
Abstract
Laboratory assays for the detection of recent HIV infection for HIV incidence surveillance are essential to HIV prevention efforts worldwide because they can identify populations with a high incidence and allow targeting of resources and monitoring of incidence trends over time. This study describes the development of a novel rapid HIV-1 incidence-prevalence (I-P) test that can be used for the simultaneous detection and discrimination of prevalent (long-term) or incident (recent) HIV infections using a single device. A lateral flow assay was developed that uses a multisubtype recombinant gp41 protein applied at two concentrations of antigen (high and low). Prevalent and incident HIV-1 infections can be distinguished based on differential antibody binding at the two antigen concentrations. High level/high avidity antibodies present in prevalent infections bind to and are detected at both antigen concentrations while low level/low avidity antibodies present in recent HIV infections are detected only at the higher antigen concentration line. A total of 205 HIV-positive specimens with known status (recent=105, long-term=100), including 57 specimens from seroconversion panels, were tested by the rapid I-P assay and the results were compared to the HIV-1 BED capture enzyme immunoassay (CEIA). There was a 95.1% agreement of final classification (recent or long-term) with the BED assay (kappa=0.910) (mean recency period=162 days) and a high correlation between the intensity score of the low antigen line with the BED OD-n (Pearson correlation=0.89). The new rapid I-P test has great potential to simplify HIV surveillance efforts by simultaneously providing information on both HIV prevalence and incidence using a single, rapid test device.
Introduction
L
Recent efforts to improve HIV incidence estimates have focused on antibody avidity assays that measure the changing functional properties associated with antibody maturation. 11,12 These approaches typically employ modified commercial assays based on clade B antigens raising the possibility that their performance with diverse subtypes may also be inconsistent. Two new avidity assays were recently described that use a multisubtype gp41 recombinant protein (rIDR-M) to identify recent HIV-1 infection. 13 These assays include a two-well avidity assay method and a novel single-well limiting antigen avidity (LAg-avidity) assay, both of which are formatted as 96-well microplate enzyme immunoassays (EIAs). The single-well avidity assay demonstrated that specimens with low and high avidity antibodies can be distinguished simply by limiting the amount of antigen available to bind the antibodies. This approach has considerable potential due to its simplicity and the use of the multisubtype recombinant antigen. Further characterization of LAg-avidity EIA recently demonstrated that the assay exhibited similar mean duration of recency in four different subtypes with very low rates of misclassification among individuals with long-term infections. 14 Commercially available rapid HIV tests have also been modified to detect recent HIV-1 seroconversion. 15,16 These assays were based on antibody titers and included predilution of the sample to effectively distinguish between recently infected and long-term infected individuals. However, as with the modified commercial EIA, the use of subtype B-derived antigens may limit their applicability in areas where non-B subtype viruses predominate.
In this study, the concept of a limiting-antigen-based avidity measurement was extended from the enzyme immunoassay format to a rapid, lateral flow test device that incorporates the use of the multisubtype gp41 recombinant antigen. This protein was incorporated into the test at two distinct antigen concentrations. This design was shown to have the potential to differentiate recent and long-term HIV infection using a single device in a cross-sectional specimen set. Such a test, once validated, could simplify HIV surveillance in global settings, irrespective of the prevailing subtype, and could provide information about HIV prevalence and incidence in a cost-effective manner in resource-limited settings.
Materials and Methods
Specimens
Sera of known HIV status were obtained from commercial and in-house sources and were used to optimize the antigen concentrations and to establish the performance traits of the rapid incidence-prevalence (I-P) assay (Table 1). Five specimens (two recent and three long-term; Panel 1) were obtained from SeraCare, Inc., Milford, MA (formerly Boston Biomedica, Inc.).These samples were characterized as recent (<180 days) or long-term (in this case >1 year) based on the last known date of seronegative results, as indicated by the manufacturer. Panel 1 has been extensively used for training, for the preparation of QC materials, for proficiency testing programs, and for the development of new concepts for incidence assays. 13
Total panel size=141 including 111 seroconversion panel samples +30 low-titer panel specimens; 44 seroconversion panel members were nonreactive by standard serological methods. Two specimens in the low-titer panels were seronegative.
LT, long-term infection.
Assay optimization was done using specimens obtained from SeraCare, Inc. (Panel 2, n=22; 10 recent, 12 long-term) and from Calypte Biomedical Corp (Panel 3, n=40) (Beaverton, OR). The SeraCare specimens were characterized using the commercial BED capture assay. The Calypte specimens were obtained from HIV antibody-positive individuals who were documented to have been seronegative 2–6 months prior to collection (recent, n=19) and from those who were known to have been HIV antibody-positive for 1 year or longer (long-term, n=21).
Fifteen seroconversion panels (Panels PRB—903, 904, 910, 911, 912, 916, 926, 928, 931, 940, 944, 945, 952, 957, 965; total n=111) and two low-titer panels (PRB 102, n=15; PRB 104, n=15) representing early HIV infection (Panel 4, n=141) were obtained from SeraCare. Serological HIV testing results for these specimens were provided in the manufacturer's product insert for each panel (
Cross-sectional HIV-1 antibody-positive specimens were collected in Cameroon (n=73) (IRB 1367) and by the HIV Laboratory Branch at CDC (n=15) (IRB 1896) (Panel 5, n=88). CDC reference serological testing for all specimens was performed using enzyme immunoassay screening (HIV-1 + 2 + O, Bio-Rad Laboratories, Hercules, CA) with repeatedly reactive specimens tested and confirmed as HIV-1 antibody-positive by HIV-1 western blot (Bio-Rad, Hercules, CA). These samples were subtyped using the p17 and gp41 gene regions as previously described 17 and were found to contain the following clades or recombinant forms: CRF02-A, n=40; A, n=14; CRF11-G, n=4; CRF11-A, n=4; G, n=3; F2, n=2, and one each of D, F, A2, O, and CRF06-G (one specimen was not subtyped). Clade-specific information for the CDC HIV Laboratory Branch specimens was not determined but these were likely US subtype B. These cross-sectional specimens were used to assess the performance of the rapid I-P assay. The rapid I-P results were compared to the BED classification in the cross-sectional specimen set. The BED assay was performed according to the product insert. Specificity of the rapid I-P test was assessed using HIV-1 nonreactive specimens (n=100) from routine screening in the CDC HIV Laboratory Branch (IRB 1896). A flow chart of the optimization and characterization experiments including the panels used is depicted in Fig. 1.
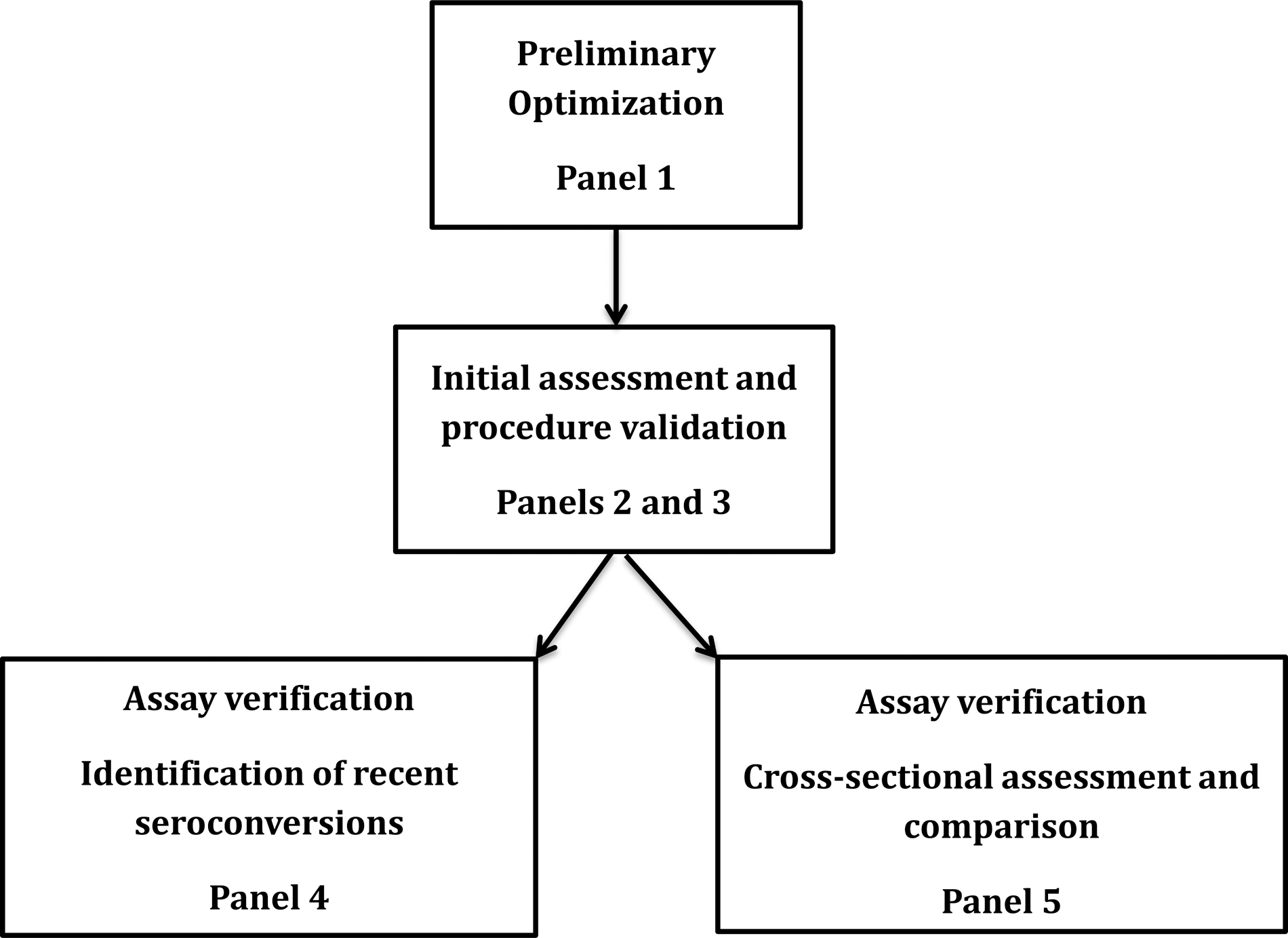
Flow diagram for the development, optimization, and evaluation of the rapid incidence-prevalence (I-P) test.
Colloidal gold conjugate preparation
The preparation of the colloidal gold (hydrogen tetrachloroaurate, Alfa Aesar, Ward Hill, MA) was done using standard preparative techniques. 18 –21 Protein A (1.8 mg) was adsorbed onto the gold nanoparticles (300 ml) for 30 min with stirring at ambient temperature. Any remaining protein-binding sites were blocked by the addition of 30 ml of a 1% bovine serum albumen (BSA) (Sigma-Aldrich, St. Louis, MO) solution to the mixture for 5 min. The colloid conjugate was centrifuged at 3600×g for 50 min, and the pellet was resuspended in a 0.1 M glycine buffer (Bio-Rad Laboratories, Hercules, CA), pH 7.0, containing 6.7% sucrose (Sigma/Aldrich) and 3.3% BSA. The conjugate was diluted to an absorbance of 10 at 530 nm using the same buffer. To prepare the conjugate pads for test assembly, Accuflow P strips (Millipore Corp., Medford, MA) were dipped into the Protein A conjugate solution for 3 min; the excess solution was drained from the pads, which were then placed onto a solid nonabsorptive surface and air dried overnight at ambient temperature. The completed conjugate pads were stored at ambient temperature in a desiccator until use (relative humidity <25%).
Preparation of the immunoassay lateral flow tests
The development of this immunoassay required the characterization of unique assay components along with the selection and optimization of materials and buffers and of individual reagents including the selection of the nitrocellulose membrane, the selection of the sample, conjugate and wicking pad materials, assay blocking agents, concentrations of the rIDR-M antigen for the diagnostic and incidence detection, and optimal dilution of the sample. The lateral flow test strips were prepared using standard techniques. 22 The development and purification of rIDR-M have also been previously described. 13 The rapid I-P assay was configured with two rIDR-M lines at different antigen concentrations (high and low) and a Protein A control line (Fig. 2A). For the optimized device, the rIDR-M protein was reconstituted in 10 mM sodium citrate buffer (pH 3.0) to a concentration of 2.0 mg/ml (high concentration) and 0.15 mg/ml (low concentration). Protein A (Zymed Laboratories, South San Francisco, CA) was reconstituted at 1 mg/ml using 0.1 M sodium carbonate/bicarbonate buffer (pH 9.6) (Sigma/Aldrich, Inc., St. Louis, MO) to serve as an assay control for the Protein A colloidal gold conjugate and as a reference band for scoring assay intensity. For the membrane preparation, Protein A, the high rIDR-M solution (2.0 mg/ml) and the lower rIDR-M solutions (0.150 mg/ml) were simultaneously dispensed onto 350-mm×25-mm nitrocellulose strips (Hi Flow plus HF18004, Millipore Corporation) lengthwise using an Isoflow Dispenser (Imagene Technology, Hanover, NH) in the configuration shown in Fig. 2A with 5 mm spacing. The striped membrane was dried overnight at 32°C in a vacuum oven, was blocked for 10 min with a 10 mM phosphate buffer (pH 7.2) containing 0.08% BSA, and dried as before. The sample application pad (Accuflow P, Millipore Corp) was blocked with 0.10 M sodium phosphate buffer (pH 7.2) containing 40% chicken sera (Animal Technologies, Inc., Tyler, TX) and 0.25% of Pluronic F98 Prill surfactant (BASF, Mt. Olive, NJ). All prepared materials were air dried and stored at ambient temperature in a desiccator until use (relative humidity <25%).
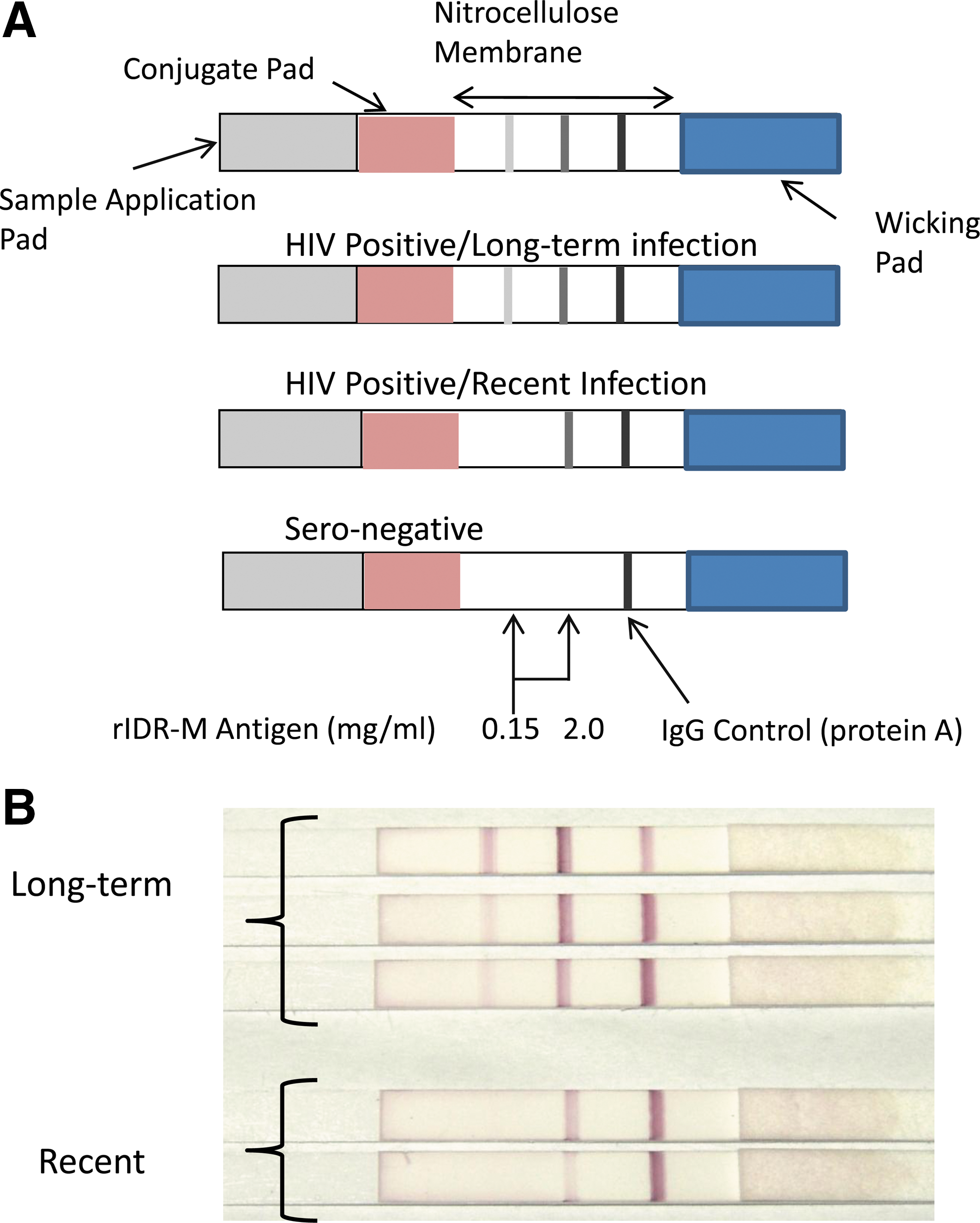
Schematic diagram of the rapid I-P assay including interpretative criteria.
The lateral flow assay was assembled in a standard configuration 21 on an adhesive card (Adhesives Research, Inc., Glen Rock, PA, MIBA-010, 80 mm×300 mm) that had been prescored for the application of the assay membrane, the upper wicking pad, the conjugate pad, and the sample pad. These assembled assay was cut into 5-mm strips that were stored desiccated (relative humidity <25%) prior to use.
Rapid I-P assay
For the final optimized assay, specimens were diluted 1:200 in sample buffer. The sample buffer consisted of 0.1 M sodium phosphate (Sigma-Aldrich), 0.15 M sodium chloride (Sigma-Aldrich), 10% chicken sera (Animal Technologies), 1% Triton X-100 (Sigma-Aldrich), 2% Tween 80 (Sigma-Aldrich), and 2% Tectronic 904 surfactant (BASF, Mt. Olive, NJ) (pH 7.2). Proclin 950 (0.3%) was added to the buffer as a preservative. The test strip was placed vertically into 3.5-ml polystyrene tubes (Sarstedt, Inc., Newton, NC) containing the diluted sample (200 μl) and allowed to react for 20 min at ambient temperature. Specimens were classified as long-term or recent based on the resulting line pattern observed on the strips (Fig. 2A). Specimens were classified as negative if they reacted only with the Protein A control line. Interpretation of recent and long-term infections is such that individuals with long-term infections have high antibody avidity that reacts with both the low and high rIDR-M antigen concentration lines, whereas those who are recently infected have weak avidity antibodies that react only with the high concentration rIDR-M line. At the end of the incubation period (20 min), the intensity of all of the lines was independently scored by two laboratorians using a sliding scale of barely visible (0.5+) to strongly reactive (4+; equivalent to the intensity of the Protein A control line). The score was 0.0 if no line was present.
HIV-1 BED incidence assay
The BED-CEIA was developed in our laboratory 4 and has been manufactured as a commercial kit since 2002. The assay was performed per the kit insert (Calypte Biomedical Corp, Portland, OR) to classify specimens as recent and long-term infections. The individuals classified as recently infected seroconverted within a mean time period of 162 days as described for subtype B with acquisition of infection within the last 6 months. 23
Results
Assay optimization
The rapid I-P test was optimized using Panel 1 (five-member panel, Fig. 2B). The critical parameter was concentration of the rIDR-M antigen (Ag) at the low Ag line, which was varied to get optimal separation (data not shown). The optimized rapid I-P test clearly distinguished the two recent and three long-term specimens in Panel 1 as shown in Fig. 2B. Three specimens with long-term infections had three lines including one at the low antigen concentration. Two specimens with recent infections displayed only two lines with no line present at the low antigen concentration.
The visual classifications of Panels 2 and 3 determined by the rapid I-P assay were compared to the results of the BED assay (Table 2), which identified 29 of the 62 specimens as recent and 33 as long-term. The rapid I-P data correlated well with the BED data with 21 of the 29 BED incident specimens having a line only at the higher rIDR-M concentration and being classified as recent. Five of the specimens were classified as long-term infections by the rapid I-P test with weak reactions at the incidence line. The remaining three samples did not react with rIDRm lines at both concentrations because they were very recent seroconversions as previously noted. 13 All of the specimens identified as long-term infections by the BED assay (n=33) produced three lines on the rapid I-P test also indicating long-term infection.
The final classification was based on the interpretation shown in Fig. 2A. Three specimens that were antibody positive by third generation screening assay were recent by the BED but were nonreactive on the diagnostic line of the rapid I-P assay.
Diagnostic performance of the rapid I-P assay
All HIV-1 known cross-sectional antibody-reactive specimens (n=88) were detected by the diagnostic line of the rapid I-P test while none of the 100 HIV antibody-negative specimens was detected (data not shown). Sensitivity and specificity based on this limited sample set were both 100%. Assay sensitivity for the detection of early seroconversion was assessed using Panels 2 and 3 (Table 3). Of the 111 seroconversion panel specimens, 67 were positive for HIV-1 antibodies by the third generation enzyme immunoassays (EIAs) (Abbott AB rDNA HIV-1/2 EIA and the Bio-Rad HIV-1/HIV-2 + O EIA) that use an antibody sandwich detection format. The rapid I-P test, formatted as an indirect immunoassay, was less sensitive than the third generation EIAs and detected 57 of these specimens. However, six of the 15 panels were detected earlier by the rapid I-P test than by HIV-1 WB positivity, which identified 45 of the specimens as HIV-1 antibody reactive. Detection of emerging antibody patterns in the low titer panels was also good with 23 of the 30 samples detected at the diagnostic line. Although all of these specimens were from infected individuals as determined by testing from later collections, three were antibody negative by third-generation EIAs and four were indeterminate by WB at the time of collection. These seven were not detected by the rapid I-P test and were reactive only by tests that indicated their early infection status (manufacturer's product insert).
First-generation HIV-1 antibody detection assay.
Originally marketed as the Genetic Systems HIV-1/HIV-2 peptide EIA; second generation test.
Abbott third-generation HIV-1/HIV-2 antibody detection assay.
WB, western blot; NA, data not available.
Determination of incident HIV infections using the rapid I-P assay
The cross-sectional HIV-1 antibody-positive specimens (n=88) were tested by the rapid I-P test and were compared to the BED EIA test results (Table 4). Seventy-one of the specimens were identified as long-term HIV infections by both the BED assay and by the rapid I-P test while nine were concordantly classified as recent. The remaining eight specimens were discordant with four being identified as recent by BED and long-term by rapid I-P, and four recent by rapid I-P and long-term by BED. All of the antibody-reactive members of the seroconversion panels (n=57) and of the low-titer panels (n=23) were identified as recent by the rapid I-P assay and by the BED assay.
The final classification was based on the interpretation shown in Fig. 2A.
The combination of all results from HIV antibody-positive specimens that were tested by both assays is shown in the scatter plot of Fig. 3 and includes the cross-sectional specimens (Panel 5, n=88), specimens from Panel 4 (seroconversion panels, n=57, and the low-titer panels, n=23), and the rapid I-P-reactive specimens from Panel 3 (n=37) (Total n=205). All of the rapid I-P test results were independently scored by two laboratorians and no discrepancies were noted. The two lines represent the cut-offs for each assay (no observable line for the rapid I-P test and 0.800 OD-n for the BED-EIA). The results clustered into the lower left quadrant for congruent incident specimens and into the upper right quadrant for congruent long-term infections. Agreement of incident versus long-term classification by the two assays was 95.1% with an excellent kappa statistic of 0.910 (95% CI 0.843–0.961). Four of the discordant specimens were classified as recent infections by the rapid I-P test but were identified as long-term infections by the BED assay (range ODn, 0.991–1.627). The remaining six discordant specimens were the reverse being classified as incident infections by the BED assay (range ODn, 0.306–0.751) and as long-term infections by the rapid I-P test (incident line score of 0.5–1.0).
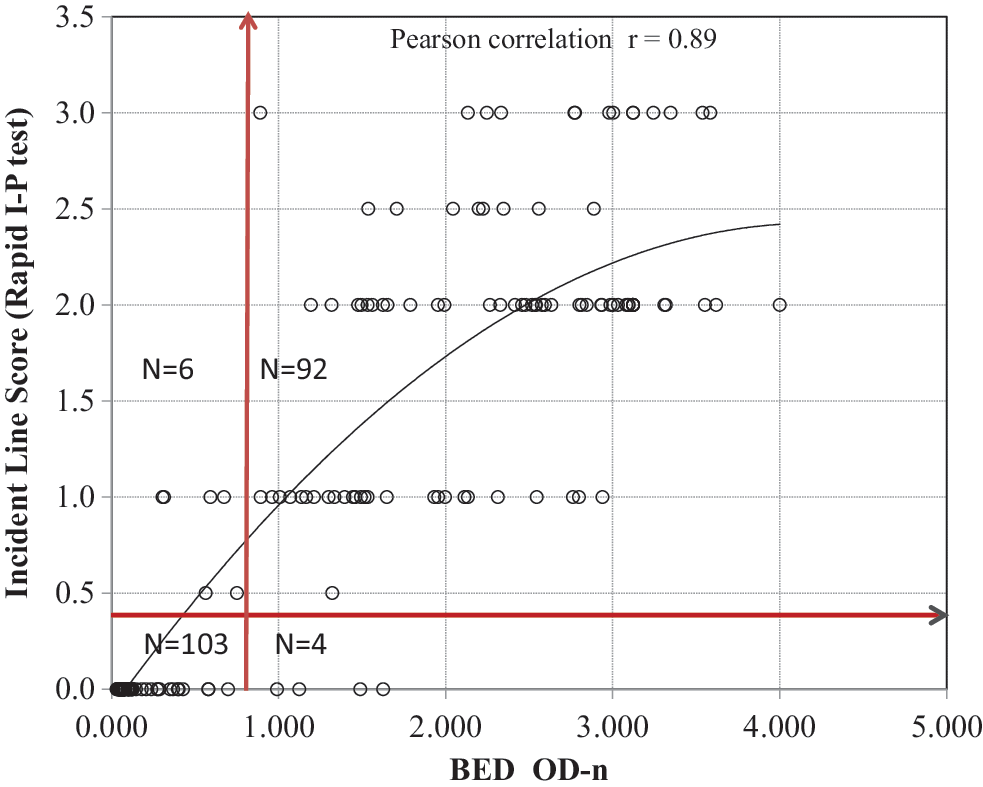
Concordance plot of the BED OD-n and the intensity score of the incidence line (0 to 4) on the rapid I-P assay using known specimens with recent and long-term infections (n=205). Score of 0=recent infection with rapid I-P assay. The vertical red line indicates a BED OD-n cutoff of 0.8 and the horizontal red line indicates the cutoff separating recent (score=0) and LT (score >0.5) infections for the rapid I-P assay. A 2×2 table on the right shows agreement between the two assays in classifying recent and LT infections with kappa statistics. Agreement between the two assays: 195/205=95.1%. Kappa statistic=0.910.
Discussion
In the past decade, several laboratory-based methods have been devised to identify HIV incident infections, most of which are based on the emerging antibody response. 24 The use of antibody titers, 1,25 the increasing proportion of HIV-specific antibody, 4 and antibody avidity 11,12,26 have all been applied to HIV incidence measurements with varying success. Modification of commercial assays may have limited applications outside the United States and Europe where the non-B subtypes are widely prevalent. 2,3 Although the BED assay was developed with the intent of providing similar performance among divergent subtypes and global populations, recent results show that recency periods were longer in African than in non-African cohorts, possibly because total IgG levels are higher in African populations. 23 The single-well rIDR-M-based limiting-antigen avidity assay that was recently developed was formatted to eliminate the effects of host IgG levels. 14 The approach described here is based on the same principle (limiting-antigen) but is adapted to a rapid, lateral flow platform.
The findings of Wei et al. 13 demonstrated that limiting the amount of available antigen in the single-well avidity assay allowed for the simplified discrimination of recent from long-term infections without the use of dissociation reagents (e.g., diethyl amine, urea, guanidine, or low pH buffer) that are commonly used to dissociate low avidity antibodies. The rapid I-P test was also able to differentiate recent and long-term HIV infections using the limiting antigen approach. In this case, rIDR-M was used for both the diagnostic and incidence lines for simplicity and with the knowledge that rIDR-M was designed to determine incidence and is not optimal for HIV diagnosis. As previously reported, 13 the EIA using rIDR-M as a diagnostic antigen had a sensitivity of approximately 97.5%. The specimens that were missed came from individuals with very recent HIV infections who had not yet developed antibodies to gp41. The rapid I-P test described here was developed to show the conceptual feasibility of a rapid test that can provide both prevalence and incidence determinations, but such a test will require a prudent choice of antigen for the diagnostic line. Ideally, the rIDR-M antigen at a low but optimized concentration could be added to existing HIV rapid tests with established sensitivity and specificity of >99%. Related rapid HIV testing work in our laboratory has characterized the use of multibranched peptides (MBP) that could be used as a diagnostic antigen 27 for HIV-1 antibodies with high sensitivity and specificity. Replacement of the rIDR-M antigen in the diagnostic line with one of these MBPs is in progress.
Current laboratory methods for incidence estimation require collection and transportation of specimens to central laboratories where the testing is usually performed. This is expensive and logistically challenging, and carries the additional costs of sample storage (freezers), testing equipment, and the test kits needed to perform the testing. The rapid I-P test described here has significant potential to simplify HIV surveillance in a very cost-effective manner, especially in resource-limited settings. As more surveillance activities include rural populations and home-based testing, the rapid I-P test is ideally suited to provide data not only for HIV prevalence but also for incidence without the need for additional sample processing and transportation. Although the current study was performed with stored serum or plasma, the method could easily be adapted for testing whole blood collected from a finger prick.
There are several distinct advantages to the use of the rapid I-P assay. The test is simple to perform, does not require highly trained personnel, and requires only 1 μl of specimen. The lateral flow platform uses currently available materials and reagents, and can be produced in large quantities using existing manufacturing processes and vendors. Currently available HIV lateral-flow tests have already been shown to have excellent stability and reproducibility 28,29 and these characteristics would be expected to be similar for the rapid I-P test described here.
The primary use for the rapid I-P test would still be population-based surveillance, and the incidence status determined by the assay would not be reported to individuals. However, considering the impact on prevention, additional data should be generated to validate the accuracy of recent detection of infection using the rapid I-P test. Accurate identification of recent HIV infections would enhance targeted prevention efforts in high-risk groups through intensive counseling, early treatment, and other intervention measures to prevent further transmission. The rapid I-P assay could be a valuable tool for such an effort.
The data presented here demonstrate the conceptual use of a rapid I-P test for the first time with recognition that more work is needed to include longitudinal specimens representing different subtypes from both recently infected individuals and those with infection for more than 1 year. More work is also needed to establish the mean recency period 4,23 and to determine false recent rates among individuals infected for a long-term. 10,30 Recent development of low-cost, accurate reflectance readers 31 could assist with these determinations by eliminating the subjective interpretation of the assay results. These quantitative measurements could assist with the setting of assay cut-offs that could identify recent HIV infections and thus help to establish the appropriate recency period. Quantitative measurements of the rapid I-P assay results using these readers are in progress.
Footnotes
Acknowledgments
We appreciate the technical assistance of Krystin Ambrose and John Hart. We thank Michele Owen and Steve McDougal for commentary and technical discussions, and for reviewing the manuscript.
Author Disclosure Statement
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention or the U.S. Department of Health and Human Services. The use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
One of the authors (BSP) receives royalties from the sale of the HIV-1 BED Incidence assay as per policies of the U.S. government. No other financial disclosures were reported.