
Abstract
Human immunodeficiency virus
Introduction
E
Based upon the recent reports published by the Iranian Ministry of Health in its official web site (
Materials and Methods
This study was performed at the laboratory of the Parasitology and Mycology Department of Shiraz University of Medical Sciences, from May 2010 to May 2011. The study's protocol was approved by the Ethics Committee of the university. HIV-infected children and adult patients suffering persistent and/or recurrent diarrhea were included in this study. A total of 356 consecutive patients were enrolled in the study. Of these, 103 patients presented with persistent/chronic diarrhea and 253 did not have diarrhea (asymptomatic interval).
Demographic and clinical data were collected using a structured questionnaire. A fecal sample was collected from each patient and was concentrated by the physiological saline solution ethyl acetate technique for the detection of parasitic ova, cysts, and larvae. Direct smear was also used for detecting trophozoites and cysts. Staining by a modified acid fast trichrome was performed for the determination of coccidian oocysts and microsporidia spores. 16 Polymerase chain reaction (PCR) was done using specific PCR primers based on the region coding for the small subunit ribosomal RNA (SSU rRNA) for diagnostic confirmation of Cryptosporidium spp., I. belli, C. cayetanensis, and E. bieneusi on all the stool samples. 17 –19 Because the internal transcribed spacer (ITS) region of the rRNA has a high degree of diversity among the isolates, it has been useful in many studies for the detection and identification of E. bieneusi genotypes. 20 Therefore, DNA extraction was done for all the samples as previously described. 21
Further genomic analyses were carried out for amplifications of all fecal samples followed by sequencing. Extracted DNA from fecal specimens was subjected to PCR using primers (designed to ITS2) from those described elsewhere in the I. belli ribosomal gene cluster (GenBank accession no. DQ060680) as follows: forward primer, 5′-CCGAACGTCATCCGAAATAG-3′ and reverse primer, 5′-ACTAGGAGCTGACGATACAC-3′. The presence of a 175-base pair amplicon was considered to indicate I. belli infection. 18 A two-step nested PCR protocol was used to amplify the SSU rRNA gene using primers, which amplified sequences unique to all species of the Cryptosporidium genus. A PCR product of 1,300 bp was amplified using forward (5′-′TTCTAGAGCTAATACATGCG-3′) and reverse (5′-CCATTTCCTTCGAAACAGGA-3′) primers. For the secondary nested PCR step, a PCR product that was 836–849 bp long (depending on the species) was amplified using primers (5′-GGAAGGGTTGTATTTATTAGATAAAG-3′ and 5′-CTCATAAGGTGCTGAAGGAGTA-3′). 17 A two-step nested PCR was used to amplify the ITS region as well as a portion of the flanking large and small subunit ribosomal RNA genes (400 bp) for the detection of E. bieneusi. The outer primers were EBITS3 (5′-GGTCATAGGGATGAAGAG-3′) and EBITS4 (5′-TTCGAGTTCTTTCGCGCTC-3′) and the inner primers were EBITS1 (5′-GCTCTGAATATCTATGGCT-3′) and EBITS2.4 (5′-ATCGCCGACGGATCCAAGTG-3′). Finally, these reactions produced a fragment of 390 bp. 17 Nested PCR for the detection of Cyclospora and Eimeria species was performed using the primer pairs F1E/R2B (5′-TACCCAATGAAAACAGTTT-3′/5′-CAGGAGAAGCCAAGGTAGG-3′) and F3E-R4B (5′-CCTTCCGCGCTTCGCTGCGT-3′/5′-CGTCTTCAAACCCCCTACTG-3′) to generate an amplified fragment of 292 bp. 19
All PCR-positive samples were directly sequenced with the inner set of primers used for the secondary PCR. For this purpose, PCR products of the positive samples were then treated with a QIAquick Gel Extraction kit (QIAGEN Gmbdh, D-40724 Hilden, Germany) and sent to the Kowsar Tech Exploration Company (Iran) for sequencing. Sequence chromatograms from each strand were edited and aligned using Gene Runner software (version 3.05). The sequences were compared with sequences in the GenBank database by BLAST analysis. Data were analyzed using SPSS (version 12).
Results
Of the 356 patients with an age range of 10–69 years, 273 (76.68%) were males and 83 (23.31%) females. The mean age of the male and female patients was 38.68 and 35.69 years, respectively. The study population consisted of 51 patients with CD4 count >500 cells/μl, 117 patients with CD4 count 200–500 cells/μl, and 188 patients with CD4 count <200 cells/μl. Among the 188 patients with a CD4 count <200 cells/μl, 53 patients were infected with intestinal parasites and opportunistic parasites were detected in 34 cases. Cryptosporidium (23 patients) was the most common opportunistic pathogen followed by E. bieneusi (eight patients), I. belli (two patients), and C. cayetanensis (one patient) in this group (Table 1) (Figs. 1 –5). Of the 117 patients with CD4 count 200–500 cells/μl, pathogenic parasites were identified in 26 patients and opportunistic parasites in eight patients. Pathogenic parasites were detected in only 14 patients with CD4 count >500 cells/μl (Table 1). E. histolytica/E. dispar were found in seven patients (two samples from patients with CD4 count <200 cells/μl, three samples from patients with CD4 count 200–500 cells/μl, and two samples from patients with CD4 count >500 cells/μl) (Table 1).
Confirmed as C. parvum and C. andersoni by PCR sequencing using specific primers of the SSU-rRNA gene.
Confirmed as Enterocytozoon bieneusi (genotypes D and K) by PCR sequencing using primers of the ITS region of the rRNA gene.
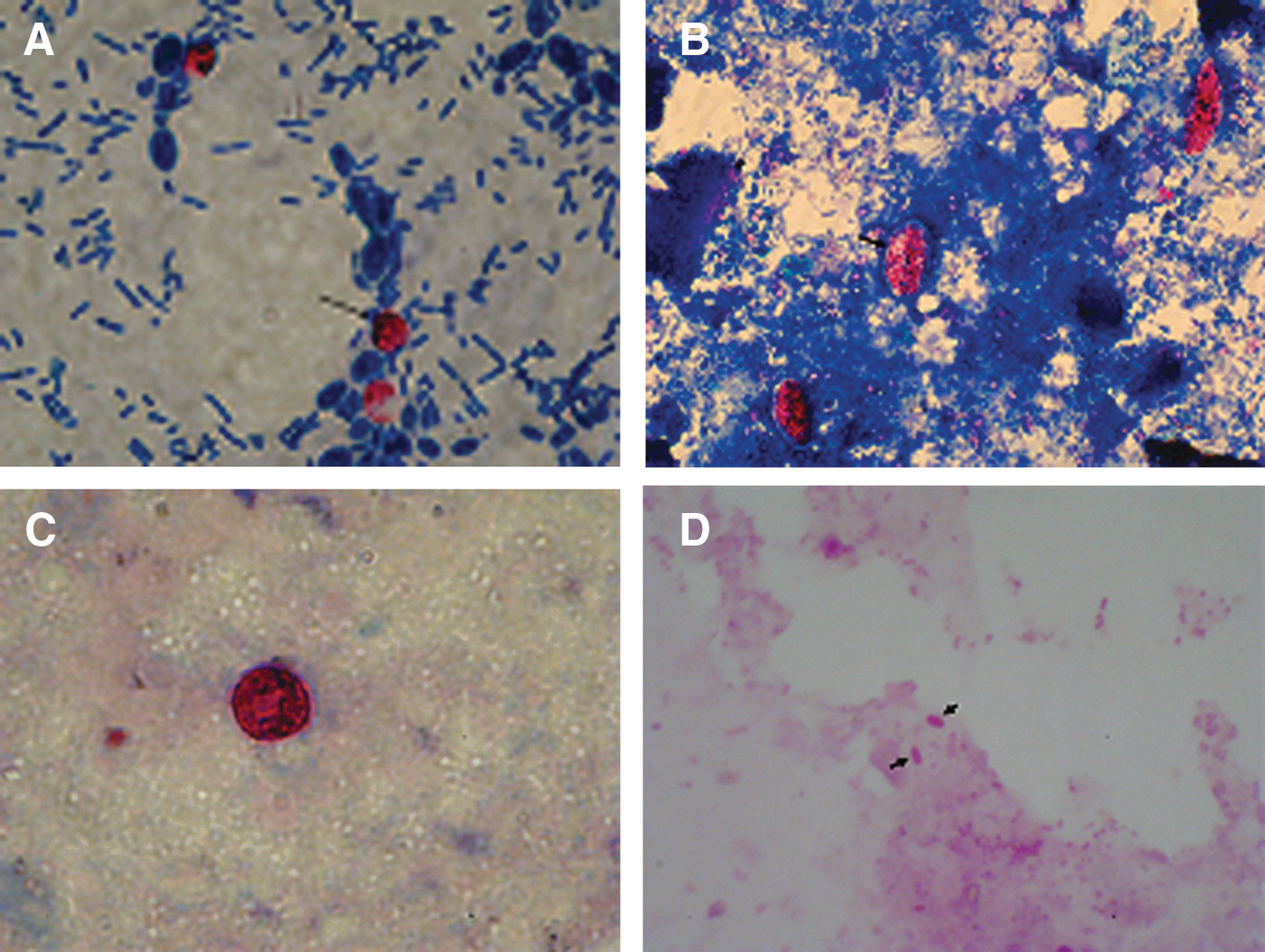
Photomicrographs of fecal smears.
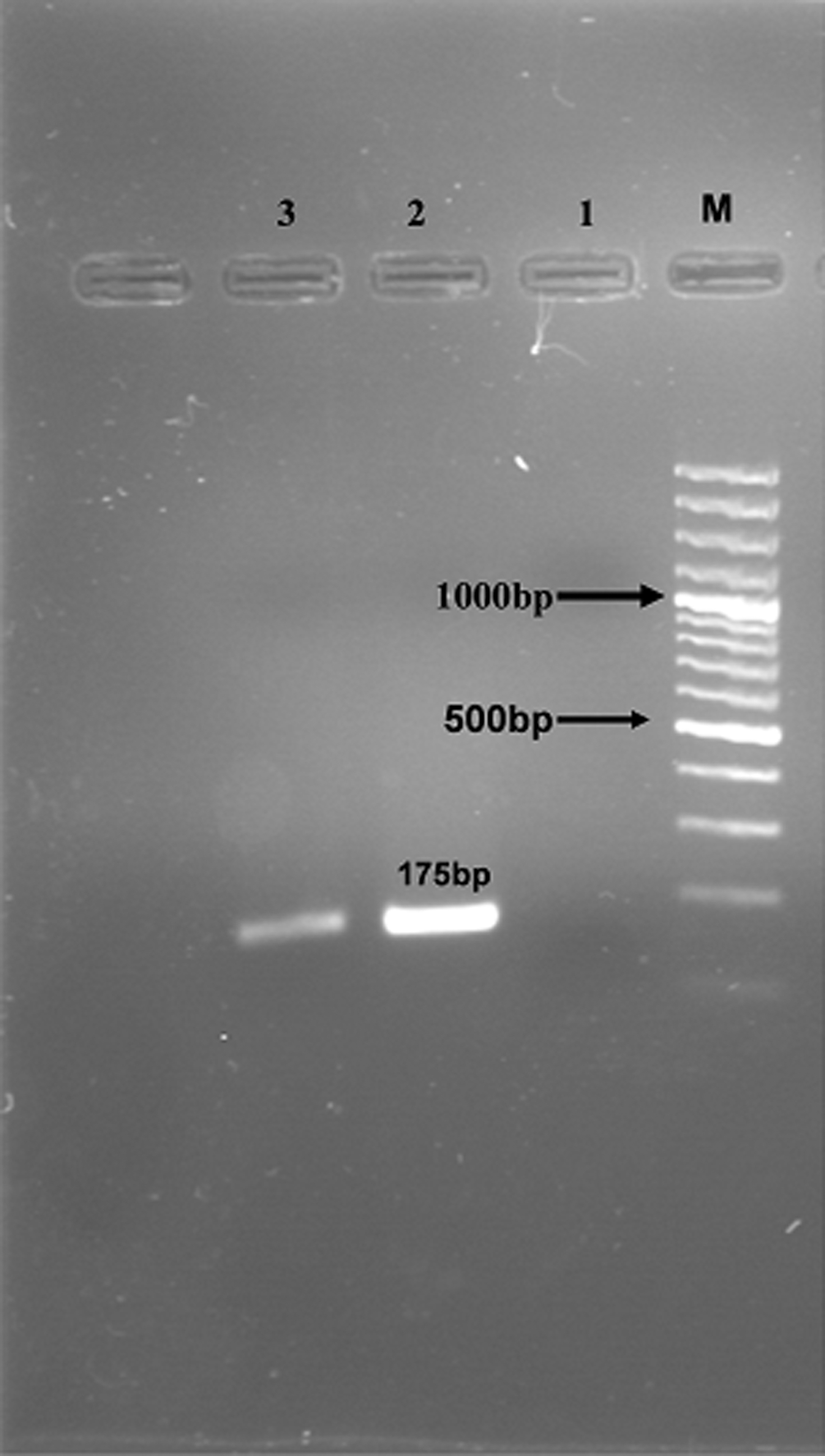
PCR products of Isospora belli on electrophoresis on 1.5% agarose gel. Lane M: 100 bp DNA size marker. Lanes 1–2: negative and positive control, respectively. Lane 3: positive sample.

Detection of Cryptosporidium-specific fragments by nested PCR. Lanes: M, molecular marker; 1–3, positive samples; 4–5, negative and positive control samples, respectively. The molecular weight marker was a 100-bp ladder.
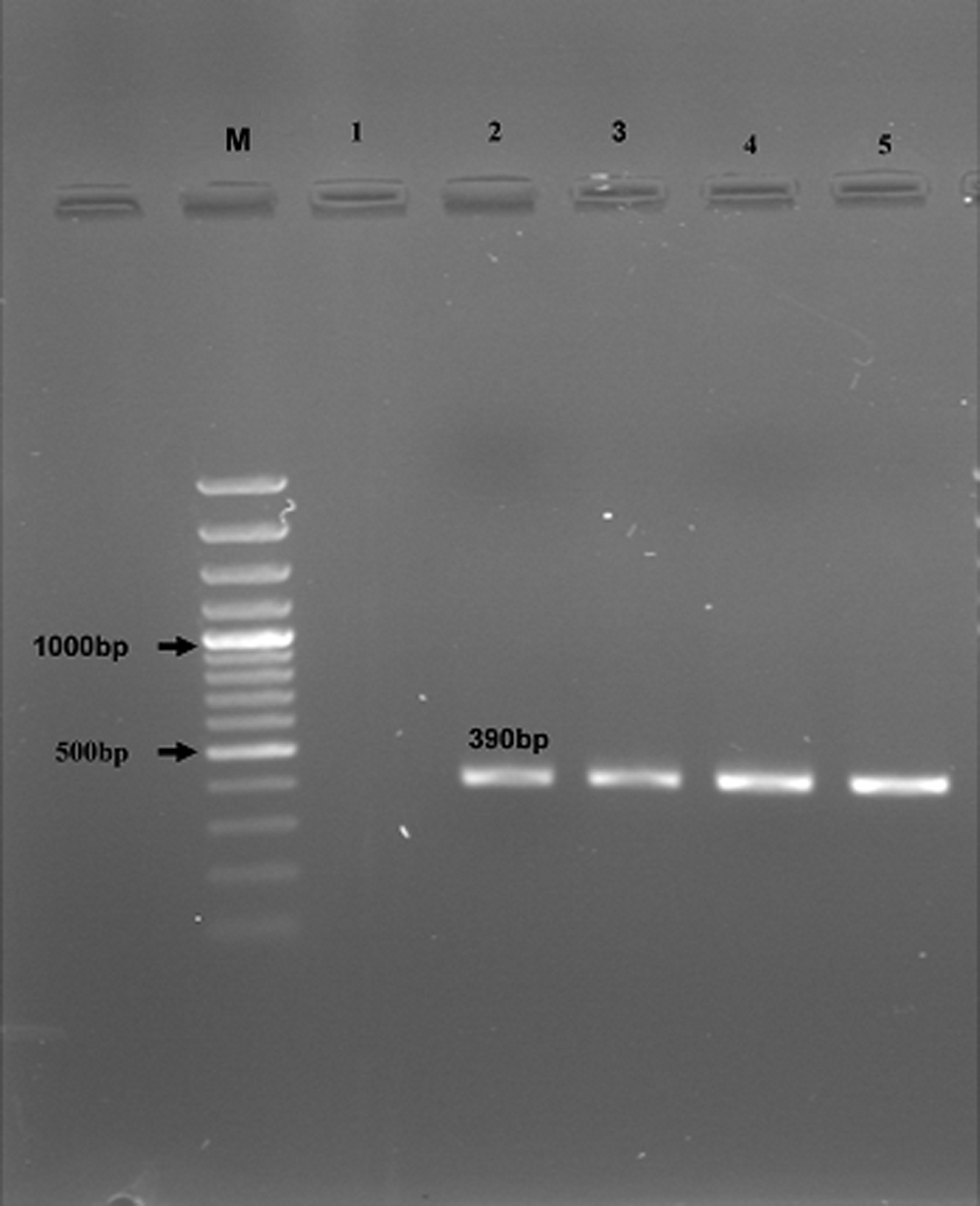
Nested PCR-amplified products of Enterocytozoon bieneusi from stool samples (M: 100-bp MW; lanes 1 and 2: negative and positive control, respectively; lanes 3–5: positive samples).
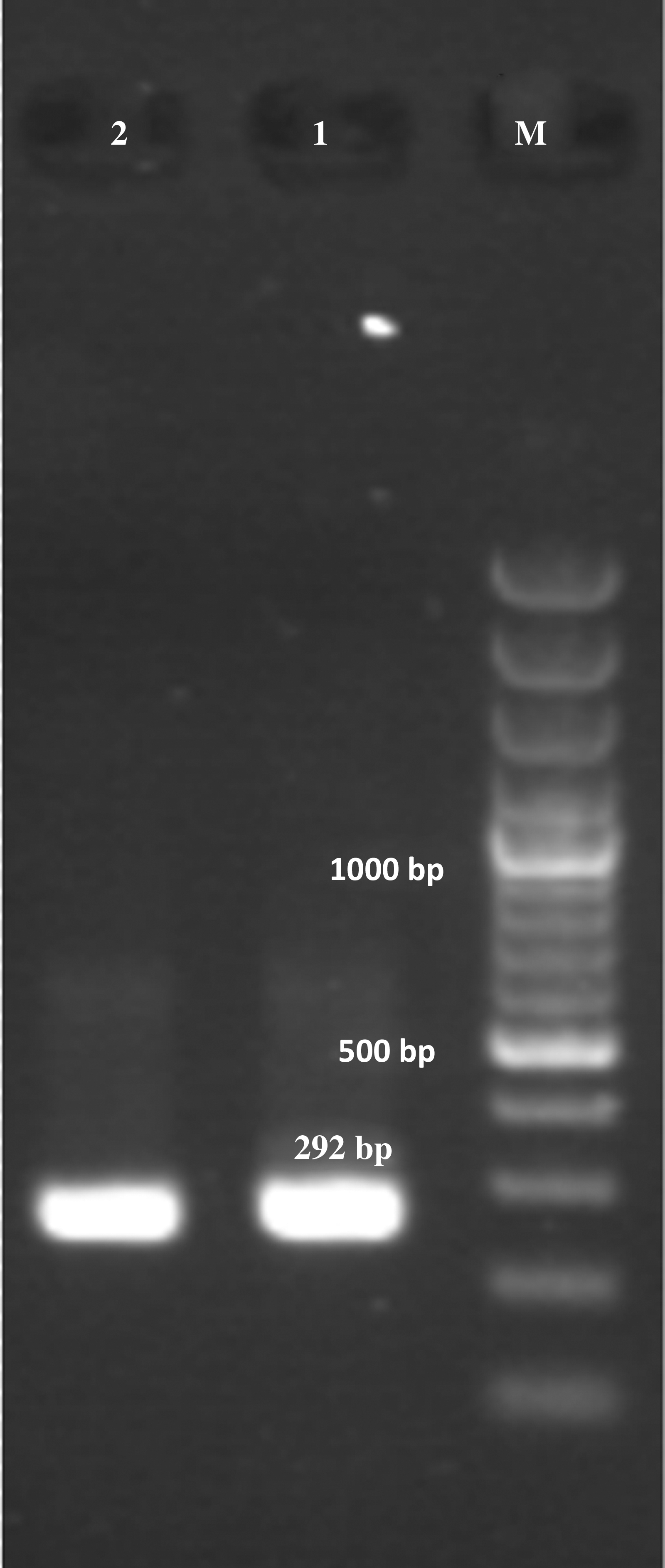
Nested PCR amplification of Cyclospora cayetanensis DNA. Lane M: molecular size markers; lanes 1 and 2: positive control and study specimen.
In microscopy-positive stool samples, E. bieneusi spores were found to be oval measuring 1–1.5 μm in size (Fig. 1). PCR amplification of E. bieneusi DNA was done in all samples of 356 patients by nested PCR using the species-specific primers (Fig. 4). Of the 356 HIV-positive patients evaluated in this study, eight with persistent chronic diarrhea were found to be positive for E. bieneusi using microscopic examination and the nested PCR technique. E. bieneusi (genotypes D and K) were detected in all eight positive cases without coinfection with other enteric parasites. No microscopic detection or PCR amplification was found from HIV-positive patients with asymptomatic intervals who were negative for E. bieneusi (n=253). It must be emphasized that infections with intestinal nonpathogenic parasites are not shown here. The dominant species of Cryptosporidium was C. parvum (33 out of 34 patients), and only one patient was infected with C. andersoni. G. lamblia (23 patients) and B. hominis (14 patients) were the more prevalent nonopportunistic pathogens in our study (Table 1). Genotyping of E. bieneusi from patients with diarrhea by sequence analysis of the ITS region showed genotypes D and K. The great proportion of opportunistic pathogens in patients with CD4 count <200 cells/μl was significantly higher than that in the other two groups of patients with CD4 count >200 cells/μl (p<0.05).
In this particular group, the most common opportunistic and nonopportunistic pathogens were Cryptosporidium spp., E. bieneusi, G. lamblia, Sarcocystis spp., and B. homonis, observed in 34, 8, 23, 1, and 14 patients, respectively. The few helminthes, E. vermicularis and H. nana, were observed in three patients and one patient, respectively (Table 1). Overall, out of 356 HIV-infected patients, enteric pathogenic parasites were detected in 93 (26.12%) stool samples, of which 45 patients had opportunistic and 48 had nonopportunistic pathogenic parasites.
Discussion
Numerous opportunistic infections occur in HIV-infected patients, because of the down-regulation of the immune system. 22 Gastrointestinal opportunistic parasitic infections are a universally recognized problem in such patients. These infections mostly present with diarrhea, leading to life-threatening complications. 11,23 Unfortunately, the diarrhea caused by these parasites cannot be differentiated from that caused by other enteric infectious agents such as G. lamblia, noninvasive bacterial infections (e.g., enterotoxigenic Escherichia coli), and viral infections (e.g., Norwalk and Rotavirus). 1,4 Diarrhea is a significant problem in immunocompromised patients worldwide, especially patients with HIV/AIDS with CD4 counts <200 cells. 24
Previous studies have demonstrated that C. parvum is frequently associated with diarrhea in patients with AIDS with CD4 counts <200 cells in developed countries where the prevalence of infection ranges from 17% to 62%. 25–26 In our study, we used the genus/species-specific PCR primers for the detection of the enteric coccidia and E. bieneusi in stool samples (Figs. 2 –5). The DNA extraction method in combination with a modified physiological saline solution ethyl acetate sedimentation procedure may result in increasing sensitivity, raising the number of oocysts and spores. False-positive results and cross-amplification were not observed. An increase in oocysts and spore concentration by sedimentation method has also been reported in another study.
The interpretation of genotyping results with sufficient concern is highly recommended and is the basis for the detection of the sources of infection. For example, in two studies in India, the Cryptosporidium mouse genotype was identified in a child and an HIV-positive adult based on the results of RFLP analysis of the SSU rRNA PCR products. 27–28 The true identity of the parasite was probably C. meleagridis, which has the same RFLP pattern as the mouse genotype in the genotyping technique used. The detection of C. andersoni in a Malawian child was also largely based on RFLP analysis, 29 which needs to be confirmed by DNA sequencing because DraI and AseI RFLP is mainly used in species differentiation and C. muris may also share the same pattern. Although the microscopic examination of feces still remains the mainstay of laboratory diagnosis of cryptosporidiosis, the results indicate that PCR is more effective than microscopic examination for the detection of coccidiosis.
To determine if there was a correlation between the prevalence of coccidian and microsporidia parasites and CD4 counts, we calculated the mean CD4+ T cell counts in these patients and we found that CD4 counts <200 cells, especially CD4 counts less than 100 cells, were significantly associated with the presence of opportunistic parasites and diarrhea. In the present study, microscopic stool examination and PCR techniques showed that 45 (12.64%) patients were infected with enteric opportunistic parasites. Among the opportunistic parasites, C. parvum is the predominant pathogen in some countries, similar to what was found in our study. 5 The prevalence of opportunistic parasites in patients with CD4 counts <200 cells/μl was 18.08% (34/188 patients). In our study, C. parvum infection was detected in 34/356 (9.55%) patients using microscopic examination and a molecular method.
The use of parasitological combination with molecular methods in our study suggests that the prevalence of Cryptosporidium spp. infections in HIV-infected patients may be significantly greater than reported previously. DNA sequencing analysis of SSU rRNA of Cryptosporidium spp. showed that except for one case, all isolates were C. parvum. The occurrence of zoonotic genotypes of Cryptosporidium in all of the cases in the present study indicates that zoonotic transmission is of considerable significance in the epidemiology of cryptosporidiosis in the studied region. The presence of cryptosporidial infections in patients with HIV/AIDS in our study is probably related to an increased risk of acquiring infection from contact with infected animals and prolonged excretion, which in turn increases the risk of subsequent transmission. In these patients, the risk of acquiring cryptosporidiosis is associated with the degree of immune suppression as measured by CD4 cell counts. Other risk factors for cryptosporidiosis in our patients with HIV/AIDS include gender, age, personal health, occupation, and level of education.
Studies from Nairobi and London demonstrate that cryptosporidiosis is a common opportunistic enteric protozoan disease encountered in HIV/AIDS-infected individuals. 2,30,31 This is supported by a recent prospective, comparative study comparing the prevalence of enteric protozoa among HIV-positive and HIV-negative men in Australia. 2,32 A total of 1,868 inpatients submitted stool specimens over a 36-month period to determine the presence of enteric parasites. 2 In this study C. parvum cases occurred exclusively in HIV-positive patients. In our survey I. belli, C. cayetanensis, and E. bieneusi were detected in two, one, and eight patients, respectively. I. belli is found worldwide, but occurs predominantly in tropical and subtropical climates and is endemic in South America, Africa, and Southern Asia, and immunodeficiency was shown to increase the susceptibility to infection with I. belli. 33 –35 Since the use of trimethoprim-sulfamethoxazole to prevent Pneumocystis jirovecii in developed countries, there has been a marked reduction in the occurrence and clinical course of isosporiasis.
The lower prevalence of isosporiasis in developed countries and Iran and especially in this area may be ascribed to the secondary prophylaxis for pneumocystosis through the administration of sulfamethoxazole-trimethoprim during the course of AIDS, since I. belli and C. cayetanensis are sensitive to this treatment. In contrast, in developing countries, I. belli infections are frequently accompanied by chronic diarrhea in patients with HIV/AIDS, occurring in 5–26% of these individuals. 33–34 Also, since the introduction of highly active antiretroviral therapy (HAART), there has been evidence of improvement in chronic diarrhea caused by enteric coccidian. 36 Although these changes have been attributed to the restoration of cell-mediated immunity, it has been suggested that some antiretroviral compounds used in HAART may have a direct inhibitory effect on Cryptosporidium and I. belli. 37 E. bieneusi is the most common microsporidian causing diarrhea in humans and the second most prevalent in immunocompromised patients, especially those with HIV/AIDS, after Cryptosporidium. 2,38
In countries with access to HAART, the prevalence of microsporidial infections has declined. In a study from Australia, the total incidence of intestinal microsporidiosis in HIV-infected patients decreased from 11% in 1995 to 0% in 2004. 39 In contrast, in developing countries because of limited access to HAART, the incidence of coccidiosis and microsporidiosis still remains high. Therefore, because of the use of HAART in most of our patients with HIV/AIDS, a low prevalence of microsporidiosis, isosporiasis, and cyclosporiasis was seen. To the best of our knowledge, this study is the first report of genotypes of E. bieneusi using sequencing from our country. A few studies from Iran have reported a prevalence ranging from 1.5% to 9.4% of enteric coccidiosis in patients with HIV/AIDS. 13,15 Both C. parvum and C. hominis have been reported from HIV-positive adult patients using genetic tools. 40 Thus, the dramatic decline of enteric microsporidiosis, isosporiasis, and cyclosporiasis in our study confirms the importance of effective HAART in preventing advanced immunodeficiency, opportunistic parasitic infections, and associated AIDS-related deaths.
A few studies from other regions of Iran have reported a prevalence of enteric parasites in patients with HIV/AIDS ranging from 17.2% to 18.4%. 13 –15 In our study, nonopportunistic parasites such as G. lamblia and B. hominis were detected in 10.39% (23 and 14 patients, respectively) of all HIV-positive patients across different CD4 groups, which emphasizes the need for early detection and treatment of such infections among HIV-infected patients to reduce the morbidity. The results of our study highlight the importance of the evaluation of intestinal parasitic infections, especially enteric coccidian and microsporidia, in HIV-infected individuals with diarrhea for intestinal parasitic infections, which may help to improve the management of these patients. The etiology of diarrhea could not be determined in most patients, suggesting a need for comprehensive etiological studies covering bacterial, fungal, viral, and parasitic causes of diarrhea among HIV-infected patients in Iran. Also, the importance of tropical and subtropical endemic nonopportunistic intestinal parasitic infections among HIV-infected patients should not be neglected. Therefore, our study emphasizes the need for routine screening of enteric coccidiosis as well as education about practicing personal hygiene and taking timely and appropriate measures.
In conclusion, understanding the species and genotypes of intestinal coccidia and microsporidia can also be useful in establishing the identity of the parasites infecting humans, assessment of the public health significance of these pathogens from animals and the environment, and tracking of infection and contamination sources. All these will promote understanding of the transmission and epidemiology of human coccidiosis and the development of preventive measures to minimize exposures to infections. It could finally lead to strengthening the assessment of accurate risk in high-risk groups.
Footnotes
Acknowledgments
This article is based in part on the Ph.D. thesis of Mahmoud Agholi, which was financially supported by the office of the Vice-Chancellor for Research of Shiraz University of Medical Sciences (Grant 4859). The authors would also like to acknowledge the office of the Vice-Chancellor of Health for its kind support.
Author Disclosure Statement
No competing financial interests exist.