
Abstract
To evaluate the course of liver fibrosis, 328 HIV-hepatitis C virus (HCV)-coinfected patients (210 HCV treated and 118 HCV untreated) were followed-up for 38–42 months. Liver fibrosis was assessed by biopsy or elastometry at baseline and by elastometry afterward, in addition to other noninvasive indexes. A combined liver stiffness stage (LSS) was established and evaluated over time. Eighty patients had sustained virological response (SVR) and 130 had treatment failure (TF) after a standard course of peginterferon-ribavirin therapy. LSS decreased significantly in all fibrosis indexes during HCV therapy in treated patients, but the improvement persisted only in those with SVR. At the end of study, median elastometry values suffered variations of −29%, −5.0%, and +15.4% in SVR, TF, and untreated patients, respectively. Likewise, LSS worsened in 2.5%, 33.1%, and 39% of these groups, respectively: [OR (95% CI) 19.3 (4.4–119), p<0.001] for TF vs. SVR; [24.9 (5.6–154), p<0.001] for no therapy vs. SVR; and [1.29 (0.74–2.3), p=0.40] for no therapy vs. TF. LSS improved in 53.8%, 19.2%, and 5.9% of these groups, respectively: [4.88 (2.51–9.53), p<0.001] for SVR vs. TF; 18.4 (7.17–49.4), p<0.001 for SVR vs. no therapy; and 3.78 (1.47–10.1), p=0.003 for TF vs. no therapy. Independent predictive factors of LSS improvement or worsening were as follows: alcohol abuse [OR (95% CI) 0.48 (0.20–0.99), p=0.047] and [2.45 (1.19–5.03), p=0.016], respectively; SVR [27.7 (6.41–168), p<0.001] and [0.15 (0.07–0.31), p<0.001], respectively; and lower baseline CD4 counts [1.92 (1.08–3.45), p=0.026] and [0.31 (0.15–0.63), p=0.001], respectively. SVR was usually associated with regression of noninvasive liver fibrosis markers, whereas TF and HCV-untreated patients experienced poorer outcomes.
Introduction
L
Virological eradication with therapy is associated with biochemical and histological improvement, and decreased liver-related morbidity and mortality. 1,2 However, an important problem involved in studying changes in liver fibrosis before and after peginterferon-ribavirin involves liver biopsy. Biopsy is often difficult to obtain for sequential monitoring and liver fibrosis staging. Longitudinal assessment of fibrosis over time with transient elastometry in patients with chronic viral hepatitis is becoming routine practice in many clinics. Transient elastometry is noninvasive, easy to perform, and relatively inexpensive, allowing early detection of cirrhosis. 3,4 Changes over time in liver stiffness are insufficiently documented, especially in the coinfected HIV-HCV population.
The aim of this study was to evaluate the course over time of liver fibrosis, measured by noninvasive methods, in a population of HIV-HCV-coinfected patients prospectively followed-up during at least 1 year after the ending of anti-HCV therapy, depending on the response to such a therapy. Additionally, we also compared the results observed in these patients with those of another group of coinfected patients who did not receive anti-HCV treatment.
Materials and Methods
Study patients
This is a longitudinal cohort study of HIV-HCV-coinfected patients who had undergone treatment with either peginterferon alfa-2a or 2b plus ribavirin between 2002 and 2010. Patients enrolled in the study belonged to a large cohort of about 1,165 coinfected individuals previously described 5 ; 310 of them (26.6%) initiated anti-HCV therapy and were in regular follow-up and surveillance of liver fibrosis evolution using transient elastometry since January 2007. Only 210 treated patients fulfilled the following criteria and were included in the study: (1) HIV-1 and HCV infection confirmed by reactive antibodies and positive HCV plasma RNA measurement; (2) no evidence of concomitant chronic hepatitis B; (3) first treatment with peginterferon-ribavirin for at least 12 weeks; (4) liver biopsy available or, alternatively, a liver stiffness measurement by transient elastometry, both before and after anti-HCV treatment; (5) a complete clinical and laboratory evaluation pretherapy and posttherapy and at least 1 year of follow-up after the ending of anti-HCV therapy; and (6) age older than 18 years, and ability to give informed consent.
Likewise, a group of coinfected patients who did not receive anti-HCV therapy underwent similar longitudinal monitoring of liver fibrosis by transient elastometry and liver fibrosis indexes (LFI) calculated from laboratory parameters, in order to compare the course of their liver disease with that of treated patients. These patients did not receive treatment for different reasons, mainly because of no indication of therapy as a result of minor or absent fibrosis, advanced cirrhosis, or refusal to receive treatment in this cohort of intravenous drug users.
In this study, peginterferon-ribavirin dosing and treatment duration were not controlled but reflected the clinical practice of the physician and/or hospital at the time the patients were treated. Data concerning demographic characteristics, biochemical markers, and HIV- and HCV-related variables were collected for all patients just before anti-HCV treatment (baseline), at an intermediate point on treatment (around 12 weeks), at 24 weeks after the end of treatment, and at a further time point at the end of the study (a median of 38 months after baseline).
Patients were classified into three groups: patients with SVR, patients with treatment failure (TF), and patients who did not receive anti-HCV therapy. The first group was composed of 80 patients with undetectable HCV RNA in plasma 24 weeks after stopping anti-HCV therapy. The TF group included the remaining 130 patients who did not attain SVR. The group of untreated patients was composed of 118 consecutive individuals who did not receive anti-HCV therapy.
The study was approved by the hospitals' local ethical committees and all patients gave informed consent at enrollment in accordance with the Helsinki declaration.
Virological assessment
Serological diagnosis of HIV-1 and HCV infection was established by the presence of specific antibodies by enzyme immunoassay (MEIA AxSYM; Abbott Diagnostics, Abbott Park, IL). HIV-1 RNA and HCV RNA were measured by quantitative polymerase chain reaction (Cobas TaqMan; Roche, Mannheim, Germany). The detection limits were 50 copies/ml for HIV-1 and 25 IU/ml for HCV. HCV genotypes were analyzed by line-probe assay (Versant HCV; Siemens, Camberley, UK). Routine biochemical parameters were measured by standardized laboratory methods.
Liver fibrosis assessment
Estimates of liver stiffness were obtained by transient elastometry using FibroScan (EchoSens, Paris, France), performed in all patients since 2007, following previous recommendations. 3 –6 Transient elastometry measurements were performed by two trained nurses unaware of the anti-HCV-treatment status of the patients. Prior to 2007 only patients with a liver biopsy performed within 1 year before the onset of anti-HCV therapy were included, unless an earlier biopsy showed cirrhosis. Therefore these cirrhosis patients were included regardless of the 1-year criteria, as it was clear that they were already in the highest fibrosis stage. The different scoring of liver fibrosis was converted to comparable stages of fibrosis in the METAVIR system, 7,8 establishing four stages: F0F1=no fibrosis or portal fibrosis without septa, F2=few septa, F3=numerous septa without cirrhosis, and F4=cirrhosis. In nonbiopsied patients hepatic fibrosis was scored by transient elastometry results and then combined with the stages of biopsied patients according to the cut-off levels of equivalence previously established by us 5 and others, 3,4,6 although there is no definitive agreement regarding the exact cut-offs. Thus we obtained a final liver stiffness stage (LSS) to classify patients as follows: F0F1: patients with mild or no fibrosis (<7.2 kPa), F2: significant fibrosis (7.2–9.3 kPa), F3: advanced fibrosis (9.4–13.9 kPa), and F4: cirrhosis (>13.9 kPa). When biopsy and transient elastometry were performed in the same patient, elastometry measurement was preferred.
Three well-established LFI, done on the basis of liver inflammation tests, platelets, cholesterol, and age of patients, were calculated by conventional formulas at each evaluation time point. These LFI and their particular cut-off values, as validated previously, 9 were APRI index (<0.5, no or minimal fibrosis, >1.5, significant fibrosis), FIB-4 (<1.45, no or minimal fibrosis and >3.25, significant fibrosis), and Forns index (<4.2, no or minimal fibrosis and >6.9, significant fibrosis).
Statistical analysis
Quantitative variables were expressed as medians and interquartile ranges (IQRs) and qualitative variables as absolute frequencies and percentages. The differences in continuous variables between two independent groups were assessed with the Mann–Whitney U-test and χ2 test (or Fisher's exact test when appropriate) for categorical variables. The differences before and after anti-HCV therapy for paired samples were analyzed by Wilcoxon signed ranks or McNemar tests. Multivariate analyses were carried out with a stepwise logistic regression to evaluate the variables independently associated with changes in LSS staging between baseline and the end of follow-up. A p-value <0.05 for a two-tailed test was considered statistically significant. All calculations were carried out with SPSS 15.0 software (SPSS, Chicago, IL).
Results
Baseline characteristics
A total of 210 HIV/HCV-coinfected patients who initiated anti-HCV therapy and fulfilled the inclusion criteria together with 118 HCV-untreated patients constituted the study group. The 328 patients studied had a median age of 44 years (IQR 40–48), and 74% of them were males. The route of acquisition of the HCV-HIV infections was through intravenous drug use in 95% of cases, and the estimated duration of HCV infection (considered as 1 year after starting intravenous drug use) was 24.4 years (20.8–27.5). In 26% there was a past history of alcohol abuse (≥50 g alcohol intake/day during ≥5 years), and 27% of them continued drinking regularly. AIDS had been diagnosed in 24% of patients, 80% had been receiving highly active antiretroviral therapy (HAART) for 8.8 (4.0–11.7) years, 78% had undetectable plasma HIV viral load, and 50% maintained cellular immunity over 500 CD4/mm3 and 72% over 350 CD4/mm3. HCV genotype distribution was 1 (53%), 2 (2.7%), 3 (34.1%), and 4 (10.1%), and 57% of them had HCV viral loads over 800,000 UI/ml. Significant differences were observed between treated and untreated patients regarding age, HCV-genotype distribution, duration of HCV infection, and LSS at baseline (Table 1). However, such differences were not unexpected, as patients with lower stages of fibrosis are more likely to be younger and have a shorter duration of HCV infection, and patients with less fibrosis and/or unfavorable genotypes are more likely not to be treated.
Data are expressed as median (interquartile range) or n (%; determined over available patients for each variable).
Comparisons performed between treated and untreated patients (* p<0.05; ** p<0.01) and between sustained virological response and treatment failure groups (# p<0.05; ## p<0.01) by Mann–Whitney U and χ2 tests.
ART, antiretroviral therapy.
Table 1 also shows the baseline characteristics of the patients according to the final results of anti-HCV therapy. Eighty patients (38.1%) reached an SVR and 130 patients (61.9%) finally failed to respond to anti-HCV therapy (TF group). This TF group had a significantly longer duration of HCV infection, persistence in drug addiction, and a more unfavorable genotype distribution and RNA-HCV.
Baseline estimates of liver fibrosis using transient elastometry were available in 39 and 51 patients of the SVR and treatment failure groups, respectively, and in all untreated patients. The rest of the patients had a Metavir score from a liver biopsy performed 6.5 (0.3–22) months before the baseline time point. A total of 49 and 92 liver biopsies were available in the SVR and TF groups, respectively. Biopsied (n=141) and nonbiopsied patients (n=90) had similar fibrosis stages at baseline. Of the 21 patients who had both biopsy and transient elastometry measurements, there was a concordance in the fibrosis stage in 11 of them, and in seven additional patients there was a discrepancy of only one stage. Elastometry stages were more advanced than biopsy stages in almost all discrepant cases, which is not unexpected considering that biopsies were performed earlier than transient elastometry measurements. At the first assessment, the distribution of the combined LSS showed a higher rate of F4 stage in the TF group than in the SVR and untreated groups.
Effect of HCV treatment on liver fibrosis
Changes in fibrosis by transient elastometry and LFI were assessed at an intermediate point (around 12 weeks of the onset of anti-HCV therapy), and, finally, the last LSS was obtained in all patients at a median of 38 (25–46) months from baseline. The outcome results in treated and untreated groups are shown in Table 2, according to the virological response obtained.
p<0.05; ** p<0.01, as compared with baseline values by Wilcoxon signed ranks or McNemar tests.
Data are presented as median (interquartile range) or n (%; determined over available patients for each variable).
RC, relative change with respect to baseline (%); ND, not done.
In the SVR group, APRI, Fib-4 and Forn indexes experienced a progressive reduction with anti-HCV treatment. The median change for the APRI index from baseline to the end of the study was a fall of −63.5% (−77 to −45), for Fib-4 of −27.0% (−50 to 1.9), and for Forns of −19.7% (−35 to −7.8). Similarly, transient elastometry measurements fell abruptly and the median percentage change of liver stiffness decreased by −29.6% (−45 to −10.5) at the end of anti-HCV therapy, remaining at this level at the end of follow-up. The distribution of LSS in the SVR group was 52 (65%) patients had a mild fibrosis score (≤F2) and 28 (35%) had severe liver fibrosis (≥F3) at baseline, but at the final assessment LSS changed to 69 (86.3%) and 11 (13.7%) patients, respectively [odds ratio (OR) 0.30 (95% CI 0.13–0.69), p=0.003].
However, the TF group experienced a mild and not uniform fall in transient elastometry and in LFI indexes, which were not maintained at the end of follow-up. The median change for the APRI index was −6.9% (−46 to +50), for Fib-4 0.89% (−25 to +65), and for Forns index 4.9% (−9 to +18). The median rate of change for transient elastometry measurements showed a heterogeneous behavior among patients in the TF group with a −5.0% (−23 to +33) change. The LSS in the treatment failure group before and after anti-HCV therapy was as follows: mild liver fibrosis (≤F2): 56 (43.1%) vs. 49 (37.7%) and advanced fibrosis (≥F3): 74 (56.9%) vs. 81 (62.3%); OR 1.25 (0.74–2.12), p=0.44.
The untreated group suffered a median rise of +15.4% (−9.4 to +48) in transient elastometry measurements and a significantly higher rise in LFI indexes with a median percent change of 17% (−24 to +72) for APRI, 21.3% (−7.4 to +60) for Fib-4, and 10.2% (−2.7 to +30) for Forn indexes. Untreated patients allocated in a ≤F2 stage decreased from 97 (82.2%) at baseline to 73 (61.9%) at the end of follow-up; reciprocally, 21 (17.8%) patients with advanced liver fibrosis (≥F3) at baseline increased to 45 (38.1%) at the end of follow-up, respectively [OR 2.85 (1.50–5.43), p<0.001]. Four patients in the SVR, nine in the TF, and no patient in the untreated groups died during follow-up because of complications of decompensated cirrhosis. Three patients in the TF group developed a hepatocellular carcinoma.
Factors associated with changes in liver stiffness measurement
Ninety-one treated or untreated patients (27.7% of the cohort, or 34.6% excluding patients classified F4 unable to worsening) increased LSS at the end of the study with respect to baseline. The distribution of overall changes in fibrosis development among the different groups is shown in Fig. 1, and the stratification by individual baseline LSS in Table 3. The increase in LSS was mainly related to the anti-HCV treatment outcome. Thus, 33.1% of patients in the TF group, 39% of patients in the untreated group, and 2.5% of patients in the SVR group showed a worsening of their liver disease. Worsening outcomes in liver stiffness stages as compared between paired groups were OR (95% CI) 19.3 (4.4–119), p<0.001, for TF vs. SVR; 24.9 (95% CI 5.6–154), p<0.001, for no therapy vs. SVR; and OR 1.29 (95% CI 0.74–2.3), p=0.40, for no therapy vs. TF. However, we observed a decrease in LSS in 53.8% of patients in the SVR group, but only 19.2% and 5.9% in the treatment failure and HCV-untreated groups, respectively. Paired comparisons were OR: 4.88 (95% CI 2.51–9.53), p<0.001, for SVR vs. TF; 18.4 (7.17–49.4), p<0.001, for SVR vs. no therapy; and 3.78 (1.47–10.1), p=0.003 for TF vs. no therapy. Finally, the rate of patients remaining in the same baseline stage was more uniform among the groups: 47.7% for TF, 43.8% for SVR, and 55.1% for the untreated groups, respectively (p nonsignificant).
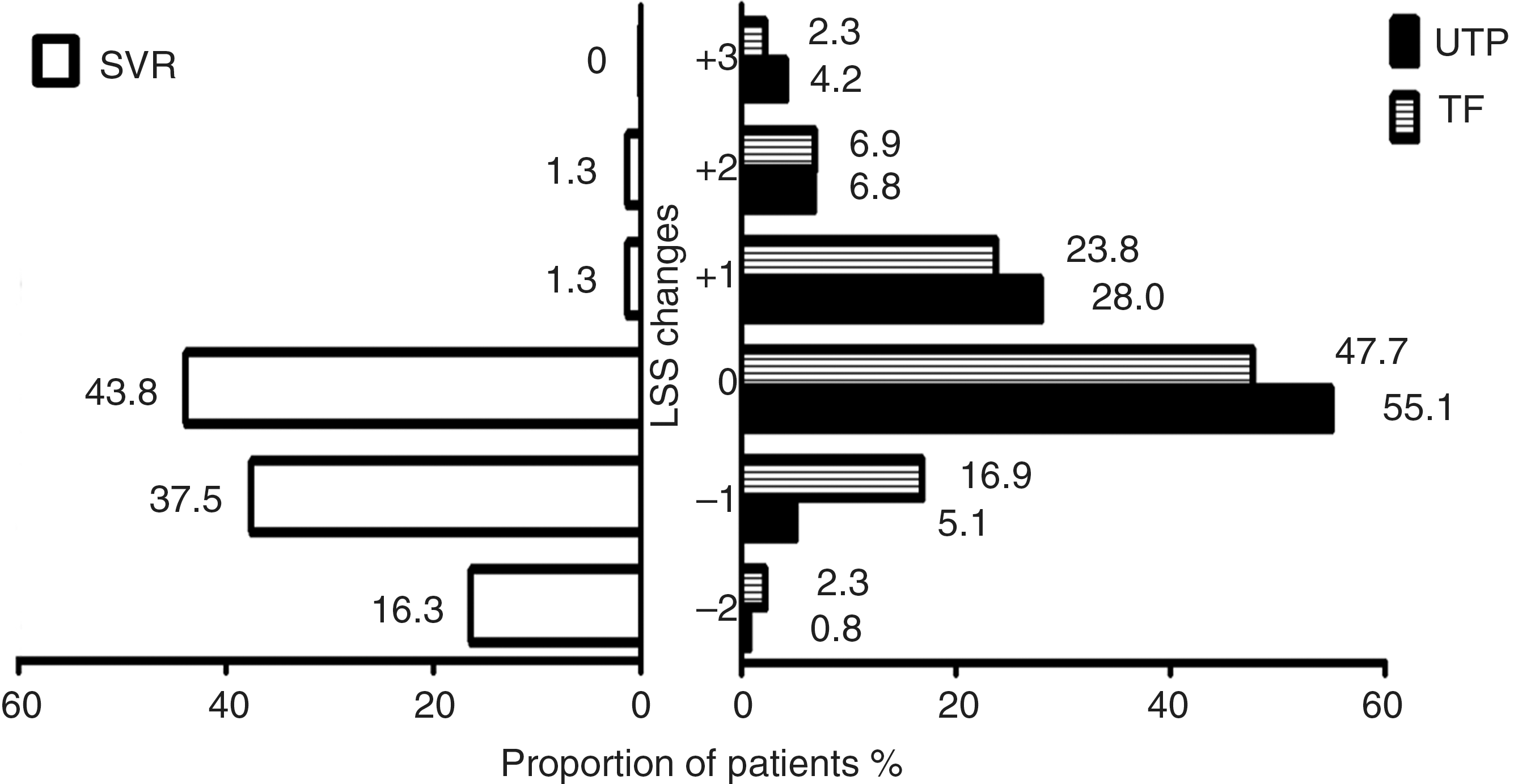
Rate of changes (%) observed in liver stiffness stage (LSS) between baseline and the end of follow-up in patients with sustained virologic response (SVR), treatment failure (TF) and untreated patients (UTP).
Data are n (%). SVR, sustained virological response group; TF, treatment failure group; UTP, untreated patients.
Predictors of worsening in LSS between baseline and end of study were analyzed in 263 patients, after excluding 65 patients with cirrhosis at baseline. Variables significantly associated by univariate analysis with an increase in LSS (Table 4) were alcohol abuse defined as >50 g/day intake for ≥5 years, longer duration of HCV infection, HCV genotypes 1 or 4, RNA-HCV >800,000 UI/ml, poorer immunological status at baseline, absence of anti-HCV therapy, unsuccessful anti-HCV therapy, and longer time interval between baseline and end of follow-up. In multivariate analysis, only alcohol abuse, CD4 count <500 cells/mm3, failure of anti-HCV treatment, and a longer time between therapy and end of follow-up were associated with increased LSS staging.
Patients with F4 stage at baseline were excluded because their fibrosis stage cannot progress.
Patients with F0-F1 stages at baseline were excluded because their fibrosis stage cannot improve.
In 75 patients (22.9% of the cohort, or 36.9% excluding F0-F1 patients unable to improve) LSS decreased during follow-up. When the 125 patients with F0-F1 stage at baseline were excluded from the analysis, factors significantly associated with a decrease in LSS, in the remaining 203 patients, were alcohol abstinence, CD4 count >500 cells/mm3, anti-HCV therapy, and SVR achievement. By multivariate analysis the parameters predictive of decreased LSS were absence of alcohol abuse, baseline CD4 cells count over 500/mm3, and SVR achievement.
Discussion
Using a longitudinal approach with serial transient elastometry and LFI measurements, we were able to confirm the dynamic profile of hepatic fibrogenesis, which was clearly influenced by the response to anti-HCV treatment. Treated patients experienced a median fall in liver stiffness of −22% expressed as rate of change over baseline, while the nontreated patients experienced an increase of 15.4%. The most striking finding was observed in the SVR group, where the baseline liver stiffness decreased −29% after a median follow-up of 38 months, almost similar to that obtained at the end of anti-HCV treatment. The early decrease in liver stiffness suggests an effect of peginterferon-ribavirin on the severity of inflammation and hepatic injury, whereas the late, long-term reduction in liver stiffness suggests regression of fibrosis itself. However, patients with an unsuccessful therapy outcome also showed a significant improvement in elastometry at the end of treatment, but it was not maintained afterward.
Other studies with serial elastometry measurements have generally demonstrated similar results in monoinfected or coinfected patients, with changes from −29.5% to −43.5% and from −24.5% to +17% in SVR and non-SVR patients, respectively. 10 –12 Other studies found elastometry decreases of −3.4 kPa, and −1.8 kPa in patients who achieved or did not achieve SVR. 13
The rate of progression of fibrosis in HCV-infected patients cannot be predicted with certainty, because the studies published have focused on different populations of monoinfected or coinfected subjects, regardless of anti-HCV treatment status, with diverse follow-up periods and using different fibrosis assessment based on paired biopsies, noninvasive methods, or both procedures. Untreated patients better represent spontaneous fibrosis evolution without intervention. In this group we found worsening of fibrosis, defined as a one-stage increase in the LSS, in 44% of patients, excluding those with cirrhosis at baseline, in almost 3 years of follow-up. Based on paired biopsies, spontaneous progression of fibrosis in monoinfected patients ranged from 8% to 12% in 30–44 months 14,15 to 50% to 75% in at least 60 months. 16,17 Considering only coinfected patients, spontaneous histological progression has been described in 35–46% of untreated patients over a 3-year interval. 18,19 Also, a faster fibrosis progression measured by transient elastometry 11 or even no change in liver stiffness in untreated patients over 2 years has been reported. 10
The main objective of our study was to evaluate the changes in LSS according to the response to therapy. Overall, 34.6% of patients without previous cirrhosis had an increase in LSS and 36.9% of patients ≥F2 at baseline improved in at least one LSS. The outcome of anti-HCV-therapy was a determinant of these changes, as 44% and 54% of the SVR patients stopped progression of fibrosis or improved, respectively. However, the TF and untreated groups showed a parallel unfavorable evolution with 33% and 39% of LSS progression, respectively.
Discordant results have been published regarding the impact of anti-HCV treatment on LSS progression in HIV-HCV-coinfected patients. Thus, some studies found a fibrosis progression rate of 38.2% in nonresponders to anti-HCV therapy 19 and another study found 44% of fibrosis progression, but 17% of histological regression in treated patients after a median follow-up of 3.3 years. 18 Other studies reported a worsening in fibrosis in 20% 20 and 17.1% 21 after therapy.
Assessment of fibrosis by transient elastometry has also been reported. Thus, some studies found favorable fibrosis changes even in non-SVR patients, 10,22 increases in advanced fibrosis despite SVR, 23 and reversal of advanced fibrosis/cirrhosis. 10,11 Although the correlation of elastometry with biopsy after anti-HCV treatment is unclear, studies based on pretherapy and posttherapy paired biopsies have also found lesser degrees of fibrosis if SVR was achieved. 18,20,24
We found expected and logical associations of LSS progression in the multivariate analysis with factors such as alcohol consumption, immunological status, and non-SVR. However, LSS regression was associated with the same factors taken in the opposite sense, which reinforces the validity of our observations.
Failure to obtain an SVR was the most commonly reported factor associated with worsening of fibrosis. 5,10 –12,18 –22 Other variables associated with fibrosis progression were older age, 25 alcohol intake, 5,12,25 interval between biopsies or elastometry measurements, 18,22 necroinflammatory histological index, 18 poor HIV control, 18 insulin resistance, and mitochondrial toxicity linked to the use of dideoxynucleosides, 21 among others. Histological or elastometry improvement was almost constantly correlated with the presence of SVR or, at least, with initial HCV clearance despite subsequent relapse. 2,10
Several characteristics of the study may limit our findings and their generalization to other settings. At the time of starting therapy, fibrosis was assessed by two different methods, biopsy prior to 2007 and elastometry afterward, and only by elastometry during follow-up. Furthermore, to homogenize measures in a semiquantitative scale of LSS, it was necessary to establish cut-off points. Although elastometry is a well-validated method for the detection of cirrhosis, there is no general agreement on the optimal cut-off values for intermediate stages of fibrosis. 3 –6 However, such a mixed approach has been reported previously, 26 and, in addition, biopsied and nonbiopsied patients had similar stages of fibrosis at baseline, suggesting that there was no significant bias by the combination of these two methods of fibrosis evaluation. Moreover, we also used LFI, measured in parallel, to increase the diagnostic accuracy. Another point of concern is the initial imbalance in some characteristics between treated and untreated patients, extracted from the same cohort, mainly as a result of selective indications for anti-HCV treatment. 1
In summary, we found progression of fibrosis in about one-third and improvement in fibrosis in another one-third of treated patients during a follow-up period of nearly 3 years. The main factor responsible for these changes was the type of response to anti-HCV therapy, although other factors such as alcohol consumption and immunological status were also involved. Transient elastometry and simple LFI, running in parallel, might allow monitoring of fibrosis without requiring a liver biopsy.
Footnotes
Acknowledgment
These results were presented in part at the 51rd Intersciences Conference on Antimicrobial Agents and Chemotherapy (ICAAC), Chicago, IL, 17–20 September 2011.
Author Disclosure Statement
No competing financial interests exist.