
Abstract
Whether response to combination antiretroviral therapy (cART) differs between those infected with HIV-1 subtype A or B remains unclear. We compared virological and immunological response to cART in individuals infected with subtype A or B in an ethnically homogeneous population. Data derived from the Athens Multicenter AIDS Cohort Study (AMACS) and analysis were restricted to those of Greek origin. Time to virological response (confirmed HIV-RNA <500 copies/ml) and time to failure (>500 copies/ml at any time or no response by month 6) were analyzed using survival models and CD4 changes after cART initiation using piecewise linear mixed effects models. Of the 571 subjects included in the analysis, 412 (72.2%) were infected with subtype B and 159 (27.8%) with subtype A. After adjusting for various prognostic factors, the rate of virological response was higher for those infected with subtype A versus B (adjusted HR: 1.35; 95% CI: 1.08–1.68; p=0.009). Subtype A was also marginally associated with a lower hazard of virological failure compared to subtype B (HR=0.73; 95% CI: 0.53–1.02; p=0.062). Further adjustment for treatment adherence did not substantially changed the main results. No significant differences were observed in the rates of CD4 increases by subtype. The overall median (95% CI) CD4 increase at 2 years of cART was 193 (175, 212) cells/μl. Our study, based on one of the largest homogeneous groups of subtype A and B infections in Europe, showed that individuals infected with subtype A had an improved virological but similar immunological response to cART compared to those infected with subtype B.
Introduction
H
Monitoring the HIV-1 genetic heterogeneity is important for epidemiological reasons, since it can provide estimates about the origin and the patterns of the spread of an epidemic in a region. 6 –10 Moreover, HIV global surveillance is important for diagnosis, assay development, and prevention. 11,12 Given the increasing genetic heterogeneity of the virus globally, it is important to examine potential differences in virological and immunological response to combination antiretroviral therapy (cART) across different subtypes. Most of the clinical trials assessing the efficacy of antiretroviral drugs have been conducted in developed countries enrolling patients mainly infected with subtype B. Therefore it is of high clinical relevance to examine potential differences in the efficacy of cART among patients infected with non-B clades or different recombinant forms versus subtype B. Although this seems straightforward, given the large variability in HIV-1 subtype distribution by geographic area and/or ethnicity with subtype B prevailing in the Western countries, cohorts also including non-B infections are scarce. Until now a number of studies examined potential differences in the response to treatment across different subtypes in European or American cohorts, but in almost all cases non-B infections were mainly among African heterosexuals, whereas subtype B was detected in white men having sex with other men (MSM), making adjustment for ethnicity group difficult if not impossible. 13 –23 Moreover, most previous studies addressing this question had the serious, but because of the small numbers necessary, limitation of grouping all non-B subtypes together. 13,15,16,20 –23 Thus, the question of whether non-B subtypes correlate with different response rates to cART in an ethnically homogeneous population remains unresolved.
In Greece, a monophyletic HIV-1 subtype A epidemic has been identified. 24 The prevalence of HIV-1 subtype A among recently infected individuals eventually surpassed that of subtype B in recent years. The cocirculation of both, A and B, subtypes among the local population in Greece provided us with a unique opportunity to assess whether virological or immunological response to cART differs between these two HIV-1 clades. To our knowledge, this is the first study in Europe to address this question in an ethnically homogeneous cohort.
Materials and Methods
Study population
Data were derived from the Athens Multicenter AIDS Cohort Study (AMACS), a collaborative open, ongoing, population-based study initiated in 1996. All HIV-1-positive individuals seen in one of the 10 collaborating infectious diseases units located in the greater Athens area are included in the AMACS. Clinical records data are entered into electronic databases by trained staff in each center. Quality control is conducted through multiple data checks and resolution of discrepancies via queries. Individuals are followed-up at the time of their clinical appointments, usually every 3 to 4 months. Death is ascertained though medical records review. A standardized protocol is used for data collection. A variety of data are recorded, including demographic characteristics, clinical events and deaths, antiretroviral therapy history, laboratory tests, and HIV-1 subtype and resistance tests results (if available).
Data are provided by the clinics anonymously. The study protocol was reviewed and approved by the Bioethics and Deontology Committee of Athens University Medical School, the National Organization for Medicines, and by each participating Unit Hospital's Scientific Committee.
cART was defined as a regimen of three or more antiretroviral drugs consisting of two nucleos(t)ide reverse transcriptase inhibitors (NRTIs) plus one or more protease inhibitors (PIs), or one nonnucleoside reverse transcriptase inhibitor (NNRTI), or an integrase (IN), or an entry inhibitor (EI), or three NRTIs including abacavir or tenofovir. 25 Prior exposure to mono or dual antiretroviral therapy was allowed. Eligible individuals were of Greek origin, started a stable first line cART (i.e., at least 2 months), who had CD4 counts and HIV-RNA measurement available both at baseline (i.e., within 6 months prior to cART initiation) and while on their first cART regimen. Ethnic group was based on self-reported ethnicity. Compliance to cART was also self-reported. Individuals were classified as compliers if they reported having received at least 95% of their drug doses. Follow-up was censored at the first major treatment modification (i.e., change of cornerstone drug or simultaneous change of at least two backbone drugs) or at treatment interruption lasting for more than 2 months.
For those with detectable baseline viral load, virological response was defined as the time to a confirmed decrease in HIV-RNA below 500 copies/ml, considered to occur at the midpoint between the last detectable and first undetectable viral load. Virological failure was defined as the time to virological rebound (i.e., confirmed increase in HIV-RNA above 500 copies/ml; single blips in HIV-RNA between 500 and 1000 copies/ml were allowed) for those who achieved undetectability while on cART or those who had undetectable baseline viral load, or to 6 months for those not responding by that time. As the cut-off of the early assays used in our study was 500 copies/ml, this value was used uniformly as the HIV-RNA detectable limit.
HIV-1 subtype classification
HIV-1 subtypes were determined by phylogenetic analysis in partial protease (PR) and partial reverse transcriptase (RT) regions. Specifically, PR and partial RT sequences were aligned against HIV-1 reference sequences, including all previously described subtypes and major CRFs available from
Statistical methods
Cumulative incidences of virological response and failure were estimated through the nonparametric Aalen–Johansen estimator, to account for the competing event of switching to a new cART regimen. 27 Cause-specific hazards of response and failure were analyzed using the Cox proportional hazards model. 28 CD4 changes after cART initiation were analyzed based on a piecewise linear mixed effects model, with change in slope at 6 months. The following covariates were considered as potential confounders in all multivariable analyses: age at cART initiation (<35 or ≥35 years), gender, transmission group [MSM, men having sex with woman (MSW), other/unknown], calendar year of cART initiation (1996–1997, 1998–1999, and ≥2000), first line cART regimen (unboosted PI, boosted PI, other), pre-cART antiretroviral experience (naive, experienced), previous AIDS diagnosis, and coinfection with hepatitis B or C virus (HBV or HCV) (yes, no, unknown).
A set of sensitivity analyses was carried out to adjust for the potential confounding effect of treatment adherence and final models were further adjusted for compliance, and analyses were restricted to those who started cART at or after 2000, when boosted PIs came to be in common use.
Results
Baseline characteristics of the study population
The AMACS database, updated in 2011, included data from 3,414 HIV-1-infected individuals of whom 1,384 initiated cART during the follow-up. Of these, we excluded 459 who were of non-Greek origin and 645 without HIV-RNA and/or CD4 measurements at cART initiation or while on cART. Of the 1,384 eligible individuals, HIV-1 subtype was known for 649 (46.9%). Those with known HIV-1 subtype were on average more likely to have been exposed to pre-cART antiretrovirals and to have higher baseline viremia levels.
Among the 659 individuals with known HIV-1 subtypes, the predominant subtypes were B in 412 (63.5%), A in 159 (24.5%), C in 13 (2%), F1 in 3, G in 2, and D in 1, whereas 59 (9.1%) were infected with recombinant viruses (7 CRF02_AG, 4 CRF01_AE, 4 CRF04_cpx, and 44 with various URFs). As our main aim was to compare subtype B with subtype A, we further excluded all individuals infected with any subtype other than A or B. The baseline characteristics (i.e., at cART initiation) of the 571 remaining individuals by HIV-1 subtype are shown in Table 1. In total, 171 (30.0%) of the study population had been exposed to previous non-cARTs [69 (40.4%) one regimen, 43 (25.1%) two regimens, and 59 (34.5%) more than two previous regimens].
Compliance was self-reported. Compliers were considered those who had reported receiving at least 95% of their drug doses.
MSM, men having sex with men; MSW, Men having sex with women; cART, combination antiretroviral therapy; PI, protease inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; HBV, hepatitis B virus; HCV, hepatitis C virus.
Compared to those infected with subtype B, those infected with subtype A were more likely to be older, infected through MSW, AIDS-free, ART naive, initiate cART at later calendar years, and thus use boosted-PI based regimens and less likely to be HCV or HBV coinfected. Compliance with cART was known for 72.9% and 75.7% of those infected with subtype A or B, respectively. Individuals infected with subtype A were more likely to be treatment compliers that those infected with subtype B.
The analysis of time to virological response/failure may be sensitive to the timing of viral load measurements; if patients with a particular subtype had more distant viral load measurements, they would be artificially considered to have experienced virological response/failure at later times and thus to have lower rates of virological response. Therefore we compared median follow-up time, number of HIV-RNA measurements, and median time interval between consecutive measurements between subtypes. There were no significant differences (p>0.325in all cases).
Virological response/failure
Virologic response
Of the 571 individuals included in the analysis, 44 (13 with HIV-1 subtype A and 31 with subtype B) had undetectable baseline viremia. Among those with detectable baseline viral load, 380 (72.1%) experienced virological response with the cumulative incidence (95% CI) being 65.4% (61.1–69.3%) at 6 months after cART initiation.
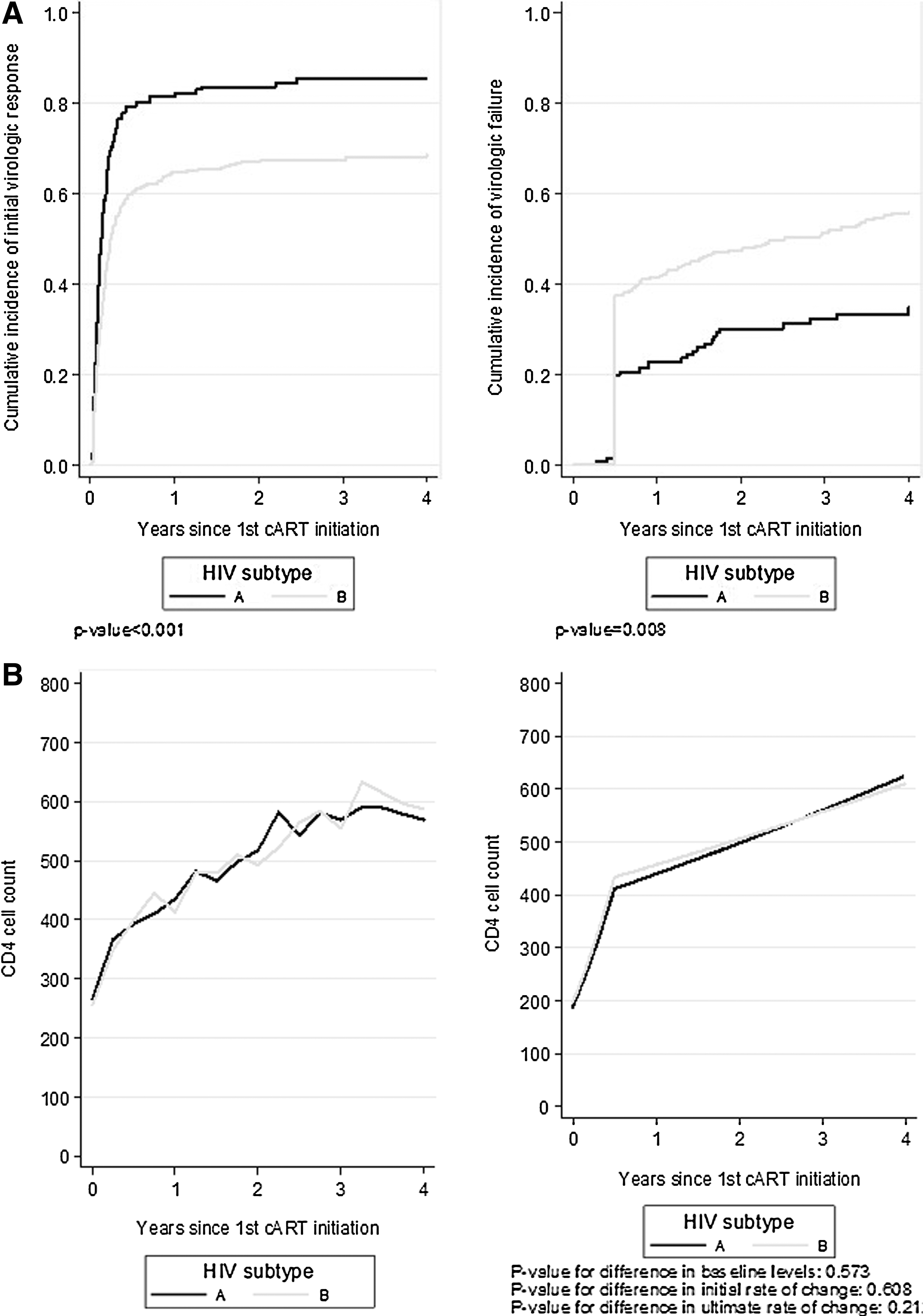
The unadjusted cumulative incidence of virological response differed significantly by HIV-1 subtype, being higher in those infected with subtype A compared to those infected with subtype B (p<0.001; Fig. 1A). The cumulative incidence of virological response (95% CI) was 79.3% (71.7–85.1%) and 60.1% (55.0–64.8%) for individuals infected with subtypes A and B, respectively, after 6 months of cART and 81.5% (74.1–86.9%) and 64.6% (59.5–69.2%) after 12 months of cART. The difference between the two subtypes persisted in multivariable analysis [adjusted HR of A/B: 1.35, 95% CI: (1.08–1.68), p=0.009; Table 2]. Those who initiated cART at earlier calendar periods, were ART experienced at cART initiation, and were on unboosted PIs had lower rates of virological response (Table 2).
The HIV-1 subtype effect persisted even after further adjustment for compliance to cART [adjusted HR (95% CI) for A/B 1.33 (1.06–1.66), p=0.012]. Restricting the analysis to those who initiated cART at or after 2000 did not substantially alter the results regarding HIV-1 subtype effect [adjusted HR for A/B (95% CI): 1.37(1.07–1.76), p=0.012].
Virologic failure
Of the 571 study participants, 41 had less than 180 days of follow-up after cART initiation and were excluded from the analysis of virological failure. Of the 530 remaining individuals, 91 (17.2%) experienced a virological rebound and 167 (31.5%) did not respond by 6 months. The cumulative incidence of virological failure differed significantly by HIV-1 subtype being lower in those infected with subtype A compared to those infected with subtype B (p=0.008; Fig. 1B). The results from the multivariable cause-specific proportional hazards model are shown in Table 2. Subtype A was associated with a lower hazard of virological failure compared to subtype B [adjusted HR for A/B (95% CI): 0.73 (0.53–1.02), p=0.062], although the difference was only marginally significant. Those who initiated cART at earlier calendar periods, were ART experienced at cART initiation, and were on an unboosted PI regimen had higher rates of virological failure (Table 2).
Further adjustment for compliance to cART did not substantially change the estimated effect of HIV-1 subtype (HR=0.77, p=0.117). Restricting the analysis to those infected at or after 2000 yielded a statistically significant result for HIV-1 subtype effect [adjusted HR (95% CI) for A/B: 0.60 (0.36–0.98), p=0.041].
Immunological response
Cross-sectional medians of CD4 counts by time since cART initiation and HIV-1 subtype are shown in Fig. 1B (left part). However, this plot should be interpreted with caution as it is subject to biases due to missing visits (i.e., different number of subjects contribute at different time points). CD4 increases followed a bilinear trend with steeper increases during the first 6 months after cART initiation followed by less steep increases thereafter. Both unadjusted and adjusted mixed effects models showed no significant differences in baseline CD4 counts and initial (i.e., during the first 6 months on cART) or long-term (i.e., after 6 months on cART) CD4 increases by HIV-1 subtype. Rates of initial CD4 increases were slower in older individuals, in those who initiated cART at earlier calendar periods, and in those who were ART experienced, on unboosted PIs, coinfected with HBV or HCV, without AIDS history, or with high viremia, whereas long-term rates of CD4 increases were lower in women and in ART-experienced subjects.
Using as the reference population MSMs of a mean age, initiating a boosted PI regimen after 2000, without prior ART or AIDS experience, with no HCV or HBV coinfection, and with median baseline HIV-RNA, the estimated median (95% CI) CD4 counts at cART initiation were 189 (153–225) and 197 (166–229) for those infected with subtype A or B, respectively (p=0.573). The overall median (95% CI) CD4 increase for the reference population at 6 months after cART initiation was 232 (200–265), and was 223 (183–263) and 236 (202–271) for those infected with subtype A or B, respectively (p=0.438). The overall mean (95% CI) rate of CD4 increase after 6 months on cART was, on the square root scale, 0.576, being significantly different from zero (p<0.001). The adjusted estimated median CD4 counts by time after cART initiation and HIV-1 subtype are shown in Fig. 1B (right panel). Sensitivity analyses as mentioned earlier yielded results consistent with those of the main analysis results.
Clinical progression
Of the 571 study subjects, 25 developed a new or recurrent (eight recurrences) AIDS event during 1568.3 prys of follow-up after cART initiation resulting in an overall mean (95% CI) rate of 1.59 (1.08–2.35) AIDS events/100 prys, being 0.92 (0.35–2.46) and 1.85 (1.21–2.84) for those infected with subtype A and B, respectively (the difference not being statistically significant; p=0.202). The main AIDS diagnoses were pulmonary infection by Mycobacterium tuberculosis (n=5, 20%), Kaposi sarcoma (n=4, 16%), and progressive multilocus leukoencephalopathy (n=4, 16%).
Discussion
With cART becoming widely available worldwide, ensuring that cART is equally active against all HIV-1 subtypes becomes very important. HIV-1 subtype A, in particular, is the second most prevalent subtype globally. 2 Thus comparing responses to cART between those infected with subtype A and subtype B is highly relevant.
Most of the previous studies have reported no significant differences in virological response to cART in those infected with B or non-B subtypes, 13,15,16 21 –23,29 but all non-B subtypes were grouped together 13,15,16,21 –23,29,30 (Table 3). However, Atlas et al. showed that different ethnicity rather than genetic subtype was associated with significant differences in response to cART and that CD4+ cell increase was more pronounced for CRF01_AE and B versus subtype A. 19 Moreover, Easterbrook et al. reported higher rates of virological rebound for subtype D versus B-infected individuals; in contrast, subtype A was associated with a reduced risk of viral rebound than subtype B cases. 18 However, Geretti et al. reported that viral load suppression occurred more rapidly in individuals infected with subtype A or C compared to those infected with subtype B. 17 In this study though, as in most studies conducted in Western countries, non-B subtypes mainly circulated among heterosexual black African men and subtype B among MSM. 17 Therefore, adjustment for ethnicity and/or transmission group was not possible. This was an important limitation, also taking into account results from other studies suggesting that ethnicity rather than subtype influences responses to cART. 15
In our study, we compared responses to cART therapy in individuals infected with subtype A or B of Greek origin and we found that for those infected with subtype A, HIV-RNA declined faster and they had lower rates of virological failure compared to those infected with subtype B. There were no significant differences though in the rates of CD4 increases after cART initiation by HIV-1 subtype. To our knowledge, this is one of the first studies to compare subtype A with subtype B in an ethnically homogeneous population. Moreover, we estimated treatment effect in individuals infected with subtype A strains belonging to a monophyletic cluster. 24 That is, our study focused on a particular subclade within subtype A circulated in Greece and also spreading in Albania, 24 suggesting that subtype A was less divergent than B in this specific population. Whether results can be generalized to overall subtype A infections or they are a specific biological property of the Greek monophyletic lineage remains to be answered. Our results are compatible with those reported recently from the Swiss HIV Cohort study. 30 In this study, restricting the analysis to whites only, it was found that individuals infected with non-B subtypes had lower rates of virological failure compared to those infected with subtype B. In particular, subtypes A and CRF02_AG had improved outcomes. 30 On the other hand, most previous studies have not reported significant differences in rates of CD4 increase after cART initiation by HIV-1 subtype. 13,15 –18,21,22
It is known that boosted PIs are more effective than unboosted PI-based regimens. In our study, those infected with subtype B were more likely to have initiated cART at earlier calendar periods and to be on unboosted PI-based regimens than those infected with subtype A. In the main analysis we had adjusted for cART regimen. However, to exclude residual confounding, we restricted the analysis to those who started cART at or later than 2000 and results were consistent with those of the main analysis. Another factor affecting virological response to cART is treatment adherence. In our study, adherence was higher in those infected with subtype A compared to those infected with subtype B, most likely because the former group started antiretroviral therapy at later calendar periods when less toxic and easier to receive regimens were available. However, results were robust to adherence adjustment. Availability of adherence data and including them in a sensitivity analysis are advantages of our study.
An interesting question is whether response to cART correlates with replicative capacity for different HIV-1 subtypes or recombinant viruses. Previous studies suggested that subtype C has a lower replicative fitness than all the other subtypes and this could be associated with a longer infectivity period in subtype C-infected individuals. 31,32 These findings are associated with recently published results that HIV RNA persists at high levels after acute infection for subtype C. 33 On the other hand, CRF02_AG was found to be more fit than parental subtypes A and G, 31 but no differences were observed in survival or clinical disease rates between patients infected with CRF02_AG or non-CRF02_AG viruses. 34,35 In another study, differences in progression to death were reported for subjects infected with recombinant viruses or multiple subtypes when compared to those infected with subtype A. 36 While most previous studies support the hypothesis of subtype C being less fit than the other subtypes, the overall results regarding differences in fitness or natural history between subjects infected with different subtypes or recombinants remain contradictory, suggesting that further studies, optimally in seroconverters, are needed to address this issue. As a result, our finding of a better virological response in those infected with subtype A compared to those infected with subtype B cannot be consistent with data on the biological properties of the different subtypes.
Our findings of better virological responses in subtype A compared to subtype B infections could be at least partly explained by potential HIV-1 clade-specific differences in factors influencing viral replication. As suggested previously, viral load set point can be affected by genetic characteristics of the virus that are distinct for both subtypes A and C compared to others. 37 However, further documentation is needed before we hypothesize that differences found in our study could be explained by the latter findings. Another potential reason for the observed differences in the time to virological response could be that subtype B infections might have higher levels of transmitted drug resistance (TDR). Although there is no information about baseline resistance levels for this population, in a previous study from our group we have found that TDR levels were similar between subtype B-infected and subtype A-infected individuals, 38 suggesting that differences in virological response, probably, are unlikely to be explained by TDR.
In conclusion, in this study, restricting the analysis to an ethnically homogeneous population, with the highest representation of subtype A infection to date, and adjusting for most known cofactors, including treatment adherence, we have shown that those infected with subtype A had better virological but similar immunological responses to cART compared to those infected with subtype B. These findings are important as they reassure us that current antiretroviral regimens when administered to individuals with subtype A infection have equal, if not better, efficacy as when they are administered to individuals with subtype B infection.
Footnotes
Acknowledgments
The study was supported in part by the Hellenic Center for Disease Control and Prevention.
Members of the AMACS:
Author Disclosure Statement
No competing financial interests exist.