
Abstract

E
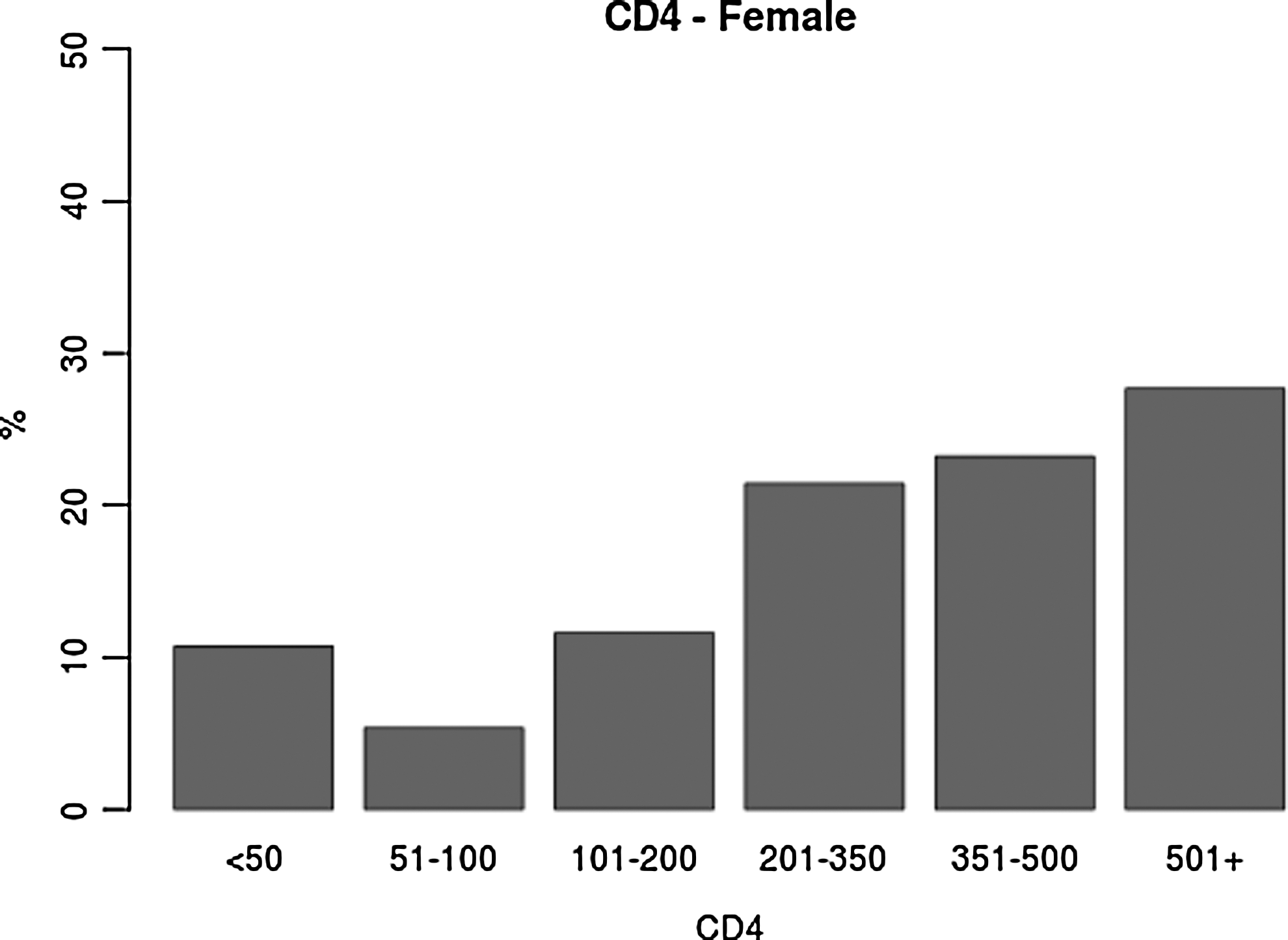
In 1996 Brazil became the first developing country to ensure free and universal access to ART to all HIV-infected individuals who fulfill locally developed treatment guidelines, which recommend treatment for all individuals with CD4 counts <350 cells/mm3. Additionally, frequent public health campaigns stimulate repeat HIV tests, which are freely available at numerous voluntary counseling and testing sites (VCT) throughout the country. An ethics committee-approved prescreening protocol allows the VCT site at the Federal University of Rio de Janeiro to refer individuals found to be HIV positive to the clinical trials unit (CTU) located one floor above. At the CTU these individuals receive counseling and information on ongoing trials, are offered free CD4 counts, and provide limited demographic data. Over 95% of the individuals found to be HIV positive at the VCT go to the CTU and have a CD4 count performed. All individuals 18 years of age or older who indicated that they had just learned of their HIV positive serostatus and who attended the CTU between September 12, 2011 and March 9, 2012 are the object of the present report. A total of 483 individuals [371 males (77%), 112 (23%) females] fulfilled inclusion criteria. The median and interquartile ranges (IQRs) for ages were 33 (19–68) and 37 (20–64) for males and females, respectively (Wilcoxon rank sum test p-value < 0.001). The median and IQRs for CD4 counts were 365 (5–1929) and 358 (13–1180) for males and females, respectively (p=0.26); 7.3, 12.4, 22.6, and 47.7% of males and 10.7, 16.1, 27.7, and 49.1% of females had CD4 counts <50, <100, <200, and <350 cells/mm3, respectively (Chi-square test p-value=0.63; Fig. 1).
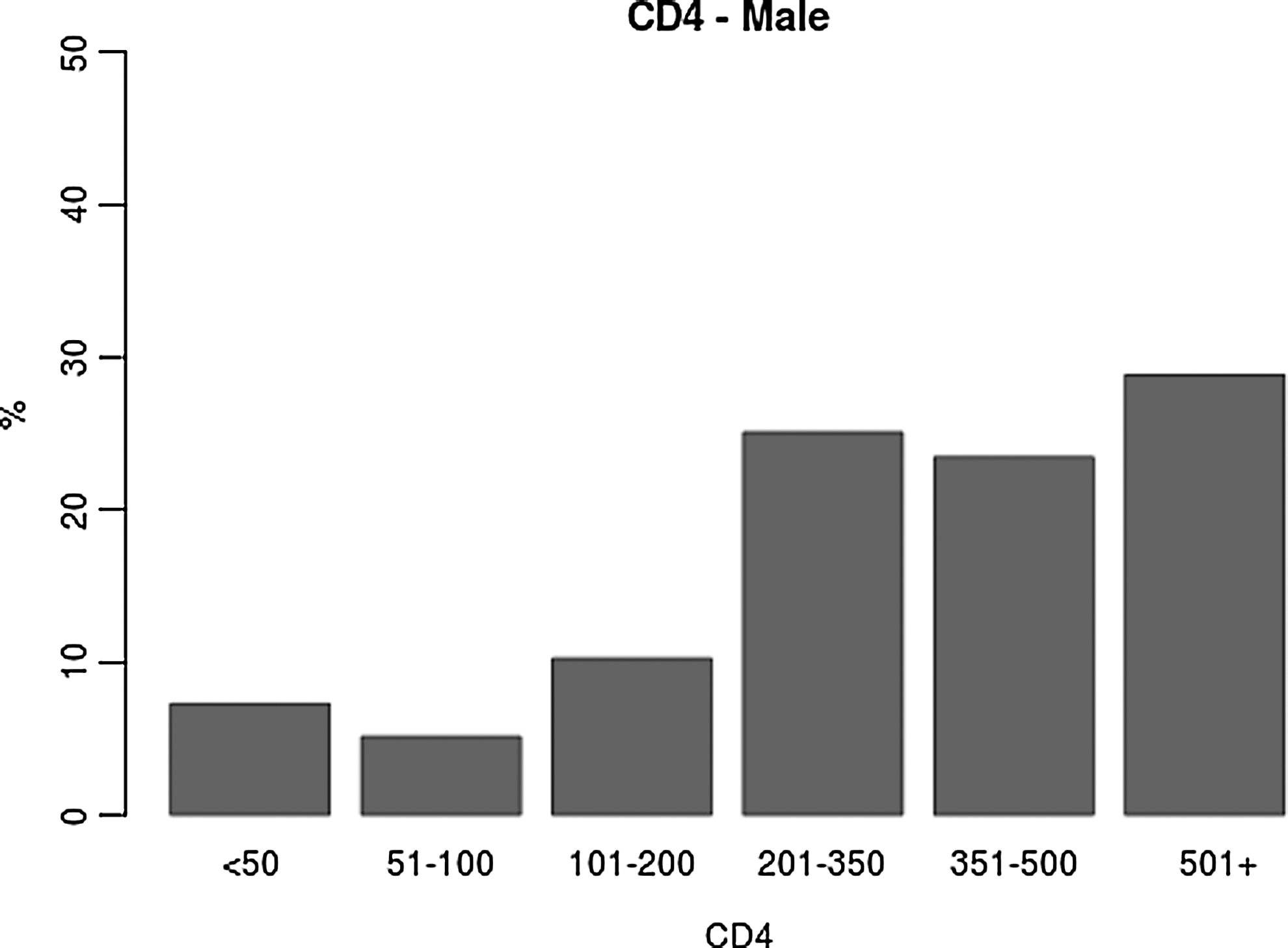
CD4 cell count distribution in 371 men and 112 women recently diagnosed with HIV infection.
In the United States, surveillance data indicate that approximately one-third of HIV-infected persons present late (CD4 count <200 cells/mm3) for HIV testing, a figure that has remained virtually unchanged for the past decade. 5 Studies from Western Europe estimate that 24–39% of HIV-infected patients present for care at advanced stages of disease (AIDS and/or CD4 cell count <200/mm3). 1,6,7 There are very limited published data on the first CD4 count among individuals recently diagnosed with HIV infection in Brazil. 8 Our data indicate that despite free access to diagnosis and treatment, a considerable proportion of adult men and women learn of their HIV-positive serostatus at advanced stages of immune deficiency.
Although the design of the study and the limited demographic information that could be obtained for this IRB-approved prescreening protocol do not allow us to determine how representative of the entire country the studied population is, our data suggest that in Brazil and in several developed countries public health and programmatic interventions leading to earlier HIV diagnosis and initiation of ART could substantially improve patient outcomes and have a major impact on the future of the epidemic.
Footnotes
Acknowledgments
We would like to thank Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) for their support.
Author Disclosure Statement
No competing financial interests exist.