
Abstract
Recent studies have shown that rosuvastatin significantly decreases serum levels of inflammatory biomarkers and slows progression of carotid atherosclerosis in the general population. However, there are no data about its effect on progression of atherosclerosis in HIV-infected patients. Adult patients with HIV infection, on stable antiretroviral therapy, with asymptomatic carotid atherosclerosis and hypercholesterolemia, who started a rosuvastatin treatment at 10 mg daily during the period 2007–2009 were enrolled and followed-up for 24 months. Thirty-six patients (30 males) were enrolled, with a mean age of 49 years, a mean duration of current antiretroviral therapy of 38 months, and a mean 10-year risk of myocardial infarction of 18.5%. Rosuvastatin led to a significant decrease in mean values of intima-media thickness in all extracranial carotid arteries, with the greatest magnitude observed in carotid bifurcations (a mean decrease of 18.7% in the right artery and of 21.4% in the left artery) and in internal carotid arteries (a mean decrease of 23.7% in the right artery and of 25.6% in the left artery). Moreover, there was a significant reduction in mean levels of total cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides versus respective baseline values associated with a significantly decreased mean cardiovascular risk. The treatment with rosuvastatin was well tolerated, and serious adverse events were not reported. A 24-month treatment with rosuvastatin in HIV-infected patients on highly active antiretroviral therapy (HAART) with subclinical atherosclerosis and a moderate cardiovascular risk seems to promote significantly favorable changes in carotid atherosclerosis, associated with a favorable effect on serum lipid levels and a good tolerability profile.
Introduction
S
The association of HIV infection and HAART with premature subclinical atherosclerosis was shown in several case-control and cohort studies using carotid ultrasonography to assess the intima-media thickness (IMT), 4 –7 even though other published investigations have failed to find an atherogenetic effect of HIV infection and antiretroviral treatment. 8 –10 Certainly, hyperlipidemia is a frequent metabolic side effect induced by antiretroviral agents, particularly ritonavir-boosted protease inhibitors (PIs), and it may favor the premature occurrence of atherosclerosis in HIV-positive individuals. 2,3
Statins inhibit hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase and cholesterol synthesis in the liver, leading to a significant reduction in plasma total and low-density lipoprotein (LDL) cholesterol levels, associated with a significantly decreased incidence of cardiovascular disease. 11 Moreover, some of the favorable effects of statins are associated with their antiinflammatory and immunological properties. 12,13
Rosuvastatin, a highly effective statin in lowering plasma total and LDL cholesterol levels, 14 reduces plasma level of C-reactive protein 15 and slows progression of carotid IMT 16 in the general population.
An observational study was performed in HIV-infected patients with hypercholesterolemia and subclinical carotid atherosclerosis to assess changes in carotid IMT after a 24-month treatment with rosuvastatin at 10 mg daily. This is the first study, to the best of our knowledge, evaluating the effect of statins on the atherosclerosis progression in HIV-positive subjects.
Materials and Methods
The Cardiovascular Risk in HIV-infected Patients (RiCHIV) Study is a cross-sectional study conducted between May 2007 and October 2009 in a population of HIV-infected adult subjects referring to our tertiary care outpatient center. The study was approved by the ethics committee of our hospital, and preliminary results regarding evaluation of cardiovascular risk factors and carotid IMT in a subgroup of 66 subjects were previously published. 7
During the study period, 135 patients (Table 1) naive or treated with antiretroviral therapy underwent an ultrasound investigation of the extracranial carotid arteries (common, internal, and external arteries) using a Philips HDI 5000 power color-Doppler with 7.5-MHz probes (Koninklijke Philips Electronics, Eindhoven, The Netherlands). Of the 135 participants enrolled in the RiCHIV study, 42 subjects (Table 2) receiving antiretroviral therapy had asymptomatic carotid atherosclerosis and hypercholesterolemia, were naive to a lipid-lowering therapy, and started a treatment with rosuvastatin (given at 10 mg daily) during the study period. Carotid atherosclerosis was defined as a carotid IMT ≥0.9 mm, in conformity with the guidelines of the European Society of Cardiology. 17 Hypercholesterolemia was defined as a persisting (of at least 3-month duration), fasting LDL cholesterol level above the value requiring drug therapy according to the National Cholesterol Education Program Guidelines. 18
SD, standard deviation; AIDS, acquired immunodeficiency syndrome; HAART, highly active antiretroviral therapy; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BMI, body mass index; MI, myocardial infarction; NCEP, National Cholesterol Education Program. 18
SD, standard deviation; AIDS, acquired immunodeficiency syndrome; HAART, highly active antiretroviral therapy; NNRTIs, nonnucleoside reverse transcriptase inhibitors; PIs, protease inhibitors; CPK, creatine phosphokinase; BMI, body mass index; NCEP, National Cholesterol Education Program. 18
Rosuvastatin was chosen among currently available statins because of its high efficacy and low risk of pharmacokinetic interactions with antiretroviral agents. The dosage of 10 mg daily was chosen in conformity with international guidelines regarding statin therapy in patients receiving HAART. 19,20
This group has been enrolled in the present observational study, assessing changes in carotid atherosclerosis after a 24-month therapy with rosuvastatin. Inclusion criteria were age 18–70 years, proven HIV-1 infection, receiving antiretroviral therapy for ≥12 months, asymptomatic carotid atherosclerosis at baseline ultrasonography, hypercholesterolemia, and initiation of rosuvastatin treatment (10 mg daily) within 3 months after the baseline ultrasonography. Exclusion criteria were clinical history of coronary heart disease, cerebrovascular disease (including transient ischemic attack, amaurosis fugax, or stroke), or peripheric vascular disease; unilateral/bilateral carotid occlusion, or stent implantation or endoarterectomy; previous endovascular intervention; current infectious or inflammatory disease; diabetes mellitus; known alcohol abuse or drug addict; hypothyroidism; Cushing's syndrome; acute or chronic myopathy; acute or chronic kidney diseases; acute or chronic hepatitis or liver cirrhosis; alanine aminotransferase (ALT) or aspartate aminotransferase (AST) >80 U/liter; creatinine >1.2 mg/dl; creatine phosphokinase (CPK) >150 U/liter; underlying treatment with corticosteroids, androgens, estrogens, growth hormone, thiazide diuretics, beta-blockers, thyroid preparations, proton pump inhibitors, acid-reducing agents, or lipid-lowering drugs; and pregnancy or lactation.
All subjects underwent a three-monthly clinical and laboratory examination, including hematology testing, measurement of plasma glucose, triglycerides, total cholesterol, LDL cholesterol, and high-density lipoprotein (HDL) cholesterol levels, CD4 lymphocyte count, and HIV-1 RNA viral load (with a lower limit of detection placed at 50 bDNA copies/ml). Physical examination included evaluation of body mass index (BMI), waist circumference, and blood pressure. Traditional risk factors for coronary artery disease, and presence of lipodystrophy syndrome and/or metabolic syndrome, were carefully evaluated. The 10-year risk for myocardial infarction in all considered patients was estimated by the Framingham equation (available at the following on-line address:
Carotid ultrasonography was repeated within 2 months after the end of the 24-month follow-up. In each ecographic evaluation, the patients were placed in a supine position after at least 10 min of acclimatization in a comfortable room. The common carotid, the bifurcation, and at least the first 2 cm of the internal carotid arteries were evaluated in the short and long axis during the telediastolic phase. During the investigation, the head of the patient was hyperextended and extrarotated from the opposite side. The morphological investigation of the carotid lesions was performed using both ultrasonography and the ultrasound power color-Doppler to better characterize the profile of the lesion and the IMT. The presence of carotid plaque was defined when IMT was above 1.2 mm. The interpreters of carotid IMT were blinded to the patients' clinical data. Intraclass correlation coefficients within and between observers were 0.86 and 0.89, respectively.
Data are presented as mean±standard deviation (SD) for descriptive data, while comparisons between groups were performed by Student's t test or Fisher exact test (where appropriate). The significance of changes in carotid IMT were assessed using the paired Student's t test. Associations between demographic, lifestyle, and laboratory variables and changes in carotid IMT were examined using linear regression models. A two-tailed p value<0.05 was considered significant. The post hoc sample size calculation showed that 31 patients were needed to achieve 80% power with a 5% significance level. The primary outcome of this study is change in the carotid IMT after a 24-month treatment with rosuvastatin, which could become an important therapeutic target of the statin therapy in dyslipidemic patients with atherosclerosis. Secondary outcomes are change in lipid parameters and incidence of adverse events associated with the lipid-lowering treatment.
Results
Study inclusion criteria were met by 42 patients who were enrolled in the study, but six patients were excluded from the final evaluation because they showed a low adherence (<95%) to rosuvastatin therapy and/or they missed one or more laboratory or clinical assessments during the 24-month follow-up.
Demographic, clinical, and laboratory characteristics of study patients are summarized in Table 3. Differences between the 42 enrolled patients and the 36 evaluated subjects are not statistically significant regarding all considered parameters (data not shown). Mean age±standard deviation (SD) was 49.3±16.2 years, 30 patients (83.3%) were men, and 34 (94.4%) were white. The percentage of current smokers was 58.3%, the prevalence of hypertension was 52.8%, and one-third of patients had a family history of coronary heart disease. Therefore, the enrolled subjects showed a moderate mean 10-year risk of myocardial infarction (mean risk above 18%), as shown in Table 4.
SD, standard deviation; AIDS, acquired immunodeficiency syndrome; HAART, highly active antiretroviral therapy; NNRTIs, nonnucleoside reverse transcriptase inhibitors; PIs, protease inhibitors; CPK, creatine phosphokinase; BMI, body mass index; NCEP, National Cholesterol Education Program. 18
Mean change, mean change month 12 and 24 versus baseline value.
p-value, p value month 12 and 24 versus baseline value.
By Framingham equation (available at
SD, standard deviation; LDL, low-density lipoprotein; HDL, high-density lipoprotein; NCEP, National Cholesterol Education Program 18 ; MI, myocardial infarction; n.a., not applicable; IMT, intima-media thickness.
Among the 36 evaluated patients, the mean duration±SD of hypercholesterolemia was 6.2±1.7 months. The mean duration±SD of current antiretroviral therapy was 38.1±15.6 months, and plasma HIV viral load was undetectable in 29 subjects (80.6%). Ongoing protease inhibitor (PI) therapy included atazanavir/ritonavir in 11 cases (30.6%), lopinavir/ritonavir in seven cases (19.4%), and fosamprenavir/ritonavir in two cases (5.6%), while the current nonnucleoside reverse transcriptase inhibitor (NNRTI) was efavirenz in 12 cases (33.3%) and nevirapine in four cases (11.1%).
With regard to the carotid ultrasonography, after 12 months of rosuvastatin treatment there were evident but not statistically significant reductions in mean values of IMT in carotid arteries compared with respective baseline values (Table 4). In particular, the mean changes±SD were −0.09±0.04 mm in the right common carotid artery (p=0.065) and −0.06±0.04 mm in the left common carotid artery (p=0.074); −0.11±0.05 mm in the right carotid bifurcation (p=0.058) and −0.09±0.07 mm in the left carotid bifurcation (p=0.078); and −0.04±0.02 mm in the right internal carotid artery (p=0.081) and −0.02±0.03 mm in the left internal carotid artery (p=0.113). At the same time, the decrease in the prevalence of carotid plaques was not significant (from 22/36 or 61.1% to 17/36 or 47.2%; p=0.067).
However, after 24 months of therapy with rosuvastatin there were statistically significant decreases in mean values of IMT in all extracranial carotid arteries compared with respective baseline values (Table 4). The most significant reductions in IMT were observed in carotid bifurcations (a mean IMT decrease of 18.7% in the right artery and of 21.4% in the left artery) and in internal carotid arteries (a mean IMT decrease of 23.7% in the right artery and of 25.6% in the left artery) (Fig. 1). Significant reductions in mean IMT were registered also in common carotid arteries (−16.5% in the right artery and −18.4% in the left artery). Similarly, the percentage of patients with carotid plaques decreased significantly (from 61% to 28%).
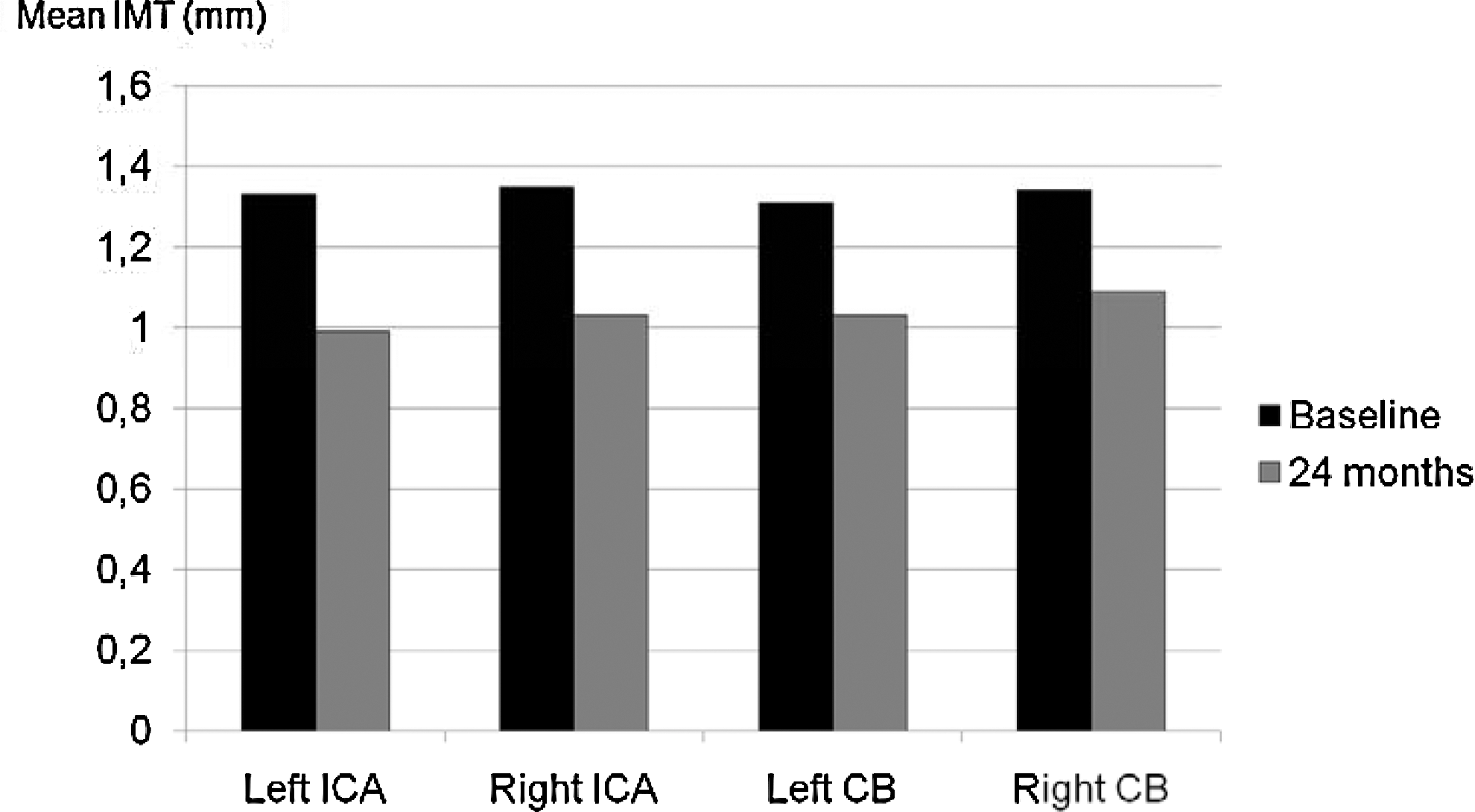
Changes in mean values of carotid intima-media thickness after the 24-month treatment with rosuvastatin among the 36 patients who completed the follow-up (IMT, intima-media thickness; ICA, internal carotid artery; CB, carotid bifurcation).
At the end of 24-month follow-up, 22 out of 36 patients (61.1%) showed changes in carotid IMT beyond a repeatability of±0.2 mm in all the evaluated arteries.
Changes in carotid IMT among all the 42 enrolled patients (by the intent-to-treat analysis) at month 24 are shown in Table 5. The 24-month treatment with rosuvastatin led to a significant decrease in mean values of IMT in all extracranial carotid arteries compared with respective baseline values even in this group.
Mean change, mean change month 24 versus baseline value.
p-value, p value month 24 versus baseline value.
By Framingham equation (available at
SD, standard deviation; LDL, low-density lipoprotein; HDL, high-density lipoprotein; NCEP, National Cholesterol Education Program 18 ; MI, myocardial infarction; n.a., not applicable; IMT, intima-media thickness.
The other modifiable cardiovascular risk factors of the enrolled patients did not change significantly during the follow-up. After 24 months, the number of smokers was 18 (50%), while the number of patients with arterial hypertension and receiving antihypertensive drugs was unchanged (19; 52.8%).
Predictors of change in carotid IMT after rosuvastatin treatment were also evaluated. In linear regression models adjusted simultaneously for all independent variables, age, smoking, hypertension, metabolic syndrome, and plasma lipid levels (total cholesterol, LDL cholesterol, and triglycerides) were significant predictors of change in IMT value, while sex, family history of coronary heart disease, BMI, lipodystrophy syndrome, CD4 lymphocyte count, and HIV viral load were not (Table 6).
All risk factors were simultaneously adjusted for each other in a single regression model.
CHD, coronary heart disease; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
Rosuvastatin led to a statistically significant reduction in the mean level of total cholesterol, LDL cholesterol, and triglycerides after both 12 and 24 months of treatment versus respective baseline values, while changes in mean HDL cholesterol level were not significant (Table 4 and Fig. 2). At the end of the 24-month statin therapy, LDL cholesterol goals were met by 26 (72.2%) out of the 36 enrolled patients, and the mean 10-year risk of myocardial infarction was significantly lower than the baseline risk. Similarly, significant changes in lipid parameters were reported among all the 42 enrolled patients by the intent-to-treat analysis (Table 5). At the same time, mean CD4+ lymphocyte count and percentage of patients with undetectable plasma HIV viral load did not significantly change during hypolipidemic treatment (data not shown).
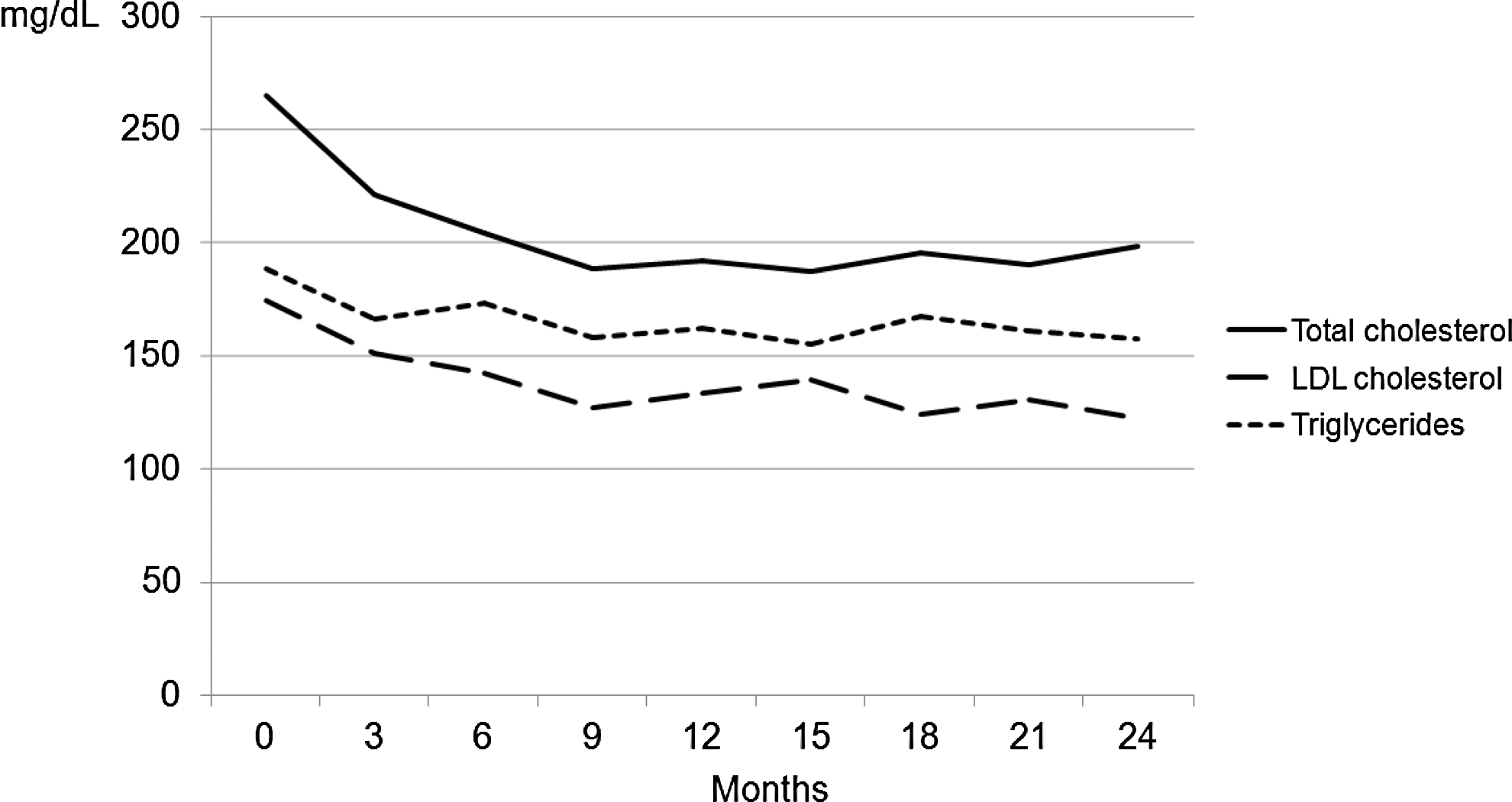
Changes in mean values of total cholesterol, LDL cholesterol, and triglycerides after the 24-month treatment with rosuvastatin among the 36 patients who completed the follow-up (LDL, low-density lipoprotein).
Throughout the 24-month follow-up, the treatment with rosuvastatin was well tolerated and serious toxicity, necessitating discontinuance of statin therapy, was not reported. No treatment-related serious adverse events leading to death or hospitalization were observed during the entire study period. No patients had clinically significant or severe elevations (>10 times beyond normal upper limits) in serum CPK levels or serum hepatic transaminases. Adverse events not associated with statin discontinuation occurred in eight patients (22.2%) and were represented by an asymptomatic elevation in CPK levels (<4 times the upper limit of normal) in three patients (8.3%), mild gastrointestinal symptoms in three patients (8.3%), and transient fatigue with headache in two subjects (5.5%).
Discussion
Rosuvastatin is a highly efficacious statin in reducing plasma levels of LDL cholesterol and favorably modifying the other lipid and apolipoprotein variables in subjects with hypercholesterolemia, as shown in clinical trials with both short-term and long-term follow-up. 21,22 In particular, the multicenter, randomized, open-label STELLAR trial demonstrated that rosuvastatin given at 10 to 40 mg daily was significantly more effective in lowering non-HDL cholesterol, apolipoprotein B, and all lipid and apolipoprotein ratios than milligram-equivalent doses of atorvastatin and milligram-equivalent or higher doses of simvastatin and pravastatin in 2,268 adult patients with hypercholesterolemia. 14
In addition to its non-HDL cholesterol-lowering effects, statins showed antiinflammatory properties by reducing serum levels of inflammatory biomarkers, such as the C-reactive protein (CRP), leading to a more significant decrease in the risk of cardiovascular events. 13,23,24 In the randomized, double-blind, placebo-controlled METEOR trial, rosuvastatin (40 mg daily) lowered significantly serum CRP levels compared with placebo after a 2-year follow-up in 984 adult patients with low cardiovascular risk, subclinical atherosclerosis, and elevated LDL cholesterol.
The decrease in CRP levels was independent of the effects of rosuvastatin on LDL cholesterol levels. 15 The randomized, double-blind, placebo-controlled JUPITER trial investigated the effects of rosuvastatin 20 mg daily versus placebo on rates of nonfatal cardiovascular events in 15,548 apparently healthy adult patients during a maximum follow-up of 5 years (median, 1.9 years). Patients enrolled in this trial had a serum CRP value ≥2 mg/liter. In subjects starting rosuvastatin therapy, achievement of target concentrations of LDL cholesterol less than 1.8 mmol/liter (<70 mg/dl) and CRP less than 2 mg/liter was associated with a significant improvement in event-free survival compared with achievement of neither target or with achievement of reduced LDL cholesterol alone. 25
A frequent question about the potential antiinflammatory effect of statins is whether or not it is secondary to their lipid-lowering action. Certainly, the two possibilities are not mutually exclusive, but statins have several effects on the cellular mediators of inflammation and immunity that may be partially responsible for their efficacy in preventing cardiovascular events. In particular, statins inhibit isoprenoid synthesis through the mevalonate pathway, which is a common mechanism for many antiinflammatory effects. Moreover, they block inflammatory responses of endothelial cells and T lymphocytes by inducing Kruppel-like transcription factors, inhibit T cell proliferation and interferon γ expression by inhibition of T cell KLF2 gene expression, and induce apoptosis of human T and B lymphocytes. Therefore, statins show many different effects that diminish innate and adaptive immune responses, leading to a reduced systemic inflammation and chronic immune activation. 26,27
Statins have also been shown to slow the progression or even promote favorable changes in atherosclerotic disease. 28 This slowing of progression or induction of regression by statins has previously been demonstrated for carotid atherosclerosis by ultrasonographic assessment of carotid IMT, 29 which has been found to be an independent risk factor for a cardiovascular event in patients with atherosclerotic occlusive disease. 30
In the METEOR trial, the rate of change in maximum carotid IMT has been assessed by B-mode ultrasound for 12 carotid sites among the 984 participants receiving rosuvastatin 40 mg daily or placebo over 2 years. The mean change in maximum carotid IMT during the follow-up was −0.0014 mm/year for the rosuvastatin group versus +0.0131 mm/year for the placebo group. Rosuvastatin therapy resulted in a statistically significant decrease in the rate of progression of maximum carotid IMT compared to placebo, while it did not induce a favorable change. 31
To evaluate the effect of lower doses of rosuvastatin on carotid IMT, 45 adult patients with hypercholesterolemia and asymptomatic carotid atherosclerosis on baseline ultrasound investigation were treated with rosuvastatin 10 mg daily for 24 months. At the end of follow-up, rosuvastatin treatment induced a significant reduction in both left (−26.6%) and right (−22.2%) mean carotid IMT, in association with a significant improvement in plasma lipid levels and a good tolerability profile. 32
In the randomized, open-label, blinded-endpoint JART Trial, the mean percentage change in the carotid IMT has been evaluated in 348 adult Japanese patients with elevated LDL cholesterol and a maximum carotid IMT ≥1.1 mm, who were randomized to receive rosuvastatin (5 mg daily) or pravastatin (10 mg daily) for 12 months. Rosuvastatin significantly slowed progression of carotid IMT at 12 months compared with pravastatin: the mean percentage changes in the mean IMT were 1.91% in the rosuvastatin group and 5.8% in the pravastatin group, with a statistically significant difference of −3.89% between the groups. 16
The efficacy and safety of rosuvastatin have also been evaluated in HIV-infected patients receiving HAART with hypercholesterolemia because of its favorable pharmacokinetic properties, even though available data in this population are still limited. In fact, it is not expected to have frequent and clinically significant interactions with PIs, because only 10% of this statin is metabolized by the CYP 2C9 isoenzyme into N-desmethyl rosuvastatin. 33,34
Rosuvastatin therapy (at 10 mg daily) for 24 weeks in 16 HIV-positive subjects treated with PIs and with persisting hypercholesterolemia (total cholesterol ≥240 mg/dl) led to a significant reduction in median values of total cholesterol, LDL cholesterol, and triglycerides versus respective baseline values, without significant clinical or laboratory adverse events. 35 In a randomized, open-label trial including 94 HIV-infected patients receiving a stable PI-based antiretroviral therapy and with persisting hypercholesterolemia (total cholesterol >250 mg/dl), the lipid-lowering effect of rosuvastatin (10 mg daily), atorvastatin (10 mg daily), or pravastatin (20 mg daily) has been evaluated. After 12 month of statin therapy, decreases in mean serum level of total and LDL cholesterol were significantly greater with rosuvastatin than with atorvastatin or pravastatin, with a good tolerability profile across the three groups. 36 A randomized trial investigated the lipid-lowering effect of rosuvastatin (10 mg daily) compared with pravastatin (40 mg daily) in 83 HIV-positive subjects treated with boosted PIs. After 45 days of statin treatment, rosuvastatin led to a significantly greater reduction in median levels of LDL cholesterol (−37%) and triglycerides (−19%) than pravastatin (−19% and −7%, respectively), without renal, hepatic, or muscular serious adverse events. 37
The antiinflammatory and immunological effects of statins have also been investigated in the setting of HIV infection, and in some, but not all, studies they have been found to inhibit HIV replication in vitro. 38 –41
A 45-day treatment with rosuvastatin or pravastatin significantly reduced the median serum level of CRP (from 3 to 2.4 mg/liter) in 58 dyslipidemic HIV-infected individuals receiving HAART. 42 In a randomized, double-blind, placebo-controlled crossover trial, the effect of atorvastatin on plasma HIV-1 RNA levels and cellular markers of immune activation has been investigated in 22 HIV-infected patients not receiving antiretroviral therapy. An 8-week therapy with high-dose atorvastatin (80 mg daily) resulted in significant reductions in the circulating proportion of activated T lymphocytes (CD4+ HLA-DR+, CD8+ HLA-DR+, CD8+ HLA-DR+ CD38+ T cells), while HIV RNA levels were unaffected by the statin treatment. Moreover, the decrease in markers of immune activation did not correlate with the reduction in serum levels of LDL cholesterol. 43
In a recent retrospective cohort study we have evaluated the antiinflammatory effect of rosuvastatin (10 mg daily), atorvastatin (10 mg daily), and pravastatin (40 mg daily) in 151 HIV-infected patients receiving a boosted PI-based antiretroviral therapy and with persisting hypercholesterolemia. After 12 months of lipid-lowering therapy, all statins led to a significant decrease in serum levels of CRP and tumor necrosis factor-α (TNF-α), without a correlation between inflammation markers and lipid parameters. However, patients treated with rosuvastatin had a significantly greater reduction in total cholesterol and LDL cholesterol levels than those treated with atorvastatin or pravastatin. 44
Few of the above-mentioned works stress the small number of available data about the antiinflammatory effect of statins in HIV-infected patients on HAART, and the lack of studies evaluating the effect of these agents on progression of atherosclerosis in the setting of HIV disease.
This is the first work, to the best of our knowledge, assessing the effect of statins on the progression of atherosclerosis in an HIV-positive population. In our observational study including 36 HIV-positive adults on HAART with a moderate cardiovascular risk, a 24-month therapy with rosuvastatin at low dosage (10 mg daily) resulted in a significant decrease in mean IMT in all extracranial carotid arteries in comparison to respective baseline values, with the greatest magnitude observed in carotid bifurcations and in internal carotid arteries. Significant predictors of change in carotid IMT were age, smoking, hypertension, metabolic syndrome, and plasma lipid levels (total cholesterol, LDL cholesterol, and triglycerides). With regard to lipid-lowering efficacy and drug safety, rosuvastatin led to a significant decrease in mean serum levels of total cholesterol, LDL cholesterol, and triglycerides, in the absence of serious clinical or laboratory adverse events, as shown in the above-mentioned studies. Moreover, at the end of the 24-month follow-up, LDL cholesterol goals were met by more than 70% of the enrolled patients, and the mean 10-year risk of myocardial infarction decreased by more than 45%, compared with the baseline risk.
Obviously, there are several limitations to our study, which is only observational and does not have a control group. Patients with cardiovascular diseases and high cardiovascular risk have been excluded from the study because they usually need a stronger intervention concerning lifestyle and a combined lipid-lowering therapy. This exclusion could be a selection bias for the evaluation of the true efficacy of the agents employed. On the other hand, the enrolled patients have a moderate cardiovascular risk, and we cannot determine whether the effect of rosuvastatin is the same in patients with a low risk. Moreover, the concomitant antiretroviral therapy is not the same, and this difference could certainly influence the lipid-lowering effects of the statin.
In conclusion, rosuvastatin seems to promote a regression of carotid atherosclerosis in HIV-infected patients on HAART with a moderate cardiovascular risk, but further randomized trials are certainly required to better investigate the effect of statins in slowing atherosclerotic progression in the setting of HIV infection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.