
Abstract

Editor: A 34-year-old previously healthy HIV+ man was started on Atripla (daily combined tenofovir 300 mg/emtricitibine 200 mg/efavirenz 600 mg) for a declining CD4 T cell count in February 2009. His HIV plasma RNA levels declined to <50 copies/ml within 5–8 months and remained at <50 copies/ml for the next year and his CD4 T cell rose (Fig. 1). He gained excess weight after starting Atripla and purchased over-the-counter orlistat (Xenical) from his local pharmacy in September 2010 to lose weight.
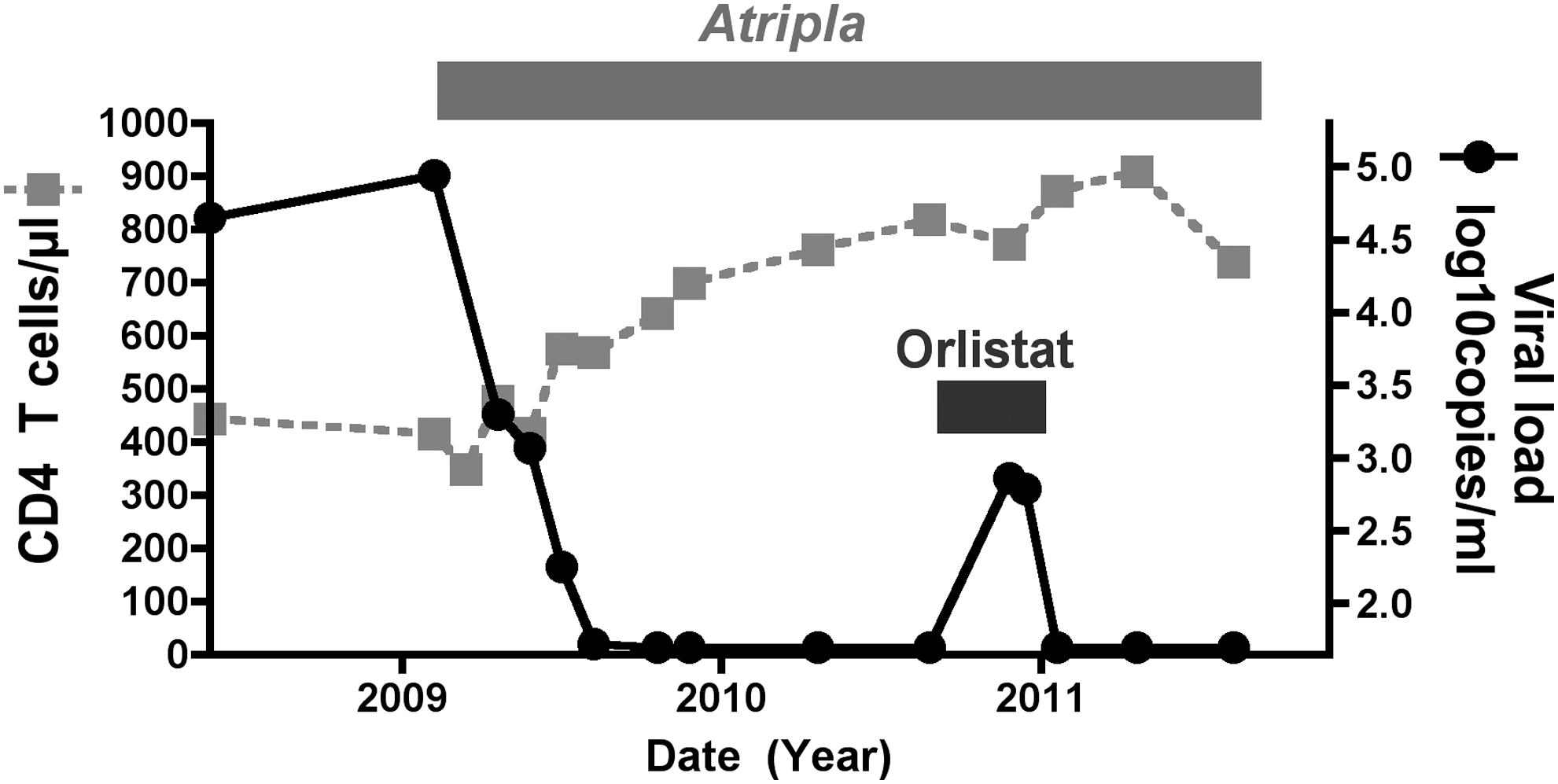
Temporal relationship between Orlistat use and recrudescence of HIV viremia. Serial viral load and CD4 T cell counts are shown in relationship to starting Atripla and the use of Orlistat.
He took three 60 mg tablets per day at each meal for the first month and then one 60 mg tablet a day at the evening meal thereafter. As expected he had mild diarrhea and steatorrhea, particularly after ingesting fatty foods, and he did lose some weight. At his next review for his HIV infection in December 2010 his HIV RNA level had risen to 722 copies/ml. His HIV viral load was repeated 1 week later and was 612 copies/ml. The patient vigorously claimed to be perfectly adherent to his Atripla dosing. Orlistat was ceased and his HIV RNA level declined back to <50 copies/ml when tested 3 weeks later and has remained at that level since then. An HIV genotype test on the blood sample with 722 copies/ml showed no drug resistance mutations.
Orlistat is a reversible inhibitor of lipases that diminishes absorption of fats and is available over the counter in many countries. Orlistat causes a 30–60% reduction in absorption of the fat-soluble vitamins beta-carotene and vitamin E acetate and 2–12% of subjects treated with orlistat develop abnormally low levels of vitamins A, D, E, or beta-carotene. 1 Preliminary studies suggest orlistat reduces blood levels of lipophilic drugs such as cyclosporine and amiodarone, and possibly thyroxine and lamotrigine. Small studies of drug–drug interactions of orlistat with digoxin, glyburide, nifedipine, oral contraceptives, phenytoin, fluoxetine, and statin drugs suggest no significant interactions. 2 No studies have been reported on the effect of orlistat on levels of antiretroviral medications.
Efavirenz is highly lipophilic and absorption might be expected to be reduced by orlistat, the most probable cause of the loss of virologic control observed in the case described. A report in rats also suggests that orlistat can damage the brush border of the small intestine and cause lymphocyte migration into the small intestine. 3 This might lead to increased CD4 T cell targets in the gut mucosa or result in enhanced microbial translocation and immune activation, any of which could increase HIV replication. 4
Obesity is a growing global problem, including HIV-infected subjects on antiretroviral treatment, 5 and recent studies document the partial success of orlistat in achieving weight loss. 6 This case highlights a temporal relationship between orlistat use and loss of control of HIV viremia that resolved when orlistat was discontinued. Fortunately, antiretroviral resistance did not result from the modest and transient elevation of HIV viremia detected, although this might be expected to occur if viremia continued. Studies on the interaction between orlistat and antiretrovirals are needed. In the interim, orlistat should be used with caution in subjects with HIV infection, particularly subjects taking efavirenz-based regimens.
Footnotes
Author Disclosure Statement
No competing financial interests exist.