
Abstract
One hundred patients have been enrolled in the CTA (ambulatory treatment center) of Brazzaville, Republic of Congo, from February to April 2011: 41 naive individuals and 59 patients at failure of first line regimen [two nucleoside reverse transcriptase inhibitors (NRTIs) plus one nonnucleoside reverse transcriptase inhibitor (NNRTI)]. Phylogenetic analysis of HIV-1 isolates allowed identification of subtypes and circulating recombinant forms (CRFs). The drug resistance mutations (DRMs) in reverse transcriptase and protease were analyzed in both subpopulations. Globally, 92 viruses were characterized, exhibiting a high diversity of HIV-1 with a majority of undetermined recombinant forms (URF) followed by CRF02_AG, CRF37_cpx, G, A1, B, D, H, and several other subtypes and CRF: F1, A2, C, CRF13_cpx, CRF11_cpx, CRF20_BG, CRF21_A2D, CRF33_01B G, CRF02_AG, CRF37_cpx, and A1. In naive patients, DRMs were observed with percentages ranging from 4% to 9% depending on drug classes. In treated patients at failure, numerous DRMs could be noted that induce actual or potential resistance to major NRTIs and NNRTIs.
Introduction
HIV-1
According to UNAIDS in 2010, the prevalence of adults living with HIV in the Republic of Congo was 3.4% (77,000 people infected). In 2009, 16,011 seropositive patients had a clinical follow-up in medical centers and 11,525 were receiving highly active antiretroviral therapy (HAART).
The high diversity of HIV-1 in this country has already been demonstrated. 4 –9
The aim of this study was to obtain further data on the molecular characterization of HIV-1 in Brazzaville, RC, and to evaluate the prevalence of drug resistance mutations (DRMs) to nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors (PIs) in both naive and treated patients at failure.
Materials and Methods
Patients and samples
The CTA (ambulatory treatment center), which was set up by the French Red Cross in 1994, is the main medical center dedicated to people living with HIV in the Republic of Congo and for the central region of Africa. The active file includes 2004 seropositive individuals (677 men, 1327 women, and 114 children). A total of 1642 individuals are under first line therapy (two NRTIs+one NNRTI) and 103 are under second line therapy (two NRTIs+PI/r).
Seropositivity is determined by two rapid tests: Determine (Alere) and ImmunoCombs (Orgenics). The T cell count is done with Fascount (Becton Dickinson) and the viral load (VL), when available, is determined using Applied Biosystem equipment with Abbott reagents in the laboratory in Pointe-Noire.
From February to April 2011, 100 HIV-seropositive patients were recruited in the CTA in Brazzaville. The population was composed of 41 naive patients and 59 individuals at treatment failure of first line therapy (total: 69 females and 31 males).
The naive patients, named population A, were selected according to the following criteria: adults over 18 years old and providing written informed consent, naive of antiretroviral therapy, asymptomatic (WHO 1 or 2 with loss of weight less than 10%) recently detected, T cell count over 500/μl if available, or recently demonstrated HIV-1 infection by a negative antibody assay within 5 years or an equivalent event (e.g., blood donation).
Forty-one persons were recruited; two were excluded, one because of a HAART treatment after a second check and the other because of a putative date of infection more than 5 years before. The median age of the 39 patients (22 females and 17 males) in population A was 38 years (range from 20 to 71 years).
Population B was composed of adults over 18 years old who provided written informed consent, were under HAART (two NRTIs and one NNRTI, NVP or EFV) for at least 6 months, and who failed on first line therapy as demonstrated by VL>1000 cp/ml and/or according to the WHO clinical and/or immunological criteria.
Fifty-nine persons were recruited and one was excluded, because she was not confirmed to be at treatment failure on the basis of a second T cell count. The median age of the 58 patients (44 females and 14 males) in population B was 41 years (range from 19 to 68 years).
The different therapeutic combinations are presented in Fig. 1. Some patients switched from one regimen to another depending on the side effects experienced. The first scheduled regimen was d4T-3TC-NVP, but the most frequent regimen finally observed was AZT-3TC-NVP.
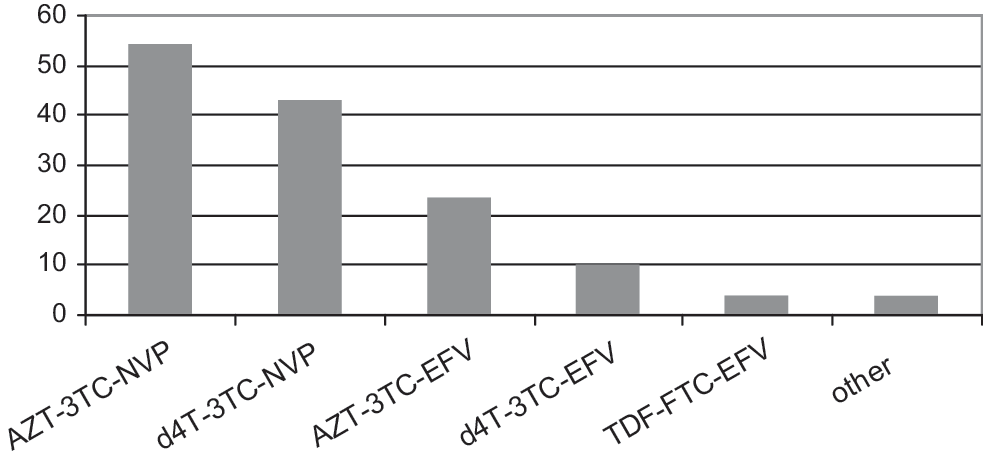
Combination of antiretroviral drugs used to treat patients at failure.
For HIV sequencing, blood samples were collected in ethylenediaminetetraacetic acid (EDTA) tubes and plasma was separated and applied to spots of Whatman 903 filter paper cards with five spots of 50 μl. The samples were allowed to dry at room temperature for 3 to 15 h in the vertical position and were placed in plastic bags with desiccants. They were stored for less than 10 days before dispatch at room temperature to Bordeaux, France (a 48-h journey).
HIV sequence analysis
Molecular characterization was performed with an in-house procedure from dried plasma samples. Viral RNA was extracted using the NucliSENS kit (Biomérieux, France). Two spots were cut with scissors and eluted in 2 ml NucliSENS Lysis Buffer. The samples were then agitated at room temperature for 30 min. RNA was extracted using NucliSENS miniMAG and NucliSENS Magnetic Extraction Reagents (BioMerieux, France).
Reverse transcriptase (RT) and protease (Prot) genes were amplified with primers detailed by ANRS (
PCR products were sequenced on both strands using an Applied Biosystems 3500xls Dx Genetic Analyzer.
The derived nucleotide sequences of the RT and Prot regions were aligned by the Clustal W 2.0.8 alignment program with known reference strains of M, N, and O pooled from the HIV-1 gene databank (
Phylogenetic trees were inferred by the neighbor-joining method from matrix distances calculated after gap stripping of alignments, according to a two-parameter Kimura algorithm. The circular trees (not shown here) were obtained using ITOL (
Genotypic drug resistance
RT and Prot sequences were analyzed for DRMs according to the ANRS algorithm using SmartGene software (SmartGene, Lausanne, Switzerland) and the 2009 update of the international working group for surveillance of transmitted HIV-1 drug resistance. 11
Results
Characteristics of investigated populations
Naive patients (population A)
The mean T-CD4 cell count was 871 cells/μl (range 116–2043). The mean VL was 10.933 copies/ml (range from <400 to 20,500), but only 25 T cell counts and 6 VL values were available. Amplifications were successful for both RT and Prot genes in 25 samples and for only the Prot region in seven samples, while seven other samples could not be amplified either on RT or Prot (Table 1).
RT, reverse transcriptase; Prot, protease; PCR, polymerase chain reaction.
Treated patients (population B)
The mean T-CD4 cell count was 211 cells/μl (range 22–533). The mean VL was 268,962 copies/ml (range from <400 to 9,600,000) with no VL in only one patient. All had a T cell count but rarely very recently. Amplifications were obtained for both RT and Prot genes in 50 samples, for only the Prot region in six and for only the RT gene in one, while another could not be amplified either on RT or Prot (Table 1).
Molecular characterization of HIV-1
We present the data from global naive plus treated populations (Fig. 2). Unique forms (UFs) were predominant followed by CRF02_AG, CRF37_cpx, G, A1, B, D, H, and several other subtypes and CRFs: F1, A2, C, CRF13_cpx, CRF11_cpx, CRF20_BG, and CRF21_A2D.
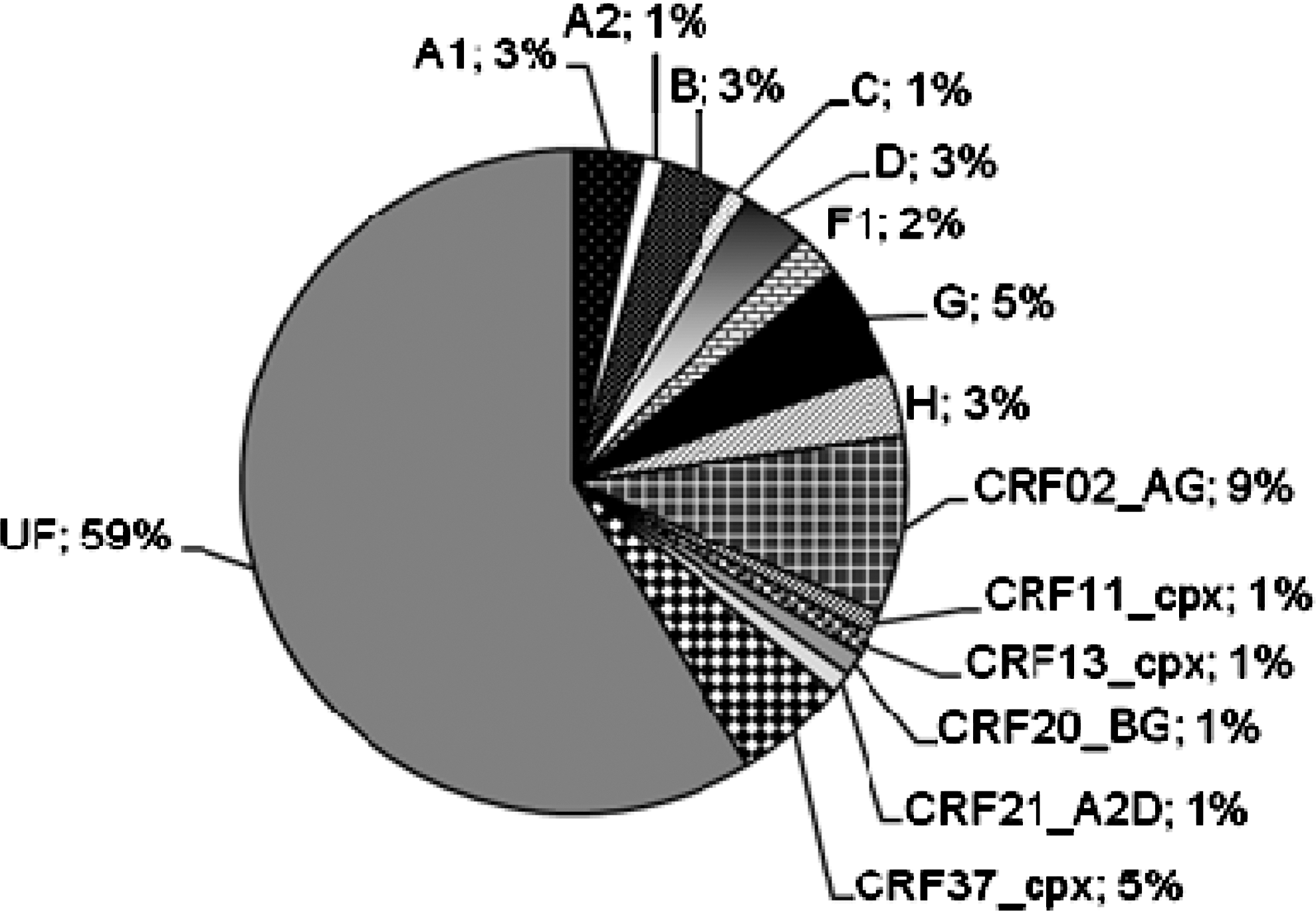
Molecular characterization of HIV-1 isolates from both naive and treated patients.
In some samples where the amplification signal was weak, we used a second set of primers to improve the amplification. Because two different sequences in Prot were observed with these two sets of primers, we concluded that dual infection was highly probable: one in a naive patient with G/UF and UF/UF viruses, and another in a treated patient with CRF16_A2D/CRF09_cpx and UF/CRF09_cpx.
Table 2 shows the UF details.
RT, reverse transcriptase; nb, number; Prot, protease; UF, unique forms.
Drug resistance mutations
Naive patients
One sample (A1 subtype) exhibited a 115F mutation to NRTIs. Resistance mutations to NNRTIs were recorded in two isolates: one UF with 101E and one UF with 103N plus 190A. Regarding resistance to PI, one 90M mutation was observed in the G virus of the dual infection, one 46L in a CRF13_cpx, while the A1 with the 115F mutation was also bearing 46L.
Treated patients
Numerous resistance mutations to NRTIs were observed with a predominance of 184V followed by thymidine-associated mutations (TAMs): 215Y/F, 41L, 67N, 70R, 219Q/E, and 210W. Other mutations observed were 69D/N/S, 74V/I, 44D, 75M/A, 215I/N, and 70E. Nucleotide-associated mutation (NAM) 151M had a prevalence of 1% (Fig. 3).
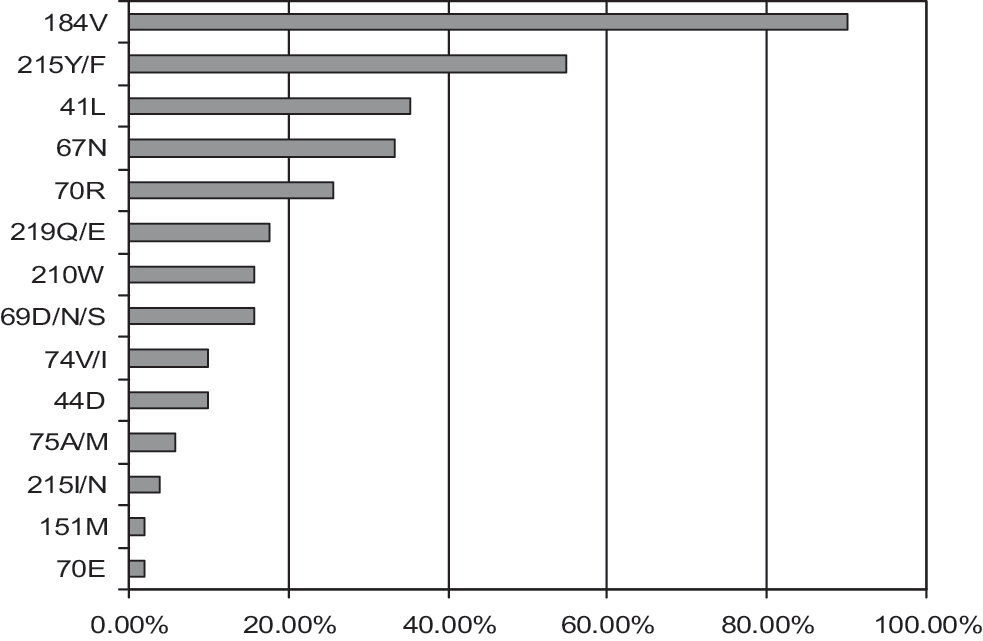
Drug resistance mutations to nucleoside reverse transcriptase inhibitors (NRTIs) in treated patients at failure.
The most predominant mutation to NNRTIs was 103N followed by 181C, 221Y, 98G, 190A/S, 179I/T, 106A, 90I, 101E, 230L, 138A/G, 101H/R, 98S, 106I, 225H, and 181V (Fig. 4).

Drug resistance mutations to nonnucleoside reverse transcriptase inhibitors (NNRTIs) in treated patients at failure.
As shown in Fig. 5 after analysis by the ANRS algorithm and the SmartGene software, these DRMs frequently induce resistance to the drugs of the treatment (d4T/AZT-3TC-NVP/EFV) but also cross-resistance to ABC/ddI (16 isolates out of 50), to TDF (18 out of 50), and to ETV/RTV. Globally (Fig. 6), most of the patients exhibit resistance to three to eight drugs of the NRTI/NNRTI classes.
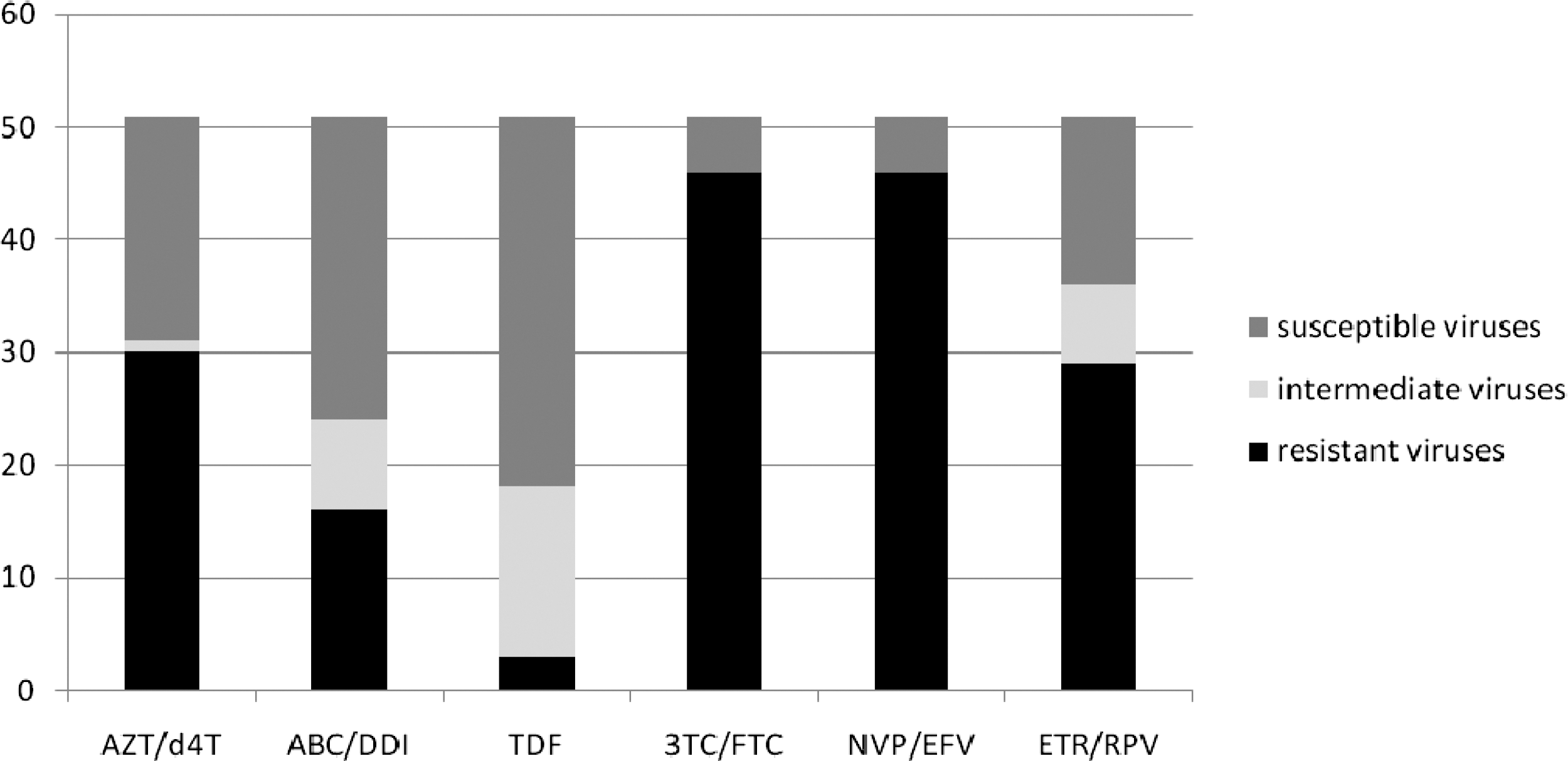
Susceptibility of the isolates from treated patients to major NRTIs and NNRTIs according to the ANRS algorithm and using Smartgene software.
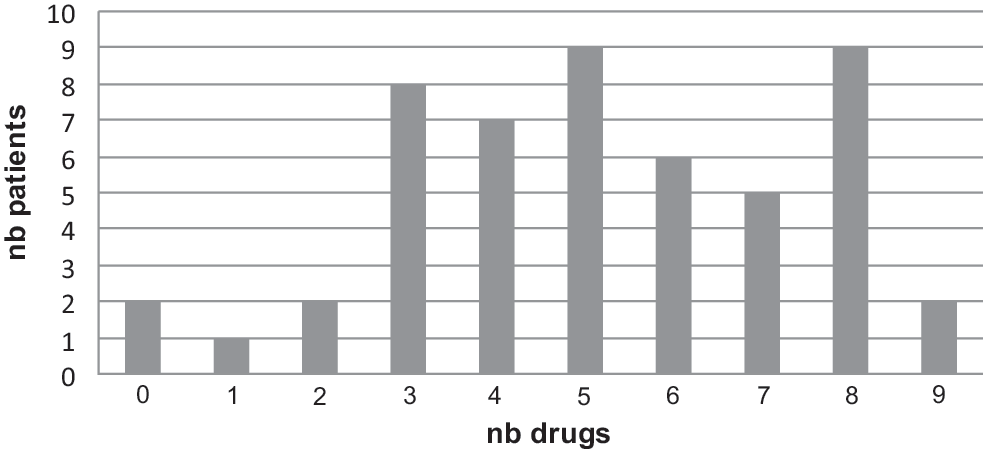
Number of inefficient drugs (NRTIs and NNRTIs) in treated patients at failure.
Only one major resistance mutation to PI (IDV) was observed in this treated population: 46L borne by an F1 virus. Most of the viruses had polymorphic substitutions 36I, 69K, and 89M, which are associated with resistance to TPV by the ANRS algorithm.
Discussion
The extremely high genetic diversity of HIV-1 in RC is again demonstrated in this series. Unlike previous authors, 4 –9 we observed a decrease in the proportion of pure subtypes and an increase in the number of UFs. Eight pure subtypes (28%), A1, A2, B, C, D, F1, G, and H, and seven CRFs, CRF02_AG, CRF11_cpx, CRF13_cpx, CRF20_BG, CRF21_A2D, CRF37_cpx, and many UFs (58%), occurred in this population. The data confirm the predominance of G-like recombinant forms followed by A-like recombinant forms, as previously described. 4 The presence of many UFs may be due to a likely high level of multiinfected individuals, as emphasized by the dual infections observed. Unlike the situation in Cameroon, 12 these UFs are not borne by single individuals but induce apparent subclusters, which might be future CRFs provided that the sequences are checked by full genome sequencing and bootscanning. Moreover, the distribution of genetic diversity in RC is very different compared to Cameroon, 12 where one CRF is predominant (CRF02_AG), and to the Democratic Republic of Congo, 13 where the pure subtypes are predominant (51%) while UFs are 34%.
The prevalence of resistance to NRTIs in naive patients is 4%, to NNRTIs is 8%, and to PI is 9%. RC can be classified as a country with low prevalence <5% to NRTIs and moderate prevalence ≤5% to ≥15% to NNRTIs and PIs, which has been reported in Yaoundé, Cameroon 14 and is higher than in Gabon. 15 Globally, DRMs to NRTIs and NNRTIs were observed in 12% while DRMs to PIs were observed in 9% of the naive patients whose isolates could be investigated by sequencing. While caution is required in interpreting these data owing to the small sample size, these findings point to the need for more extensive studies of transmitted DRMs in RC.
In treated patients at failure, DRMs are relevant to the drugs used. As noted above, these DRMs induce resistance to the drugs of the treatment but also cross-resistance to ABC/ddI, to TDF, and to ETV/RTV. Resistance to TDF has been described in this therapeutic context and can be associated either with TAMs of pathway 1 or K65R; in our series, this potential resistance is associated with TAMs since we have not observed any 65R mutation. Potential resistance to ETV/RTV is often noted in our study and is mainly related to 221Y or 181C+221Y and not to 138A as described in a study carried out in Bangui. 16 Globally, only two patients were found to have a treatment failure associated with viral replication without DRMs and were considered to be unobservant. It can be concluded that viral resistance is the major cause of treatment failure in our study. 17
Footnotes
Acknowledgments
We thank the Ministry of Public Health of RC and the headquarters of Croix-Rouge Française in Paris for permission to undertake this study. H.F. thanks professor P. Debré (former French Ambassador for HIV/AIDS) for his support. We owe sincere gratitude to the personnel of CTA in Brazzaville. This study was supported by CNRS UMR 5234, Université de Bordeaux 2, Bordeaux, France.
Author Disclosure Statement
No competing financial interests exist.