPOT assay classified all the cases independently on the basis of clinical, radiologic, histopathological, and microbiological infection. 6,7
Definition
Fibrotic TB sequelae were defined as a nodular or streaky density in the upper lobes of the lung or calcification with negative mycobacterial culture of the sputum and no sign of infection. Latent TB was defined as evidence of old TB sequelae on chest radiography or the presence of a history of prior TB. Diagnosis of active TB was based on current recommendations. 6 Confirmed TB was defined as positive culture results or PCR results and probable TB as (1) histological finding of biopsy such as caseaous granuloma or radiologic finding compatible with TB and (2) successful response to anti-TB medication.
ELISPOT assay
The ELISPOT assays for IFN-γ were performed following the manufacturer's instructions. 8 –11 Briefly, peripheral blood mononuclear cells (PBMCs) were immediately separated from fresh samples (8 ml) of peripheral venous blood. Viable PBMCs at a concentration of 2.5×105 were added to 96-well membrane-bottomed plates precoated with anti-IFN-γ antibodies. Four wells were used for each patient: a positive control well to which phytohemagglutinin (PHA) was added, a negative control well that contained medium, and two wells that contained ESAT-6 or CFP-10 peptide pools. Cells were cultured for 18 h, and spots were counted with an automated microscope (ELiSpot 04 HR; Autoimmune Diagnostika GmbH, Strassberg, Germany). The criteria for positive, negative, and indeterminate outcomes were applied as recommended by the manufacturer.
Statistical analysis
We compared baseline demographics, previous TB history, and laboratory results among TB progressors and TB nonprogressors. The χ2 test or Fisher's exact test was used for categorical variables and Student's t test or the Mann–Whitney U test for continuous variables. Excluding indeterminate ELISPOT result, ELISPOT assay results according to progression of TB were analyzed by Fisher's exact test. Associations between the factors including the ELISPOT result and the progression of TB were examined using Cox regression models, and odds ratios (OR) and 95% confidence intervals (CIs) were calculated. The number of IFN-γ producing cells to antigens of M. tuberculosis was compared in patients with TB progressors and TB nonprogressors using the Mann–Whitney U test. Statistical analysis was performed using SPSS 13.0 (SPSS Inc, Chicago, IL). and a p value <0.05 was considered statistically significant.
Results
Of the 124 HIV-infected patients who were recruited in the study, four with coprevalent active pulmonary TB at enrollment were excluded (Fig. 1). The median age was 39 years (range, 20–80 years) and 93.3% were male. The median follow-up time was 947 days (range, 135–1318 days) and the median CD4+ T cell count was 306 cells/μl (range, 3–1681 cells/μl). One hundred and three patients (85.8%) had received BCG vaccination, and 10 (8.3%) had a history of completed treatment for TB. The median time since completion of TB treatment was 13 years (range, 3–50 years) (data not shown).
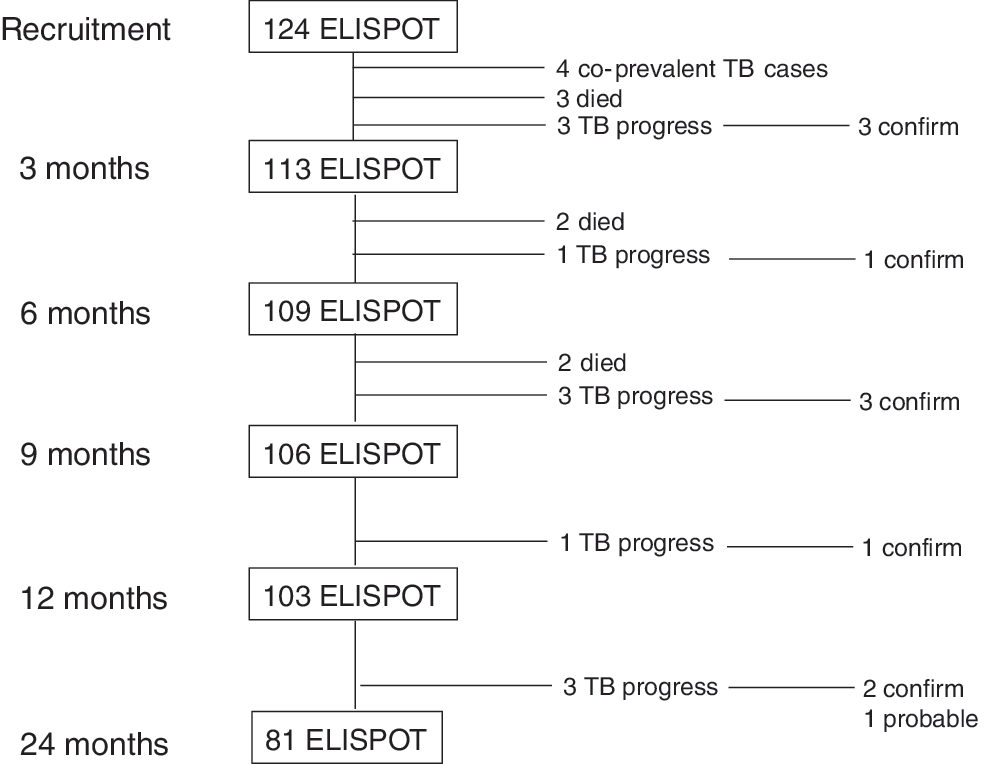
Study profile and timing of presentation for tuberculosis.
Eleven patients were diagnosed as having active TB during the follow-up: seven pulmonary TB, two TB cervical lymphadenopathy, and two disseminated TB. Ten patients were diagnosed as having confirmed TB (nine culture and one pathology PCR), and one as probable TB. The timing of diagnosis of TB after enrollment is shown in Fig. 1. Seven patients (63.6%) were receiving highly active antiretroviral therapy at the time of TB diagnosis. Of the eight patients who died during the follow-up, one died of pulmonary TB combined with Pneumocystis jirovecii pneumonia. The patient had been treated for pulmonary TB 15 years ago, and had a positive ELISPOT result at enrollment. She progressed to TB after 212 days.
Table 1 shows the comparison of the demographic characteristics between the patients who progressed to TB (TB progressors) and those who did not (nonprogressors). The median CD4+ T cell count was lower in the TB progressor group than in the TB nonprogressor group. (161 vs. 323, p=0.01). Patients in the TB progressor group had more previous TB treatment history and old fibrotic TB sequelae on chest radiography (27.3% vs. 6.4%, p=0.01; 45.5% vs. 19.3%, p=0.04, respectively). The two groups did not significantly differ according to age, sex, BCG vaccination status, viral load, and HAART status at enrollment.
Demographic Characteristics of HIV-Infected Patients with and without Progressive Tuberculosis
BCG scar or documented vaccination history.
TB, tuberculosis; BCG, bacillus Calmette-Guérin; HAART, highly active antiretroviral treatment.
The ELISPOT assay results in each groups are shown in Table 2; 30 (25%) had positive results, 83 (69.2%) negative results, and 7 (5.8%) indeterminate results on the basis of the manufacturer's criteria. The HIV patients who had positive ELISPOT assay results at recruitment had a higher rate of TB progression during the follow-up period than those who had negative results [20% (6/30) vs. 6% (5/83), p=0.052]; however, this was not statistically significant.
ELISPOT Assay Results According to Progression of Tuberculosis
Figure 2 shows the comparison between the IFN-γ ELISPOT response to antigens of M. tuberculosis of TB progressors and that of non-TB progressors; the TB progressor group had significantly higher spot-forming cells responding to both ESAT-6 (median, 17 vs. 2, p=0.009) and CFP-10 antigen (median, 8 vs. 2, p=0.03).

ELISPOT response to antigens of M. Tuberculosis.
Table 3 shows the comparison between the individuals, among those with developing TB, with ELISPOT-positive results (n=6) and those with negative results (n=5). The median CD4+ T cell count in the individuals with positive ELISPOT results was higher than in the individuals with negative results (median, 181.5 vs. 94).
Comparison Between the Individuals, Among Those with Developing Tuberculosis, with ELISPOT Positive Results and Those with Negative Results
BCG scar or documented vaccination history.
The Cox regression analysis indicated that the independent risk factors associated with progression to TB were low CD4+ T cell count (OR=18.99, 95% CI, 3.39–106.14; p=0.001), previous history of TB treatment (OR=5.88, 95% CI, 1.39–24.79; p=0.016), and positive ELISPOT results (OR=5.541, 95% CI, 1.46–20.98; p=0.01) (Table 4). After excluding three TB developing cases within the first 3 months, only low CD4+ T cell count (OR=21.73, 95% CI, 2.55–202.4; p=0.005) was found to be a significant risk factor for the progression of TB (Table 4).
Cox Regression Analysis of Risk Factors for Progression of Tuberculosis
Subjects with indeterminate ELISPOT results were excluded from statistical analysis.
Method 1: Cox regression analysis including all TB developing cases.
Method 2: Cox regression analysis after excluding three TB developing cases within the first 3 months.
Discussion
We actively followed up the HIV-infected patients for active TB disease after ELISPOT assay and found that the patients who had lower CD4+ T cell counts, a history of TB treatment, or positive ELISPOT assay results showed a higher TB developing rate.
In developing countries, TB still remains the most common cause of death among HIV-infected patients. 12 Across Asia and the Pacific, 40–70% of patients with HIV/AIDS have TB, and TB is associated with at least 40% of deaths. 12 In Korea, the World Health Organization (WHO) estimated 8 per 100,000 population died of TB among HIV-negative people. 1 It was estimated in 2009 that approximately 9,500 people living in Korea had HIV/AIDS. However, it is not known how many HIV-infected individuals died of TB. 1 Targeted testing and treatment of latent TB in high-risk populations are recommended to decrease the incidence of TB or TB-related mortality as well as protection of transmission. 13 –15 The Centers for Disease Control and Prevention also recommended the benefit of preventive therapy for HIV-infected persons with latent TB. 16 However, in Korea, there is no standard policy as yet on the treatment or the diagnosis of latent TB in HIV-infected patients, because the high resistance rate to isoniazid of approximately 10%, drug interaction or toxicity, and low sensitivity of TST have led us to avoid preventive TB treatment, especially in HIV-infected patients. 17,18
TST based on purified protein derivative has been the most important tool for the detection of latent TB for decades. However, in Korea, where more than 80% of the people are routinely vaccinated for BCG at infancy, TST is unreliable, often providing either false-positive results due to vaccination against BCG or infection with nontuberculous mycobacteria or false-negative results (especially in immune-compromised patients such as those with advanced HIV infection). 5,19 –22 Recently, M. tuberculosis-specific T cell IFN-γ release has been used to support the diagnosis of latent or active TB in HIV-infected patients. 3,23 –25 Our longitudinal analysis of IFN-γ release assay for TB in a BCG vaccination area revealed that 11 HIV-infected patients developed active TB during 238 person-years, giving a high incidence rate of 4,621/100,000 person-years. Twenty percent of the HIV-infected patients with positive ELISPOT response developed active TB during the follow-up period, whereas only 6.02% of those with negative response developed TB.
Although this is not significantly different in our study, these findings suggest HIV-infected patients with positive ELISPOT result may receive preventive therapy for TB, at least in the setting of an intermediate endemic area. However, the sensitivity of ELISPOT was very low with only 54.5% (6/11) of detected patients developing TB. Thus, further long-term studies including large populations are needed.
Our results also show that a low CD4+ T cell count is associated with development of active TB, because the impairment of cell-mediated immunity in advanced HIV patients increases the risk of TB activation as shown in previous reports. 26,27 In our study, people who developed active TB disease with a negative ELISPOT result showed lower CD4+ T cell count than those with a positive result, and this finding could explain why five (6%) people with a negative ELISPOT result developed TB. As in a study by Karam et al., the IFN-γ release assay can be impaired in severely immunosuppressed individuals; however, current data do not clearly confirm the impact of immunosuppression on IFN-γ release assay. 28 –30
In addition, analysis that excludes the three patients with TB developed within the first 3 months showed the low CD4+ T cell count was found to be the only significant risk factor for the progression of TB. This result may support the finding that earlier initiation of antiretroviral therapy in HIV-infected patients can reduce the burden of TB.
Our study has the following limitations. First, we did not perform TST. The comparison between ELISPOT and TST would be helpful in understanding the agreement between the two tests and whether TST is really affected by BCG vaccination status. Second, our sample size is small, and extending the sample size to include a large population is necessary in reaching definitive conclusions. However, this study is a significant contribution to the existing literature in that it demonstrates the importance of preventive TB treatment based on ELISPOT assay for HIV-infected patients living in intermediate TB-endemic areas where BCG vaccination is commonly administered. Third, the time of completion of TB treatment varied in our study, and according to one study, patients with a recent episode of TB showed a greater risk of being infected with TB. 31 In targeted screening for preventive TB treatment, patients with a previous history of TB treatment would normally be excluded. However, in Korea with an intermediate burden of TB, TB reactivation frequently occurs, and our study analyzed various factors for the development of TB. Fourth, the three patients who developed TB within 3 months in our study might have belonged to coprevalent window cases. However, we attempted to exclude the patients with active TB cases during the recruiting period by carrying out initial evaluations including physical examinations and chest radiography.
In conclusion, for HIV-infected patients with positive ELISPOT assay results, especially those who have a low CD4+ T cell count, the risk of developing active TB is higher than in those with negative results. Therefore we may need to consider administering preventive TB treatment on the basis of the ELISPOT results, especially among advanced HIV-infected patients in countries with an intermediate TB burden. This study may support the strategy for the diagnosis or treatment of latent TB in HIV-infected patients, at least in intermediate TB-endemic areas such as Korea.
Footnotes
Acknowledgments
Y.J. Kim, S.I. Kim, Y.R. Kim, and S.H. Wie extracted data from patient care records, Y.J. Park conducted an ELISPOT assay, and Y.J. Kim, S.I. Kim, and M.W. Kang conceived and designed the study, performed the data analysis, and wrote the article.
This research was supported by a chronic infectious disease cohort grant (4800-4859-304) from the Korea Centers for Disease Control and Prevention.
This study was approved by the institutional review boards of this hospital (KCMC06OT097).
Author Disclosure Statement
No competing financial interests exist.