
Abstract
Monitoring HIV subtype distribution is important for understanding transmission dynamics. Subtype B has historically been dominant in Australia, but in recent years new clades have appeared. Since 2000, clade data have been collected as part of HIV surveillance in South Australia. The aim of this study was to evaluate the prevalence of and risk factors for HIV-1 non-B subtypes. The study population was composed of newly diagnosed, genotyped HIV subjects in South Australia between 2000 and 2010. We analyzed time trends and subtype patterns in this cohort; notification data were aggregated into three time periods (2000–2003, 2004–2006, and 2007–2010). Main outcome measures were number of new non-B infections by year, exposure route, and other demographic characteristics. There were 513 new HIV diagnoses; 425 had information on subtype. The majority (262/425) were in men who have sex with men (MSM), predominantly subtype B and acquired in Australia. Infections acquired in Australia decreased from 77% (2000–2003) to 64% (2007–2010) (p=0.007) and correspondingly the proportion of subtype B declined from 85% to 68% (p=0.002). Non-B infections were predominantly (83%) heterosexual contacts, mostly acquired overseas (74%). The majority (68%) of non-B patients were born outside of Australia. There was a nonsignificant increase from 1.6% to 4.2% in the proportion of locally transmitted non-B cases (p=0.3). Three non-B subtypes and two circulating recombinant forms (CRFs) were identified: CRF_AE (n=41), C (n=36), CRF_AG (n=13), A (n=9), and D (n=2). There has been a substantial increase over the past decade in diagnosed non-B infections, primarily through cases acquired overseas.
Introduction
HIV-1
Historically, HIV subtypes and CRFs have been broadly linked with geographic location and risk group. 8 However, subtype distribution of the global HIV pandemic has diversified extensively through mutation and recombination, partly driven by a combination of population mobility, sexual mixing, and the impact of antiretroviral therapies. 3,9 Subtype and CRF differences have been linked to disease progression, transmission route, pathogenicity, transmissibility, accuracy of current diagnostic assays, response to therapy, and development of drug resistance mutations. 3,5,10,11 Other factors can also influence these characteristics, which makes it difficult to establish the independent effects of subtype, but this variability potentially has major clinical and epidemiological significance. 3,12
Surveillance systems have been in place since the beginning of the global pandemic, and in recent years have incorporated molecular epidemiology as a tool both for surveillance of HIV-1 genetic diversity and to monitor transmission and geographic pathways of genetic variants. 3,13 –15 For example, recent mapping of HIV strains in Asia revealed a large genetic diversity, including two new CRFs and transmission of new recombinant HIV-1 subtypes. 14,16
Historically, subtype B has predominated in Western countries 5,6 where transmission is primarily through male-to-male sex. 6,8,17 However, subtype B accounts for only 11% of global HIV infections, 9 and the prevalence of non-B infections in Western countries is increasing. Recent studies in France have found non-B prevalence rates of 42–48% in newly diagnosed HIV infections. 18 In Italy, non-B prevalence rates rose from 25% in 2000 to over 60% in 2008, with African ethnicity and heterosexual acquisition as independent predictors. 6 In a Washington cohort the non-B prevalence rate was 13%, 13 and in one broad population-based study in the United States a national non-B prevalence rate of 5.1% was reported in newly diagnosed infections. 19 In a very recently published Australian study, Chibo and Birch (2012) found a non-B prevalence rate of 22% in a Victorian cohort. 20
Parallel to this genetic diversity, there are increasing data on subtype-specific differences, related to genotyping, transmission efficiency, disease progression, vaccine development, and drug therapy. 12,21 Though subtype B has always accounted for a relatively small percentage of the total pandemic, it has historically been the predominant global reference clade for assay development, drug resistance testing, and antiretroviral susceptibility. 1,5,13
In 2000, South Australia became the first state to integrate drug resistance testing as part of the routine HIV reporting and surveillance system. The resulting data provide the first analysis of Australian trends and molecular epidemiology of HIV subtype distribution over the past decade. We report a pattern of increasing non-B subtypes in South Australia, though subtype B still characterizes the predominant HIV infection in this cohort.
Materials and Methods
Surveillance system for HIV in South Australia
AIDS and HIV notification was commenced in South Australia in 1985 and 1991, respectively. For each new person diagnosed, a standardized form is completed, which includes demographic, epidemiological, and clinical information. Where possible, an in-depth interview is also conducted.
In 2000, South Australia became the first jurisdiction to conduct routine genotypic and drug resistance testing as part of an enhanced surveillance system. This genotype information is housed on a separate database, but is linked to the notification system via patient number. The South Australian Health Department is the custodian of both databases. For the current study, the two databases were merged to create a combined dataset. Patient identifiers such as name and address were removed, and limited demographic, epidemiological, and clinical data were retained, including gender, age, reported continent of birth, reported exposure route, and reported location of infection acquired (overseas/Australia). This study was approved by both the South Australian Health and Flinders University Research Ethics Committees.
Study population and design
Five hundred and thirteen people newly diagnosed with HIV between 2000 and 2010 were identified from the South Australian HIV notification database, and 425 were retrospectively selected from this dataset according to the following inclusion criteria: no previously documented positive diagnosis and a plasma-derived RNA pol sequence available for genotyping, taken within 12 months of diagnosis. For each patient, notification data, including location where the infection was acquired, were collected through a standardized form and interview at the time of diagnosis, as part of the routine notification protocol.
HIV-1 genotyping
Blood was collected for routine drug resistance testing, viral load, and CD4+ cell count. Due to the number of routine samples, patient plasma was stored at −20°C until genotyping. Past experience has demonstrated negligible degradation of virus nucleic acid. Viral RNA was extracted and a 1098 nucleotide fragment of the pol gene that encompasses the protease and reverse transcriptase genes was sequenced in both directions, using RT-PCR and dye terminator sequencing with standard commercial reagents. Sequences were assembled and proofread to obtain a contiguous sequence using Kodon 2.4 (Applied Maths, Sint-Martens-Latem, Belgium). The entire sequence was submitted to the Stanford HIV Drug Resistance Database for the determination of virus subtype and for drug resistance interpretation. Although phylogenetic and subtype analysis was carried out on the entire 1098 nucleotide fragment of the pol gene, only the protease region was used in subsequent epidemiological analyses for simplicity. Sequences used in these analyses have been assigned the GenBank accession numbers KC237881-KC238305.
Statistical methods
HIV genetic and notification data were linked and analyzed using subtype as the dependent variable, and year, country of origin, where infection was acquired, reported risk exposure, and age as explanatory variables. Notification data were aggregated into three time periods (2000–2003, 2004–2006, and 2007–2010) of relatively equal numbers and with significant power to conduct statistical tests. Categorical variables were analyzed using chi square tests-for-trend and Fishers exact test to identify subtype-specific characteristics. Multivariate analysis was performed using logistic regression. Variables used are described in Table 1. Significance levels were set at p≤0.05. All data were analyzed using the software package Stata 10.1 (StataCorp LP, College Station, TX).
Unknown: insufficient information in the database.
Data represents number (%) of subjects. MSM, men who have sex with men; Percentages in last column are proportion B compared to non-B. Genotyped sample was representative of the total population diagnosed.
Results
South Australian HIV population; genotype
There were 513 reported diagnoses between 2000 and 2010, and 425 (83%) had genotypes determined. The annual number of diagnoses has remained relatively stable over the past 11 years (mean=47/year). Demographic and other characteristics of those for whom genotypes were obtained (n=425) were very similar to those for the total diagnosed population (n=513, Table 1). There were 101 cases (24%) of HIV non-B subtypes among these genotyped specimens (Fig. 1). The most common non-B infection was CRF_AE (41) followed by subtype C (36), CRF_AG (13), subtype A (9), and subtype D (2).
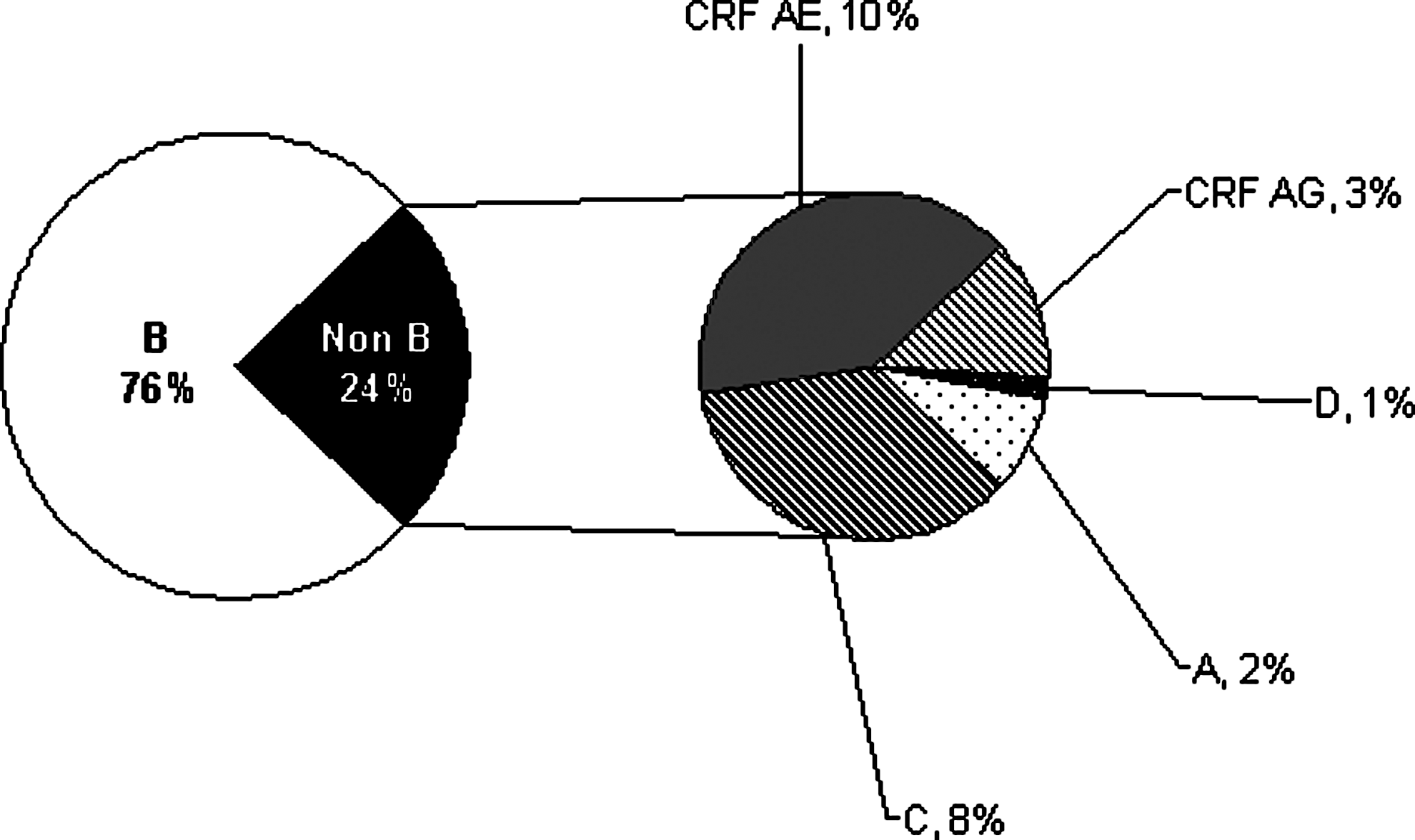
Proportion HIV-1 subtypes in new diagnoses between 2000 and 2010.
Though new diagnoses in South Australia have remained stable over time, there has been a significant change in subtype distribution within newly diagnosed individuals. The proportion of non-B infections increased from 15% (2000–2003) to 21% (2004–2006) to 32% (2007–2010) (p=0.002). In 2010, the proportion of non-B infections was 47% (Fig. 2).
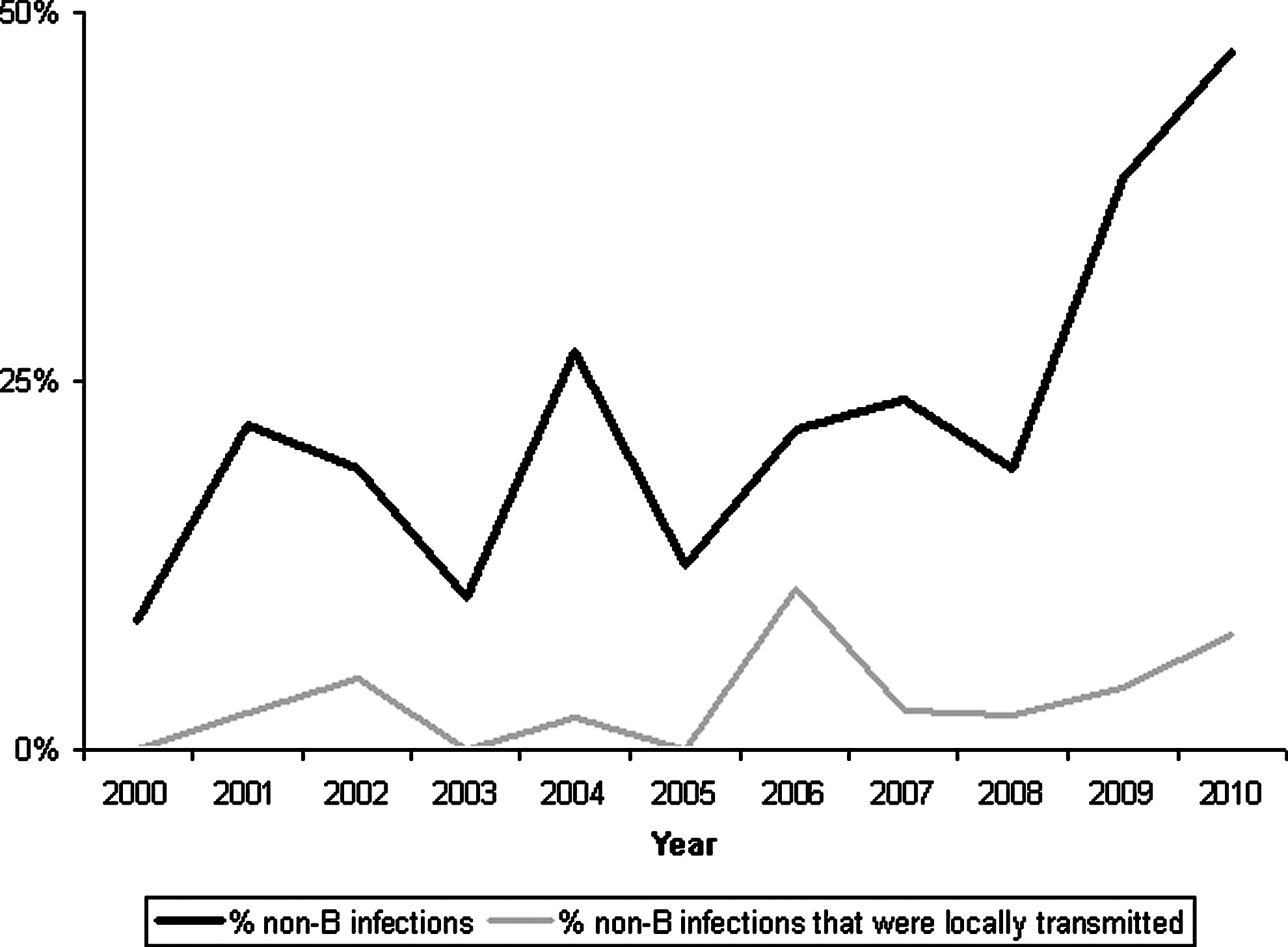
Proportion of non-B diagnoses in Australia between 2000 and 2010, including local transmission.
Location infection acquired
As well as an increase in non-B subtypes over time, there was a significant increase in the proportion of infections acquired overseas from 23% (2000–2003) to 37% (2007–2010) (p=0.006). When analyzed by subtype, 85% of the 101 non-B infections were reported to be acquired overseas and were composed of 95% (34/36) of the total subtype C infections, 81% (36/41) of the CRF_AEs, 77% (10/13) of the CRF_AGs, 89% (8/9) of the As, and 50% of the (1/2) Ds.
In contrast to non-B infections, only 10% of the 324 B infections were acquired overseas (p<0.0001).
Among the 72% of cases (305/425) determined to have been acquired within Australia, 95% were clade B (Table 1). However, new local non-B diagnoses have increased from two cases in the first time period to six in the second and seven in the third (Fig. 2). Of these 15 local transmissions, nine were female and six reported being born in Australia. Of the six males who acquired HIV locally, four reported being born in Australia.
Reported risk exposure, gender, and age at diagnosis
The majority of genotyped subjects were men who have sex with men (MSM) (62%), although the proportion has dropped from 72% (2000–2003) to 61% (2004–2006) and 55% in the most recent time period (2007–2010). Correspondingly, the proportion of reported heterosexually acquired HIV increased from 27% (2000–2003) to 35% (2004–2006) and 40% (2007–2010).
Of the 262 genotyped MSM infections, nearly all (97%) were subtype B, and 90% were acquired in Australia. The remaining 10% acquired overseas were nearly all subtype B, but three had CRF_AE. Of the 146 genotyped heterosexual infections, 43% were subtype B (Table 1) and 43% (63/146) were acquired in Australia. The remaining 57% acquired overseas were nearly all (89%) non-B (36% C, 35% CRF_AE, 18% A/D/CRF_AG). The proportion of female infections was significantly higher in the non-B cohort (36% or 36/101) compared to the B cohort (6% or 18/324) (p<0.0001).
Approximately one-tenth of genotyped patients (45/425) were under the age of 25 years when diagnosed (32 males and 13 females). The observed frequency of non-B infections in the <25 years cohort was 64% greater than expected, compared to B infections in the same cohort (20% smaller than expected) (p=0.01). The majority (77%) of the 13 young females had a non-B infection, in comparison to 25% of the young males.
Region of origin
People born in Australia constituted 57% (240/425) of the genotyped cohort and subtype B accounted for 88% (211/240) of these infections (Table 1). Of these Australian born subtype B patients, 77% (163/211) were acquired in Australia. In contrast, of the 12% (29/240) of Australian born people with a non-B infection, 66% acquired their infection overseas.
One hundred (24%) people in the genotyped cohort were born overseas while 20% had no recorded country of birth. In the overseas born white population, subtype B accounted for 81% of European born people (21/26), of which 91% were acquired in Australia. Subtype B accounted for 86% of American born people (6/7), but half of these infections were acquired overseas. All non-B infections in both European and American born individuals were acquired overseas.
Nearly all (40/43) African born people had a non-B infection and 98% of these were acquired overseas. The predominant non-B infection was C (51%), followed by CRF_AG (21%), A (16%), CRF_AE (2%), and D (2%). Two-thirds (16/24) of Asian born people had a non-B infection and 75% of these were acquired overseas. The predominant non-B infections were CRF_AE (63%), C (19%), CRF_AG (13%), and A (5%).
Subtype associations with comparator variables
Multivariate logistic regression analyses were conducted, taking subtype B infections as the baseline group for comparison and controlling for other independent variables (acquired overseas, heterosexual, overseas born, and age <25 years).
As shown in Table 2, there was a strong association between subtype C and overseas acquisition, with subtype C infections 34 times more likely than subtype B to be acquired overseas (95% CI 5.8–192.0, p<0.0001). Non-B infections were 17 times more likely to be acquired overseas compared to B infections (95% CI 6.9–42.6, p<0.0001). Non-B infections were almost 21 times more likely than B infections to be acquired through reported heterosexual transmission (95% CI 7.5–57.0, p<0.0001), which rose to 44 times more likely for subtype C cases (95% CI 5.0–384.6, p=0.001). Non-B infections were almost four times more likely (95% CI 1.5–9.9, p=0.006) among people born overseas, though this was not significant for CRF_AE infections alone (95% CI 0.7–7.9, p=0.146). The age at diagnosis of HIV infection was not different between B and non-B patients, except in the “Other” category, which was subtype A, D, and CRF_AG (p<0.05). There were 24 patients with A, D, or CRF_AG: four born in Australia, 17 born in Africa, and three born in Asia. Of these, 38% were under 25 years of age at detection of infection; 75% (3/4) from Australia, 24% (4/17) from Africa, and 66% (2/3) from Asia.
95% CIs are indicated in parentheses.
Proportion of subtype B infections was used as the baseline for comparison. All associations in the first three columns were statistically significant at p<0.05 except born overseas and CRF_AE (p<0.146). In the age column, only the association between other and age <25 was significant (p<0.05). Non-B includes all non-B subtypes and CRFs. Other consists of subtypes A, D, and CRF_AG. MSM, men who have sex with men.
Discussion
This is the first Australian study to investigate genotypic diversity and trends in subtype distribution of the HIV epidemic over the past 10 years. At present, no formal national HIV-1 molecular surveillance program exists in Australia. However, South Australia has implemented routine baseline drug resistance testing, providing viral sequence data combined with notification information to yield an enhanced comprehension of South Australian HIV molecular epidemiology. 21 As HIV continues to evolve, migration patterns change, and tourism increases, it is important to monitor this geographic diversity in order to understand and respond to transmission patterns. 5,17
Despite ongoing programs and improved access to testing and treatment, the rate of new HIV infections remains stable. However, differences were identified in subtype prevalence, place of acquisition, region of birth, gender, and age at diagnosis. The main finding of this study is that the proportion of non-B infections has increased in Australia over the past decade. Non-B patients represented approximately a quarter of the cases in this study, but this proportion had risen to nearly half of all new diagnoses in 2010. This is similar to a European report in which more than 60% of new infections were non-B in 2008. 6
The current study demonstrates that patients infected with B or non-B subtypes represent highly distinct populations. The majority of B-infected people were MSM, while non-B infections were mainly heterosexually acquired and just over a third of were female. Most B infections were acquired in Australia by people born in Australia while the majority of non-B infections were acquired overseas by people born overseas or people traveling to areas of high HIV prevalence. 5,6 These figures are comparable to findings by Chalmet et al. (2010) in Belgium, in a similar sized cohort. 22
White MSM with locally acquired subtype B continue to represent the largest HIV risk group in South Australia, supporting epidemiological trend analyses in Australia, Canada, Europe, and the United States. 15,21 –25 There is also a small subset of MSM acquiring non-B infections overseas and locally, reflecting findings in the U.K. 8 and the recent Victorian study. 20 Though national HIV incidence has remained stable in the MSM population over the past decade, the proportion of undiagnosed infections in South Australia is estimated to be around 20%. 26
On a global scale, heterosexual transmission is the major route of HIV infection. 27 In South Australia we are seeing a shift in the epidemic toward this: a decrease in the local representation of MSM and an increase in the representation of heterosexual men and women, including a large proportion from sub-Saharan Africa. This shift has also been noted in Europe. 28 Since 2000, heterosexually acquired infections have doubled to nearly half of all new diagnoses, not quite as high as the 4-fold increase seen in the U.K. since 1996. 21 Most non-B patients contracted HIV by heterosexual contact, and a small number through male-to-male sex. The proportion of women infected with subtype B was very low; this can be partly explained by the high representation of MSM in the B cohort, while the majority of females acquired their infection overseas where non-B subtypes are more frequently circulating. Despite the apparent shift in the South Australian epidemic toward increasing heterosexually acquired non-B HIV infections, MSM are still a critical at-risk population that justifies a continued prevention and intervention focus for scientists, program experts, and policy makers. 15
Corresponding with an increase in heterosexual infections, there has been a significant increase in imported non-B infections, through migration or travel to countries where there is a high prevalence of HIV. Though the numbers are small, there is evidence of non-B local transmission, predominantly found in females. A significantly higher proportion of non-B patients was diagnosed under the age of 25 compared to the B cohort, though when location acquired, country of birth, and risk behavior were controlled for, this was significant only for subtype A, D, and CRF_AG patients. These clades are common in Africa and Asia, where two-thirds of these young patients were born. Patients born in Africa reported sexual contact as their risk exposure while the two patients born in Asia were both under 10 years of age, with overseas medical procedure cited as the risk exposure.
Transmission of non-B subtypes and CRFs is rapidly expanding geographically, and the rise in non-B diagnoses may be a marker of more recent transmission events—some attributed to tourism and some to importation by people born in high prevalence countries where multiple subtypes and CRFs circulate.
Over half of the global HIV population is infected with subtype C, 4,29,30 which is dangerously uncontrolled in Africa and India. Subtypes A and B follow, then CRF_AG and CRF_AE, the latter predominantly found in Asia. 9,30 In our cohort, subtype C accounted for fewer than 10% of total infections but over a third of non-B infections. Nearly all were reportedly acquired overseas, and though information on a specific country was not available, a large percentage of these patients originated from Africa.
The predominant non-B infection was CRF_AE, with prevalence in the genotyped cohort twice that of the 5% global average, and almost all cases reportedly were acquired overseas. Hemelaar et al. found global CRF infections increased by over 50% between 2000 and 2007, 9,30 and the current study reflects this temporal CRF increase; almost half the AE infections were diagnosed in 2007–2010. Unlike subtype C, nearly half the patients were born in Australia and were most likely the result of acquisition during overseas travel to Asia.
Subtypes A, D, and CRF_AG are predominantly found in Africa, with a combined global prevalence rate of 10%. 9 Though prevalence was relatively low in our cohort, nearly all were diagnosed in the latter time period, and were acquired overseas by people of African origin, possibly reflecting the increase in Australian migration from this region. A number of Australian born heterosexual men and women also imported or locally acquired subtypes D and CRFs AE and AG.
These findings have public health implications, both for targeting specific at-risk populations and assessing the potential increase of non-B subtypes within the domestic HIV-1 epidemic. 1
There are scarce data available on subtype differences and even fewer data available on non-B subtypes in developing countries where they are the major infection type. There is growing evidence, however, that suggests HIV strains do differ from each other in terms of virulence, transmission, or rate of progression. 4 A 10-year prospective study in Senegal found female sex workers with a non-A subtype had a significantly shorter AIDS-free survival time. 31 A 2010 London study found a CD4 cell decline 4-fold faster in subtype D patients, and a higher virological rebound at 6 months, after adjustment for baseline, gender, and ethnicity. 21 A study of Kenyan women found a >2-fold higher risk of mortality and faster rate of CD4 cell decline in D patients compared with A, after adjustment for viral load, 32 and in a Ugandan cohort, subtype D patients tended to develop AIDS earlier. 33 In Rakai, the median time to onset and risk of progression to death were significantly shorter for subtype D and CRF patients compared with A. 11 Each of these studies concluded that HIV disease progression is affected by subtype and that this may have an impact on decision and policy making in terms of initiation of therapy and future vaccine trials. 11,21,32
Understanding genetic diversity is very important for the treatment of non-B subtypes. Many researchers now agree that though it appears subtypes and CRFs are equally sensitive to treatment, transmitted polymorphisms present before therapy may affect subtype-specific pathways of secondary resistance. 12 This combined with suboptimal therapy and poor adherence in developing countries makes them a prime target for accelerated drug resistance, both acquired and transmitted. 34 Current drug regimens targeted against subtype B may not be equally effective long term for non-B subtypes and may lead to faster drug resistance. 27
Interpreting and reporting surveillance data can be problematic. Reporting newly acquired infections does not demonstrate true reductions or increases in the wider community; HIV diagnoses represent only the subgroup of people who have willingly been tested and had an HIV-positive result. These individuals are often those who have easy access to medical health services and are concerned about their own risk behavior. 35 Immigrants, visa holders, and refugees still face barriers to accessing health services for screening and treatment of HIV, arising from stigma, financial restrictions, limited support systems and English skills, and residency concerns. 28,35 Refugees in particular may be difficult to reach because of traumatic life experiences prior to arrival in Australia.
This is a major concern as the UN recognizes migrants as one of the groups most vulnerable to HIV, and overseas born people now comprise a third of HIV notifications in Australia. 28,36 These issues along with a continuing influx of new arrivals from high HIV prevalence and low/middle income countries are likely to lead to an underestimate of HIV infections in these populations, a possible increase in local transmission of non-B subtypes, and poor treatment adherence, which could lead to transmitted drug resistance. 1,36
The global spread of HIV diversity is highly dynamic with regard to epidemiological factors such as risk group and geographic location; it continually generates through mutation and recombination, and then travel and migration assist in the transfer of this diversity between populations. 21 Our analyses focused exclusively on pol, as it is routinely used for drug resistance testing, and provided the largest possible reference dataset of B and non-B subtype sequences. We note that further subtype validation should be conducted with alternative HIV genes, such as env. 37 Ongoing surveillance and a deeper understanding of HIV variation, including factors and molecular mechanisms that affect transmission, replication, and resistance, are crucial for the development of appropriately targeted subtype-specific prevention and treatment options for populations most at risk. 5,9,21,29 Further evidence of subtype differences could drastically change the way we respond to the HIV epidemic.
Footnotes
Acknowledgments
The authors would like to thank Michael Kidd, Peter McDonald, Stuart Shapiro, and Bob Seamark for helpful discussions and comments during the course of this project. K.G.H. is supported by an Australian Post Graduate Award. Presented in part at the Australasian Society for HIV Medicine Annual Scientific meeting Canberra, ACT, Australia, September 2011.
Author Disclosure Statement
No competing financial interests exist.