
Abstract
The age of 50 has been considered as a cut-off to discriminate older subjects within HIV-infected people according to the Centers for Disease Control and Prevention (CDC). However, the International AIDS Society (IAS) mentions 60 years of age and the Department of Health and Human Services (DHHS) makes no consideration. We aimed to establish an age cut-off that could differentiate response to highly active antiretroviral therapy (HAART) and, therefore, help to define advanced age in HIV-infected patients. CoRIS is an open, prospective, multicenter cohort of HIV adults naive to HAART at entry (January 2004 to October 2009). Survival, immunological response (IR) (CD4 increase of more than 100 cell/ml), and virological response (VR) (HIV RNA less than 50 copies/ml) were compared among 5-year age intervals at start of HAART using Cox proportional hazards models, stratified by hospital and adjusted for potential confounders. Among 5514 patients, 2726 began HAART. During follow-up, 2164 (79.4%) patients experienced an IR, 1686 (61.8%) a VR, and 54 (1.9%) died. Compared with patients aged <25 years at start of HAART, those aged 50–54, 55–59, 60–64, 65–59, and 70 or older were 32% (aHR: 0.68, 95% CI: 0.52–0.87), 29% (aHR: 0.71, 95% CI: 0.53–0.96), 34% (aHR: 0.66, 95% CI: 0.46–0.95), 39% (aHR: 0.61, 95% CI: 0.37–1.00), and 43% (aHR: 0.57, 95% CI: 0.31–1.04) less likely to experience an IR. The VR was similar across all age groups. Finally, patients aged 50–59 showed a 3-fold increase (aHR: 3.58; 95% CI: 1.07–11.99) in their risk of death compared to those aged <30 years. In HIV infection, patients aged ≥50 years have a poorer immunological response to HAART and a poorer survival. This age could be used to define medically advanced age in HIV-infected people.
Introduction
Aging is a physiological fact that affects all living things. This process is accelerated in HIV-infected patients 1 –3 and, although highly active antiretroviral therapy (HAART) has slowed this process, it is uncertain as to whether this can be fully restored.
Even though most epidemiological studies in the general population do not consider patients ≥50 years as “elderly,” in the case of HIV infection the Centers for Disease Control and Prevention (CDC) has done so arguing that they are a special population. 4 Based on this arbitrary age cut-off it is generally accepted that HIV-infected patients who start HAART after this age will have a poorer immunological response 5 –15 and a better virological response. 5,8,9,15 –19 compared with younger patients. Other studies have found mixed results.
The increasing awareness of the potential implications for health outcomes of the aging process of HIV-infected subjects has also led to the inclusion of age as a key variable for deciding when to initiate HAART in different guidelines. However, there is no consensus on what is the best age cut-off. The European AIDS Clinical Society (EACS) recommended it in patients >50 years, 20 the Spanish GESIDA in those >55 years, 21 and the International AIDS Society (IAS) in >60 years. 22 More recently the Department of Health and Human Services (DHHS) recommend it in patients >50 years. 23
The clinical relevance of this problem encouraged us to carry out the present study in a large prospective, hospital-based multicenter cohort of HAART-naive HIV subjects in Spain from 2004 to 2009. Our aim was to study the impact of the age at HAART initiation as a predictor of the immunological response and virological response as well as survival.
Materials and Methods
CoRIS is an open, prospective, multicenter cohort of HIV-positive subjects, over 13 years of age, who initiated care for the first time at the recruiting centers after January 1, 2004 and were naive for antiretrovirals at entry. CoRIS is linked to a BioBank. 24 Approval has been obtained from all Hospitals Ethics Committees and all patients have signed an informed consent. 25
CoRIS is a joint activity of the Research Network of Excellence (AIDS research network, RIS) that incorporates basic scientists, immunologists, virologists, clinicians, epidemiologists, and statisticians. A total of 27 hospitals from 13 of the 17 Autonomous Regions of the country participate in CoRIS. Cohort members are followed according to each hospital clinical routine, usually every 3–6 months. Internal quality controls are performed twice annually and 10% of data are externally audited every year.
Antiretroviral-naive patients starting HAART from January 1, 2004 to October 31, 2009 (administrative censoring date) were considered for inclusion. We excluded patients who did not have at least one CD4 cell count and viral load measurements in the 6 months prior to HAART initiation and at least two CD4 cell count and viral load measurements following the start of HAART.
Immunological response was defined as an increase of at least 100 cells/ml in CD4 cell count from pre-HAART levels confirmed in two consecutive measurements. Virological response was defined as two consecutive viral loads <50 copies/ml. 14 The clinical endpoint considered was death from any cause.
Statistical analyses
For each individual, follow-up began on the date of starting HAART and ended on the date of last recorded CD4 cell count or viral load measurement for time to immunological and virological response analyses, respectively, or the date of last contact for time to death analyses.
Age at HAART was initially divided into the following age intervals: <25, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, and 70 years or older. However, 10-year age groups were considered for time to death analyses due to the small number of deaths.
The impact of age on the time to immunological response, virological response, and death from any cause was assessed using Cox proportional hazard models. All models were stratified by hospital, and adjusted for sex, transmission category, educational level, country of origin, pre-HAART CD4 cell count and viral load, pre-HAART AIDS diagnosis, year of HAART initiation, and hepatitis C virus (HCV).
All analyses were performed using Stata 11.
Results
Among 5514 patients included in CoRIS, 3523 (64%) started HAART between January 1, 2004 and October 31, 2009. Of those, 282 (8%) had no viral load and CD4 cell count in the 6 months prior to start of HAART and 515 (15%) did not have a minimum of two measurements of viral load and CD4 cell count following HAART initiation. The sociodemographic and clinical characteristics of 2726 patients included are shown in Table 1.
Sociodemographic and Clinical Characteristics of 2726 Patients Included
IQR, interquartile range; IDU, injecting drug user; MSM, men who have sex men; VL, viral load.
During the follow-up, 2164 (79.4%) patients experienced an immunological response. The chance of experiencing an immunological response decreased as age increased (Fig. 1a). Compared with patients aged less than 25 years at start of HAART, those aged 50–54, 55–59, 60–64, 65–59, and 70 or older were 32% (aHR: 0.68, 95% CI: 0.52–0.87), 29% (aHR: 0.71, 95% CI: 0.53–0.96), 34% (aHR: 0.66, 95% CI: 0.46–0.95), 39% (aHR: 0.61, 95% CI: 0.37–1.00), and 43% (aHR: 0.57, 95% CI: 0.31–1.04) less likely to experience an immunological response. The chance of experiencing an immunological response was also associated with having acquired HIV infection through homosexual/bisexual intercourse, higher educational level, European origin, lower pre-HAART CD4 cell counts, higher pre-HAART viral load, AIDS diagnosis at start of HAART, later years of starting HAART, and no HCV coinfection (data not shown).
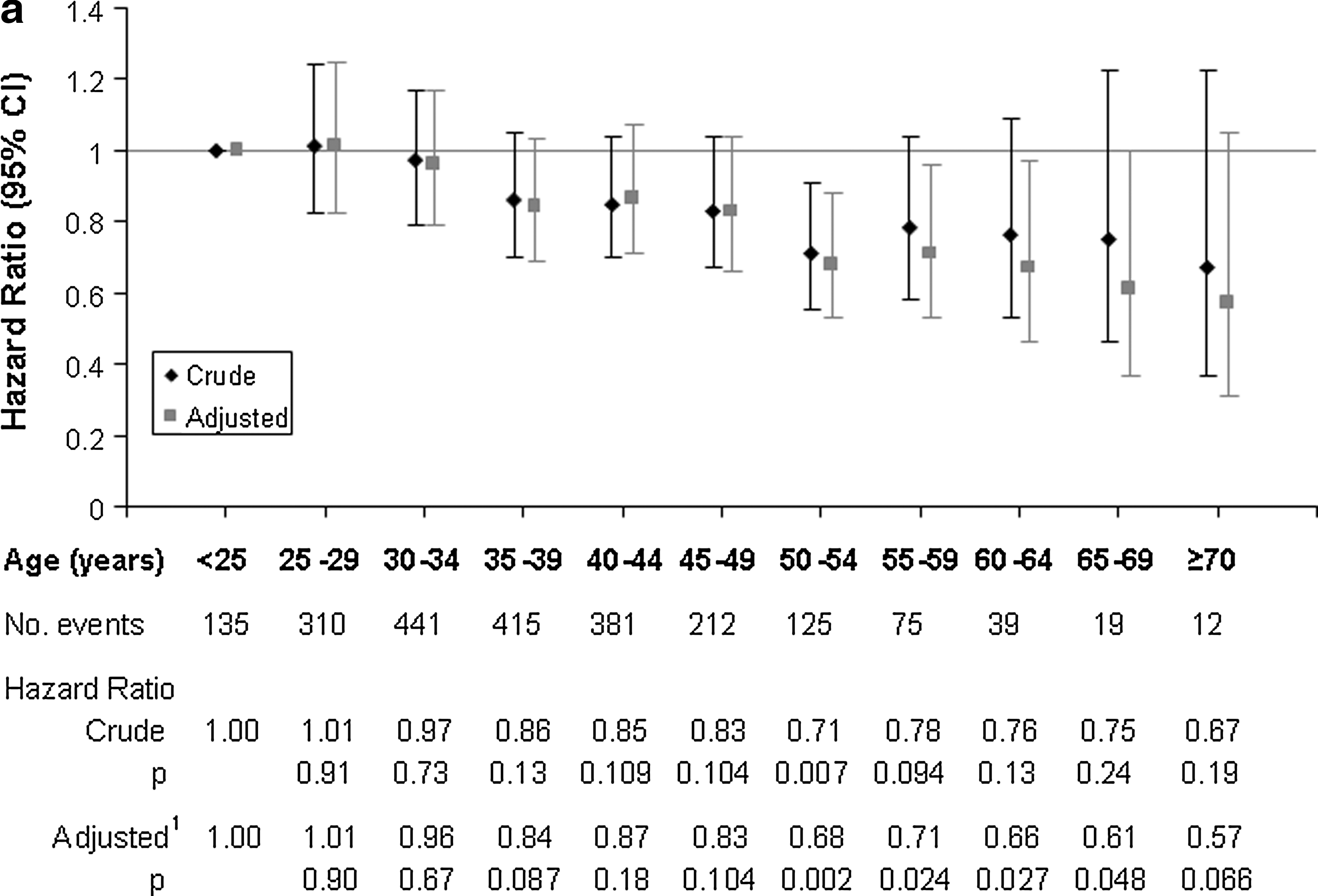
Crude and adjusted hazard ratios of the impact of age on time to
There were significant differences in the median pre-HAART CD4 cell count according to age at start of HAART (p<0.001), with the highest CD4 cell count in patients aged less than 25 years and declining thereafter. In all age groups, the median CD4 cell count increased rapidly in the first 6 months after HAART initiation to follow a more gradual increase thereafter (Fig. 2).
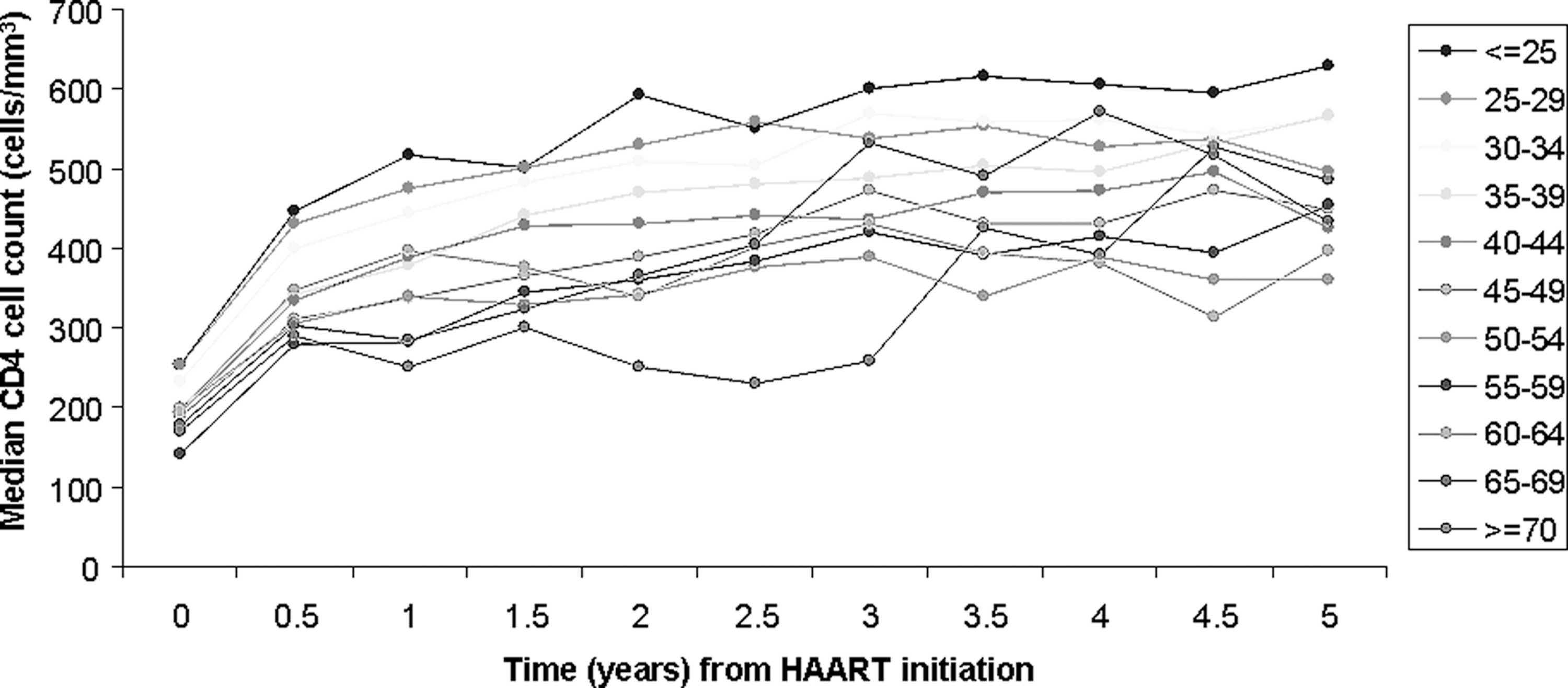
Median CD4 cell count over time according to age group.
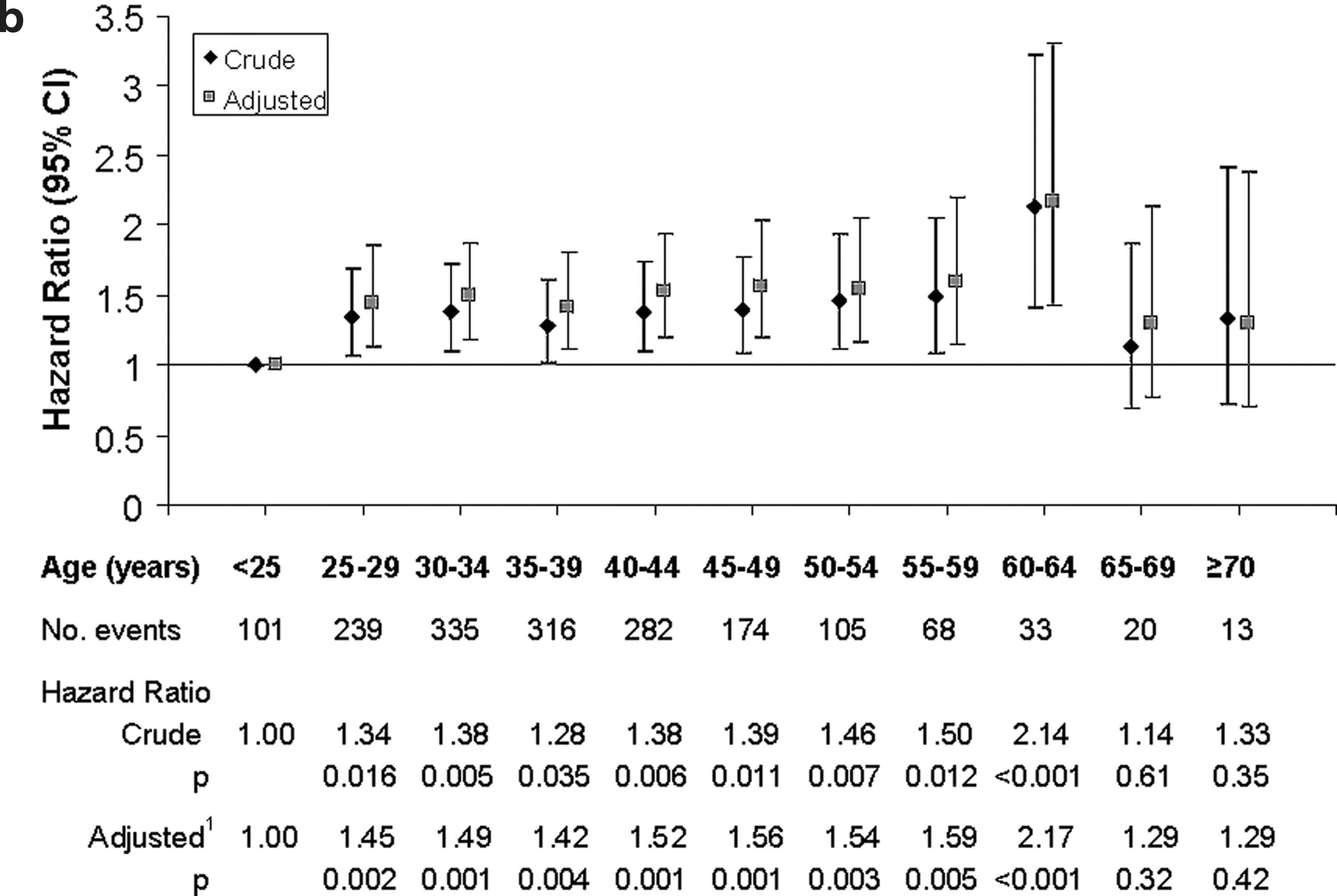
During the follow-up, 1686 (61.8%) patients experienced a virological response, with those aged less than 25 years at HAART initiation showing the greatest chance of response. Among patients aged 25 years or older, the chance of experiencing a virological response was similar across age groups (Fig. 1b).
Other predictors of achieving a virological response were European origin, lower pre-HAART CD4 cell counts, higher pre-HAART viral load, earlier years of starting HAART, and no coinfection with HCV (data not shown).
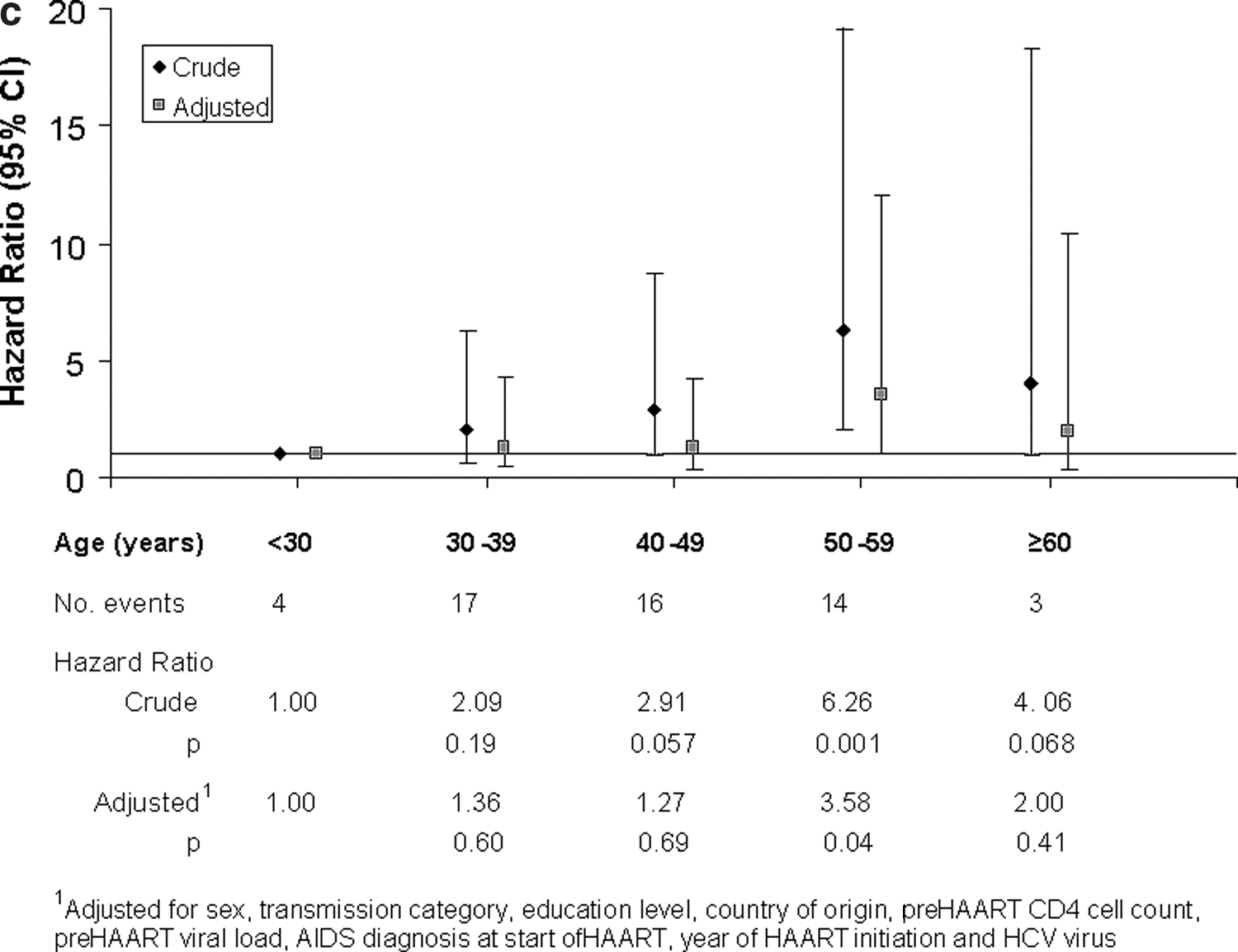
A total of 54 (1.9%) patients died. Of all patients for whom information on the cause of death was available, 75% died of non-AIDS-related causes. No significant differences in the risk of death were found between patients aged 30–39 (aHR: 1.36; 95% CI: 0.43–4.34) or 40–49 (aHR: 1.27; 95% CI: 0.38–4.21) and those aged less than 30 years. However, patients aged 50–59 showed a 3-fold increase (aHR: 3.58; 95% CI: 1.07–11.99) in their risk of death compared to those aged less than 30 years (Fig. 1c). Other predictors of mortality were male sex, lower educational level, AIDS diagnosis at start of HAART, and HCV coinfection.
Discussion
In this large cohort of HIV-infected patients with recent initiation of antiretroviral treatment, we have found that an age of 50 years or more clearly impacts the immunological response and the survival of HIV-infected patients after starting HAART with no effect on the virological response. Our results may have clinical importance. It gives support to current recommendations of initiating antiretroviral therapy after a given age irrespective of other criteria, and establishes the cut-off at which this recommendation should be considered.
As far as immune status is concerned, the determinants of recovery are not entirely clear and seem to depend on both host and virus (HIV). 26 In relation to the host most studies suggest that the immune response to HAART decreases with age. 5 –15 These results are also observed in our study showing a worse immunological recovery in patients aged 50 years or over. However, this has not been observed by other authors. 16,18,19,27 –33 Perhaps the higher prevalence of delayed HIV described in older patients may contribute to their poorer immune response. 30,32,34 –38 In this sense, we found a late diagnosis of HIV infection in 53.3% of the patients >50 years vs. 21.5% in those <30 years (p<0.001). 39 Similar findings were reported by Smith et al., with almost half of patients ≥50 years being late presenters compared to 33% of younger adults (p<0.001). 38 We have shown that the immunological response is lower in patients ≥50 years and is not modified by other variables.
In our study, 61.8% of patients experienced a virological response during the follow-up. Many authors have found no differences in virological control according to age, 7,10,12,27 –32,40 and, moreover, some have found a better virological response in older patients. 5,8,9,15 –19 In our case the virological response was similar across all age groups but improved significantly in patients over 60 years. The best virological control in elderly patients has been associated with better adherence to antiretroviral therapy (ART), 18,28,41 –43 despite the fact that many of them take other treatments (e.g., antihypertensives, antidiabetics). For some authors the best virologic control during the first year of ART in patients ≥50 years was entirely explained by better adherence, 18 while others have observed that this better virological control persists regardless of the degree of adherence, the treatment regimen, and the stage of the CDC. 9 In our study the impact of age on virological response is similar in all the groups and is not modified by other variables, as shown in our analysis.
Overall mortality of patients with HIV infection has decreased significantly in the era of HAART. 44,45 This has been due in particular to the decrease in deaths related to AIDS events while the proportion of deaths related to non-AIDS events (cardiovascular, liver, and tumors) has increased. 44,46,47 In our series 2% of the patients died. Among patients in whom a cause of death was identified (85%), 24% died of an AIDS event (63.6% noninfectious) and 76% of an event not related to AIDS (76.4% of noninfectious cause). These results differ from those found by other authors who noted that the main causes of death in the period from 1996 to 2004 were AIDS events (49.6%), and within them those related to infectious processes (46.2%). 47 The difference may be explained by the more recent initiation of our cohort, which included patients who started therapy after 2004.
Mortality is higher among older patients, 16,18,19,30,46,48,49 which has also been observed in patients between 50 and 59 years in our study. This association is not seen in those aged more than 60 years probably due to the small sample size of this group. Gutiérrez et al. 50 observed that the greater progression to AIDS events or death among older people persists after adjusting for CD4 lymphocyte count in patients on HAART and a sustained virological response. The increased mortality in older patients may be related to age as a predictor of disease progression, diagnostic delay, 30,32,34 –38 the presence of comorbidities, 17,18,29,30,51 or the presence of AIDS or not AIDS, 17,52,53 among others. Other authors have not found an association between mortality and age. 19,44,54
We must recognize some limitations in our study. One of the limitations common to all cohort studies is that they may not be representative of all HIV-infected patients. However, this cohort includes patients from all over Spain with a broad spectrum of patient characteristics and antiretroviral regimens. Also their number is high, limiting the bias of other studies with a smaller sample size. Similarly our cohort is subjected to quality controls limiting errors related to the collection of information. The results should therefore be applicable to many individuals with HIV-1 infection beginning HAART in Spain and elsewhere. In summary, our result indicates that being 50 years of age or older is one of the variables that determines the immunological response and survival of patients with HIV infection. Further studies addressing the when to start question for different age cut-offs using causal methods are warranted.
Footnotes
Acknowledgments
This study would not have been possible without the collaboration of all the patients, medical and nursery staff, and data managers who have taken part in the project. The RIS Cohort (CoRIS) is funded by the Instituto de Salud Carlos III through the Red Temática de Investigación Cooperativa en Sida (RIS RD06/006). Dr. José R. Blanco is a recipient of an INT 11/68 Intensification Research Grant (13SNS) from the Instituto de Salud Carlos III, Madrid, Spain. Members of the CoRIS Group are: Berenguer J, del Amo J, García F, Gutiérrez F, Labargo P, Moreno S, Muñoz MA, Caro-Murillo AM, Vegas PS, Pérez-Cachafiero S, Sebastián VH, Ferreras BA, Alvarez D, Monge S, Jarrin I, Trastoy M, Muñoz-Fernández MA, García-Merino I, Rico CG, de la Fuente JG, Almudena GT, Sogorb JP, de Lucas EM, Bañuls SR, Martínez VB, Oncina LG, Pastor CG, Tamarit IP, Toledo PA, Sirvent JL, Fortúnez PR, Valls MR, Socas Mdel M, Lirola AM, Hernández MI, Díaz-Flores F, Soriano V, Labarga P, Barreiro P, Castañares C, Rivas P, Ruiz A, Blanco F, García P, de Diego M, Asensi V, Valle E, Cartón JA, Miró JM, López-Dieguez M, Manzardo C, Zamora L, Pérez I, García MT, Ligero C, Blanco JL, García-Alcaide F, Martinez E, Mallolas J, Gatell JM, Rubio R, Pulido F, Fiorante S, Llenas J, Rodríguez V, Matarranz M, Iribarren JA, Arrizabalaga J, Aramburu MJ, Camino X, Rodríguez-Arrondo F, von Wichmann MA, Tomé LP, Goenaga MA, Bustinduy MJ, Galparsoro HA, Gutiérrez F, Masiá M, Ramos JM, Padilla S, Navarro A, Montolio F, Peral Y, García CR, Clotet B, Tural C, Ruiz L, Miranda C, Muga R, Tor J, Sanvisens A, Berenguer J, de Quirós JC, Miralles P, Ochaíta JC, Conde MS, Cuellar IG, Schacke MR, Oretga BP, Vidaurreta PG, Vidal F, Peraire J, Viladés C, Veloso S, Vargas M, López-Dupla M, Olona M, Sirvent JJ, Aguilar A, Soriano A, Aldeguer JL, Juliá MB, Rodrigo JL, Salavert M, Montero M, Calabuig E, Cuéllar S, García JG, de la Serna IB, de Rivera JM, Rillo MM, Lopez JR, Ramírez ML, Pareja JF, Arribas B, Castro JM, Vargas FX, Valero IP, de los Santos I, Sanz JS, Rodríguez J, Aparacio AS, Cepeda CS, Oteo JA, Blanco JR, Ibarra V, Metola L, Sanz M, Pérez-Martinez L, Moraza JP, Dalmau D, Manzanera AJ, Llobell MC, Puig DI, Ibáñez L, Montañez QJ, Valls MX, Martinez-Lacasa J, Velli P, Font R, Boneta JS, Uriz J, Castiello J, Reparaz J, Arraiza MJ, Irigoyen C, Mozas D, Segura F, Amengual MJ, Penelo E, Navarro G, Sala M, Cervantes M, Pineda V, Moreno S, Casado JL, Dronda F, Moreno A, Elías MJ, López D, Gutiérrez C, Hernández B, Pumares M, Marti P, Sánchez AC, Morell EB, Pérez AM, García FG, Quero JH, Monje AP, Medina LM, Ruiz JP, Guerrero Jdel R, Martin CR, López TP, Montiel JC, Raposo P, González C, Antela A, Prieto A, Losada E, Riera M, Murillas J, Peñaranda M, Leyes M, Ribas MA, Campins A, Villalonga C, Pineda JA, Sánchez ER, de León FL, Macías J, del Valle J, Gómez-Mateos J, Mata R, González JS, Solero MM, Ramos IV, Muñoz RP, Viciana P, Leal M, López-Cortés LF, Trastoy M.
Author Disclosure Statement
No competing financial interests exist.